Arrhythmology.narod.ru
ACC/AHA/ESC Practice Guidelines
ACC/AHA/ESC Guidelines for the Management of Patients
With Supraventricular Arrhythmias*—Executive Summary
A Report of the American College of Cardiology/American Heart Association
Task Force on Practice Guidelines and the European Society of Cardiology
Committee for Practice Guidelines (Writing Committee to Develop Guidelines
for the Management of Patients With Supraventricular Arrhythmias)
Developed in Collaboration with NASPE-Heart Rhythm Society
Committee Members
Carina Blomström-Lundqvist, MD, PHD, FACC, FESC, Co-chair; Melvin M. Scheinman, MD, FACC, Co-chair;
Etienne M. Aliot, MD, FACC, FESC; Joseph S. Alpert, MD, FACC, FAHA, FESC;
Hugh Calkins, MD, FACC, FAHA; A. John Camm, MD, FACC, FAHA, FESC;
W. Barton Campbell, MD, FACC, FAHA; David E. Haines, MD, FACC; Karl H. Kuck, MD, FACC, FESC;
Bruce B. Lerman, MD, FACC; D. Douglas Miller, MD, CM, FACC; Charlie Willard Shaeffer, Jr, MD, FACC;
William G. Stevenson, MD, FACC; Gordon F. Tomaselli, MD, FACC, FAHA
Task Force Members
Elliott M. Antman, MD, FACC, FAHA, Chair; Sidney C. Smith, Jr, MD, FACC, FAHA, FESC, Vice-Chair;
Joseph S. Alpert, MD, FACC, FAHA, FESC; David P. Faxon, MD, FACC, FAHA;
Valentin Fuster, MD, PhD, FACC, FAHA, FESC;
Raymond J. Gibbons, MD, FACC, FAHA†‡; Gabriel Gregoratos, MD, FACC, FAHA;
Loren F. Hiratzka, MD, FACC, FAHA; Sharon Ann Hunt, MD, FACC, FAHA;
Alice K. Jacobs, MD, FACC, FAHA; Richard O. Russell, Jr, MD, FACC, FAHA†
ESC Committee for Practice Guidelines Members
Silvia G. Priori, MD, PhD, FESC, Chair; Jean-Jacques Blanc, MD, PhD, FESC; Andzrej Budaj, MD, FESC;
Enrique Fernandez Burgos, MD; Martin Cowie, MD, PhD, FESC; Jaap Willem Deckers, MD, PhD, FESC;
Maria Angeles Alonso Garcia, MD, FESC; Werner W. Klein, MD, FACC, FESC‡; John Lekakis, MD, FESC;
Bertil Lindahl, MD; Gianfranco Mazzotta, MD, FESC; João Carlos Araujo Morais, MD, FESC;
Ali Oto, MD, FACC, FESC; Otto Smiseth, MD, PhD, FESC; Hans-Joachim Trappe, MD, PhD, FESC
*This document does not cover atrial fibrillation; atrial fibrillation is covered in the ACC/AHA/ESC guidelines on the management of patients with
atrial fibrillation found on the ACC, AHA, and ESC Web sites.
†Former Task Force Member‡Immediate Past ChairThis document was approved by the American College of Cardiology Foundation Board of Trustees in August 2003, by the American Heart Association
Science Advisory and Coordinating Committee in July 2003, and by the European Society of Cardiology Committee for Practice Guidelines in July 2003.
When citing this document, the American College of Cardiology Foundation, the American Heart Association, and the European Society of Cardiology
request that the following citation format be used: Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB,Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF. ACC/AHA/ESC guidelines for the management of patientswith supraventricular arrhythmias— executive summary: a report of the American College of Cardiology/American Heart Association Task Force onPractice Guidelines, and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for theManagement of Patients With Supraventricular Arrhythmias.). J Am Coll Cardiol 2003;42:1493–531.
This document is available on the World Wide Web sites of the American College of Cardiology (www.acc.org), the American Heart Association
(www.americanheart.org), and the European Society of Cardiology (www.escardio.org), as well as published in the October 15, 2003, issue of the
Journalof the American College of Cardiology, the October 14, 2003, issue of
Circulation, and the 24/20 October 15, 2003, issue of the
European Heart Journal.
Single and bulk reprints of both the full-text guidelines and the executive summary are available from Elsevier Publishers by calling ⫹44.207.424.4200or ⫹44.207.424.4389, faxing ⫹44.207.424.4433, or writing to Elsevier Publishers Ltd,
European Heart Journal, ESC Guidelines—Reprints, 32Jamestown Road, London, NW1 7BY, UK; or E-mail
[email protected]. Single copies of executive summary and the full-text guidelines are alsoavailable by calling 800-253-4636 or writing the American College of Cardiology Foundation, Resource Center, at 9111 Old Georgetown Road, Bethesda,MD 20814-1699. To purchase bulk reprints (specify version and reprint number— executive summary 71-0261 and full-text guideline 71-0262): up to999 copies, call 800-611-6083 (U.S. only) or fax 413-665-2671; 1000 or more copies, call 214-706-1789, fax 214-691-6342; or
[email protected].
2003 by the American College of Cardiology Foundation, the American Heart Association, Inc., and the European Society of Cardiology
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Table of Contents
1. Acute Conversion of Atrioventricular Node–
Dependent Tachycardias . . . . . . . . 1522
2. Prophylactic Antiarrhythmic Drug Therapy .1523
A. Organization of Committee and Evidence Re-
B. Supraventricular Tachycardias in Adult
Patients With Congenital Heart Disease . . . 1523
B. Contents of these Guidelines—Scope . . . . 1495
II. Public Health Considerations and Epidemiology .1495
2. Specific Disorders . . . . . . . . . . .1524
III. General Mechanisms of Supraventricular Arrhythmia . 1496
C. Quality-of-Life and Cost Considerations . . .1525
A. Specialized Atrial Tissue . . . . . . . . . 1496
B. General Mechanisms . . . . . . . . . . .1496
IV. Clinical Presentation, General Evaluation, and
Management of Patients With Supraven-
These practice guidelines are intended to assist physicians in
tricular Arrhythmia . . . . . . . . . . . . . .1496
clinical decision making by describing a range of generally
A. General Evaluation of Patients Without
acceptable approaches for the diagnosis and management of
Documented Arrhythmia . . . . . . . . . 1496
supraventricular arrhythmias. These guidelines attempt to
1. Clinical History and Physical Examination .1496
define practices that meet the needs of most patients in most
2. Diagnostic Investigations . . . . . . . .1497
circumstances. The ultimate judgment regarding care of a
particular patient must be made by the physician and the
B. General Evaluation of Patients With
patient in light of all of the circumstances presented by that
Documented Arrhythmia . . . . . . . . . .1498
patient. There are situations in which deviations from these
1. Diagnostic Evaluation . . . . . . . . . 1498
guidelines are appropriate.
V. Specific Arrhythmias . . . . . . . . . . . . 1502
A. Sinus Tachyarrhythmias . . . . . . . . . 1502
A. Organization of Committee and
1. Physiological Sinus Tachycardia . . . . .1502
2. Inappropriate Sinus Tachycardia . . . . .1503
Supraventricular arrhythmias are a group of common rhythm
3. Postural Orthostatic Tachycardia Syndrome .1505
disturbances. The most common treatment strategies include
4. Sinus Node Re-Entry Tachycardia . . . . 1505
antiarrhythmic drug therapy and catheter ablation. Over the past
B. Atrioventricular Nodal Reciprocating Tachycardia .1506
decade, the latter has been shown to be a highly successful and
1. Definitions and Clinical Features . . . . .1506
often curative intervention. To facilitate and optimize the man-
agement of patients with supraventricular arrhythmias, the
3. Long-Term Pharmacologic Therapy . . . 1506
American College of Cardiology Foundation (ACCF), the
4. Catheter Ablation . . . . . . . . . . .1507
American Heart Association (AHA), and the European Society
C. Focal and Nonparoxysmal Junctional Tachycardia .1508
of Cardiology (ESC) created a committee to establish guidelines
1. Focal Junctional Tachycardia . . . . . . 1508
for better management of these heterogeneous tachyarrhythmias.
2. Nonparoxysmal Junctional Tachycardia . .1509
This document summarizes the management of patients with
D. Atrioventricular Reciprocating Tachycardia
supraventricular arrhythmias with recommendations for diag-
(Extra Nodal Accessory Pathways) . . . . . 1510
nostic procedures as well as indications for antiarrhythmic drugs
1. Sudden Death in WPW Syndrome and
and/or nonpharmacologic treatments.
Risk Stratification . . . . . . . . . . .1510
Writing groups are specifically charged to perform a
formal literature review, weigh the strength of evidence for or
3. Long-Term Pharmacologic Therapy . . . 1511
against a particular treatment or procedure, and include
4. Catheter Ablation . . . . . . . . . . .1512
estimates of expected health outcomes where data exist.
5. Management of Patients With Asymptomatic
Patient-specific modifiers, comorbidities, and issues of pa-
Accessory Pathways . . . . . . . . . .1513
tient preference that might influence the choice of particular
6. Summary of Management . . . . . . . 1513
tests or therapies are considered, as are frequency of
E. Focal Atrial Tachycardias . . . . . . . . .1513
follow-up and cost effectiveness. In controversial areas, or
1. Definition and Clinical Presentation . . . 1513
with regard to issues without evidence other than usual
clinical practice, a consensus was achieved by agreement of
3. Site of Origin and Mechanisms . . . . . 1514
the expert panel after thorough deliberations.
This document was peer reviewed by two official external
5. Multifocal Atrial Tachycardia . . . . . .1516
reviewers representing the American College of Cardiology
F. Macro–Re-entrant Atrial Tachycardia . . . . 1516
Foundation, two official external reviewers representing the
1. Isthmus-Dependent Atrial Flutter . . . . .1516
American Heart Association, and two official external re-
2. Non–Cavotricuspid Isthmus–Dependent
viewers representing the European Society of Cardiology.
The North American Society for Pacing and Electrophysiol-
VI. Special Circumstances . . . . . . . . . . . .1522
ogy—Heart Rhythm Society assigned one organizational
reviewer to the guideline. In addition, 37 external content
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
reviewers participated in the review representing the ACC/
tachycardia (AVNRT), atrioventricular reciprocating
AHA Task Force on Practice Guidelines, the ESC Committee
tachycardia (AVRT), and atrial tachycardia (AT).
for Practice Guidelines, the ACCF Electrophysiology Com-
Overall, this is a consensus document that includes evi-
mittee, the AHA ECG/Arrhythmias Committee, the ESC
dence and expert opinions from several countries. The phar-
Working Group on Arrhythmias, and the ESC Task Force on
macologic and nonpharmacologic antiarrhythmic approaches
Grown-Up Congenital Heart Disease. Please see Appendix 2
discussed may, therefore, include some drugs and devices
in the full-text guideline for the names of all reviewers.
that do not have the approval of governmental regulatory
The document was approved for publication by the gov-
agencies. Because antiarrhythmic drug dosages and drug
erning bodies of the ACCF, AHA, and ESC. These guidelines
half-lives are detailed in the ACC/AHA/ESC Guidelines for
will be reviewed annually by the ESC and the ACC/AHA
the Management of Patients With Atrial Fibrillation (1), they
Task Force on Practice Guidelines and will be considered
are not repeated in this document.
current unless they are revised or withdrawn fromdistribution.
II. Public Health Considerations
Recommendations are evidence-based and derived primar-
ily from published data. The level of evidence was ranked as
Supraventricular arrhythmias are relatively common, often
repetitive, occasionally persistent, and rarely life threatening.
The precipitants of supraventricular arrhythmias vary with
Level A (highest): derived from multiple randomized clinical
age, sex, and associated comorbidity (2).
Failure to discriminate among AF, atrial flutter, and other
Level B (intermediate): data are on the basis of a limited
supraventricular arrhythmias has complicated the precise
number of randomized trials, nonrandomized studies, or
definition of this arrhythmia in the general population. The
estimated prevalence of paroxysmal supraventricular
Level C (lowest): primary basis for the recommendation was
tachycardia (PSVT) in a 3.5% sample of medical records in
expert consensus.
the Marshfield (Wisconsin) Epidemiologic Study Area(MESA) was 2.25 per 1000 (3). The incidence of PSVT in
Recommendations follow the format of previous ACC/
this survey was 35 per 100 000 person-years (3).
AHA guidelines for classifying indications, summarizing
Age exerts an influence on the occurrence of SVT. The
both the evidence and expert opinion.
mean age at the time of PSVT onset in the MESA cohort was
Class I: Conditions for which there is evidence for and/or
57 years (ranging from infancy to more than 90 years old) (3).
general agreement that the procedure or treatment
In the MESA population, compared with those with other
is useful and effective.
cardiovascular disease, "lone" (no cardiac structural disease)
Class II: Conditions for which there is conflicting evidence
PSVT patients were younger (mean age equals 37 versus 69
and/or a divergence of opinion about the useful-
years), had faster heart rates (186 versus 155 beats per minute
ness/efficacy of a procedure or treatment.
[bpm]), and were more likely to present first to an emergency
Class IIa: The weight of evidence or opinion is
room (69% versus 30%) (3). The age of tachycardia onset is
in favor of the procedure or treatment.
higher for AVNRT (32 plus or minus 18 years) than for
Class IIb: Usefulness/efficacy is less well estab-
AVRT (23 plus or minus 14 years).
lished by evidence or opinion.
Gender plays a role in the epidemiology of SVT. Female
Class III: Conditions for which there is evidence and/or
residents in the MESA population had a twofold greater
general agreement that the procedure or treatment
relative risk (RR) of PSVT (RR equals 2.0; 95% confidence
is not useful/effective and in some cases may be
interval equals 1.0 to 4.2) compared with males (3).
The only reported epidemiologic study of patients with
atrial flutter (4) involved a selected sample of individuals
B. Contents of these Guidelines—Scope
treated in the Marshfield Clinic in predominantly white, rural
The purpose of this joint ACC/AHA/ESC document is to
mid-Wisconsin. More than 75% of the 58 820 residents and
provide clinicians with practical and authoritative guidelines
virtually all health events were included in this population
for the management and treatment of patients with supraven-
database. In approximately 60% of cases, atrial flutter oc-
tricular arrhythmias (SVA). These include rhythms emanat-
curred for the first time in association with a specific
ing from the sinus node, from atrial tissue (atrial flutter), and
precipitating event (ie, major surgery, pneumonia, or acute
from junctional as well as reciprocating or accessory path-
myocardial infarction). In the remaining patients, atrial flutter
way–mediated tachycardia. This document does not include
was associated with chronic comorbid conditions (ie, heart
recommendations for patients with either atrial fibrillation
failure, hypertension, and chronic lung disease). Only 1.7%
(AF) (see ACC/AHA/ESC Guidelines for the Management of
of cases had no structural cardiac disease or precipitating
Patients With Atrial Fibrillation (1)) or for pediatric patients
causes (lone atrial flutter). The overall incidence of atrial
with supraventricular arrhythmias. For our purposes, the term
flutter was 0.088%; 58% of these patients also had AF. Atrial
"supraventricular arrhythmia" refers to all types of supraven-
flutter alone was seen in 0.037%. The incidence of atrial
tricular arrhythmias, excluding AF, as opposed to SVT,
flutter increased markedly with age, from 5 per 100 000 of
which includes atrioventricular nodal reciprocating
those more than 50 years old to 587 per 100 000 over age 80.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Atrial flutter was 2.5 times more common in men and was
AV node allows for recovery of, and retrograde activation
diagnosed twice as often as PSVT.
over, the accessory pathway.
Re-entry is the mechanism of tachycardia in SVTs such as
III. General Mechanisms of SVA
AVRT, AVNRT and atrial flutter; however, a fixed obstacle
A. Specialized Atrial Tissue
and predetermined circuit are not essential requirements for
The sinoatrial node, atria, and atrioventricular (AV) node are
all forms of re-entry. In functionally determined re-entry,
heterogeneous structures. There is distinct electrophysiolog-
propagation occurs through relatively refractory tissue and
ical specialization of tissues and cells within these structures.
there is an absence of a fully excitable gap. Specific mecha-
In the case of the nodes, cellular heterogeneity is a prominent
nisms are considered in the following sections.
IV. Clinical Presentation, General Evaluation,
The sinoatrial node is a collection of morphologically and
electrically distinct cells (5,6). The central portion of the
and Management of Patients With SVA
sinus node, which houses the dominant pacemaking function,
A. General Evaluation of Patients Without
contains cells with longer action potentials and faster rates of
phase 4 diastolic depolarization than other cardiac cells (6,7).
1. Clinical History and Physical Examination
Cellular recordings support the existence of distinct popu-
Patients with paroxysmal arrhythmias are most often asymp-
lations of cells in the mammalian AV node. Differences in ion
tomatic at the time of evaluation. Arrhythmia-related symp-
channel expression underlie the differences in the electro-
toms include palpitations; fatigue; lightheadedness; chest
physiological behavior of each of the cell types.
discomfort; dyspnea; presyncope; or, more rarely, syncope.
A history of arrhythmia-related symptoms may yield impor-
B. General Mechanisms
tant clues to the type of arrhythmia. Premature beats are
All cardiac tachyarrhythmias are produced by one or more
commonly described as pauses or nonconducted beats followed
mechanisms, including disorders of impulse initiation and
by a sensation of a strong heart beat, or they are described as
abnormalities of impulse conduction. The former are often
irregularities in heart rhythm. Supraventricular tachycardias
referred to as automatic, and the latter as re-entrant. Tissues
occur in all age groups and may be associated with minimal
exhibiting abnormal automaticity that underlie SVT can
symptoms, such as palpitations, or they may present with
reside in the atria, the AV junction, or vessels that commu-
syncope. The clinician should distinguish whether the palpita-
nicate directly with the atria, such as the vena cava or
tions are regular or irregular. Irregular palpitations may be due to
pulmonary veins (8,9). The cells with enhanced automaticity
premature depolarizations, AF, or multifocal atrial tachycardia
exhibit enhanced diastolic phase 4 depolarization and, there-
(MAT). The latter are most commonly encountered in patients
fore, an increase in firing rate compared with pacemaker
with pulmonary disease. If the arrhythmia is recurrent and has
cells. If the firing rate of the ectopic focus exceeds that of the
abrupt onset and termination, then it is designated paroxysmal.
sinus node, then the sinus node can be overdriven and the
Sinus tachycardia is, conversely, nonparoxysmal and accelerates
ectopic focus will become the predominant pacemaker of the
and terminates gradually. Patients with sinus tachycardia may
heart. The rapid firing rate may be incessant (ie, more than
require evaluation for stressors, such as infection or volume loss.
50% of the day) or episodic.
Episodes of regular and paroxysmal palpitations with a sudden
Triggered activity is a tachycardia mechanism associated
onset and termination (also referred to as PSVT) most com-
with disturbances of recovery or repolarization. Triggered
monly result from AVRT or AVNRT. Termination by vagal
rhythms are generated by interruptions in repolarization of a
maneuvers further suggests a re-entrant tachycardia involving
heart cell called afterdepolarizations. An afterdepolarization
AV nodal tissue (eg, AVNRT, AVRT). Polyuria is caused by
of sufficient magnitude may reach "threshold" and trigger an
release of atrial natriuretic peptide in response to increased atrial
early action potential during repolarization.
pressures from contraction of atria against a closed AV valve,
The most common arrhythmia mechanism is re-entry,
which is supportive of a sustained supraventricular arrhythmia.
which may occur in different forms. In its simplest form, it
With SVT, syncope is observed in approximately 15% of
occurs as repetitive excitation of a region of the heart and is
patients, usually just after initiation of rapid SVT or with a
a result of conduction of an electrical impulse around a fixed
prolonged pause after abrupt termination of the tachycardia.
obstacle in a defined circuit. This is referred to as re-entrant
Syncope may be associated with AF with rapid conduction
tachycardia. There are several requirements for the initiation
over an accessory AV pathway or may suggest concomitant
and maintenance of this type of re-entry. Initiation of a circus
structural abnormalities, such as valvular aortic stenosis,
movement tachycardia requires unidirectional conduction
hypertrophic cardiomyopathy, or cerebrovascular disease.
block in one limb of a circuit. Unidirectional block may occur
Symptoms vary with the ventricular rate, underlying heart
as a result of acceleration of the heart rate or block of a
disease, duration of SVT, and individual patient perceptions.
premature impulse that impinges on the refractory period of
Supraventricular tachycardia that is persistent for weeks to
the pathway. Slow conduction is usually required for both
months and associated with a fast ventricular response may
initiation and maintenance of a circus movement tachycardia.
lead to a tachycardia-mediated cardiomyopathy (10,11).
In the case of orthodromic AV re-entry (ie, anterograde
Of crucial importance in clinical decision making is a clinical
conduction across the AV node with retrograde conduction
history describing the pattern in terms of the number of episodes,
over an accessory pathway), slowed conduction through the
duration, frequency, mode of onset, and possible triggers.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Figure 1. Initial evaluation of patients
with suspected tachycardia. AVRT indi-
cates atrioventricular reciprocating
tachycardia.
Supraventricular tachycardia has a heterogeneous clinical
origin. For those with narrow complex tachycardias, referral
presentation, most often occurring in the absence of detect-
is indicated for those with drug resistance or intolerance as
able heart disease in younger individuals. The presence of
well as for patients desiring to be free of drug therapy.
associated heart disease should nevertheless always be
Because of the potential for lethal arrhythmias, all patients
sought, and an echocardiogram may be helpful. While a
with the Wolff-Parkinson-White (WPW) syndrome (ie, pre-
physical examination during tachycardia is standard, it usu-
excitation combined with arrhythmias) should be referred for
ally does not lead to a definitive diagnosis. If irregular cannon
further evaluation. All patients with severe symptoms, such
A waves and/or irregular variation in S1 intensity is present,
as syncope or dyspnea, during palpitations should also be
then a ventricular origin of a regular tachycardia is strongly
referred for prompt evaluation by an arrhythmia specialist.
An echocardiographic examination should be considered inpatients with documented sustained SVT to exclude the
2. Diagnostic Investigations
A resting 12-lead echocardiogram (ECG) should be recorded.
possibility of structural heart disease, which usually cannot be
The presence of pre-excitation on the resting ECG in a patient
detected by physical examination or 12-lead ECG.
with a history of paroxysmal regular palpitations is sufficient for
An ambulatory 24-hour Holter recording can be used in
the presumptive diagnosis of AVRT, and attempts to record
patients with frequent (ie, several episodes per week) but
spontaneous episodes are not required before referral to an
transient tachycardias (12). An event or wearable loop recorder
arrhythmia specialist for therapy (Figure 1). Specific therapy is
is often more useful than a 24-hour recording in patients with
discussed in Section V. A clinical history of irregular and
less frequent arrhythmias. Implantable loop recorders may be
paroxysmal palpitations in a patient with baseline pre-excitation
helpful in selected cases with rare symptoms (ie, fewer than two
strongly suggests episodes of AF, which requires immediate
episodes per month) associated with severe symptoms of hemo-
electrophysiological evaluation because these patients are at risk
dynamic instability (13). Exercise testing is less often useful for
for significant morbidity and possibly sudden death (see Section
diagnosis unless the arrhythmia is clearly triggered by exertion.
V-D). The diagnosis is otherwise made by careful analysis of the
Transesophageal atrial recordings and stimulation may be
12-lead ECG during tachycardia (see Section IV). Therefore,
used in selected cases for diagnosis or to provoke paroxysmal
patients with a history of sustained arrhythmia should always be
tachyarrhythmias if the clinical history is insufficient or if
encouraged to have at least one 12-lead ECG taken during the
other measures have failed to document an arrhythmia.
arrhythmia. Automatic analysis systems of 12-lead ECGs are
Esophageal stimulation is not indicated if invasive electro-
unreliable and commonly suggest an incorrect arrhythmia
physiological investigation is planned. Invasive electrophys-
iological investigation with subsequent catheter ablation may
Indications for referral to a cardiac arrhythmia specialist
be used for diagnoses and therapy in cases with a clear history
include presence of a wide complex tachycardia of unknown
of paroxysmal regular palpitations. It may also be used
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Figure 2. Differential diagnosis for narrow QRS tachycardia. Patients with focal junctional tachycardia may mimic the pattern of slow–
fast AVNRT and may show AV dissociation and/or marked irregularity in the junctional rate. AV indicates atrioventricular; AVNRT, atrio-
ventricular nodal reciprocating tachycardia; AVRT, atrioventricular reciprocating tachycardia; MAT, multifocal atrial tachycardia; ms, mil-
liseconds; PJRT, permanent form of junctional reciprocating tachycardia; QRS, ventricular activation on ECG.
empirically in the presence of pre-excitation or disabling
nate the arrhythmia if there is hemodynamic instability. At a
symptoms (Figure 1).
minimum, a monitor strip should be obtained from thedefibrillator, even in cases with cardiogenic shock or cardiac
arrest, before direct current (DC) cardioversion is applied to
The management of patients with symptoms suggestive of an
terminate the arrhythmia.
arrhythmia but without ECG documentation depends on thenature of the symptoms. If the surface ECG is normal and thepatient reports a history consistent with premature extra beats,
a. Differential Diagnosis for NarrowQRS-Complex Tachycardia
then precipitating factors, such as excessive caffeine, alcohol,
If ventricular action (QRS) is narrow (less than 120 ms), then
nicotine intake, recreational drugs, or hyperthyroidism, should
the tachycardia is almost always supraventricular and the
be reviewed and eliminated. Benign extrasystoles are often
differential diagnosis relates to its mechanism (Figure 2). If
manifest at rest and tend to become less common with exercise.
no P waves or evidence of atrial activity is apparent and the
If symptoms and the clinical history indicate that the
arrhythmia is paroxysmal in nature and the resting 12-lead
RR interval is regular, then AVNRT is most commonly the
ECG gives no clue for the arrhythmia mechanism, then
mechanism. P-wave activity in AVNRT may be only partially
further diagnostic tests for documentation may not be neces-
hidden within the QRS complex and may deform the QRS to
sary before referral for an invasive electrophysiological study
give a pseudo–R wave in lead V1 and/or a pseudo–S wave in
and/or catheter ablation. Patients should be taught to perform
inferior leads (Figure 3). If a P wave is present in the ST
vagal maneuvers. A beta-blocking agent may be prescribed
segment and separated from the QRS by 70 ms, then AVRT
empirically provided that significant bradycardia (less than
is most likely. In tachycardias with RP longer than PR, the
50 bpm) have been excluded. Due to the risk of proarrhyth-
most likely diagnosis is atypical AVNRT, permanent form of
mia, antiarrhythmic treatment with class I or class III drugs
junctional reciprocating tachycardia (PJRT) (ie, AVRT via a
should not be initiated without a documented arrhythmia.
slowly conducting accessory pathway), or AT (see Section V-B, D,and E). Responses of narrow QRS-complex tachycardias to
B. General Evaluation of Patients With
adenosine or carotid massage may aid in the differential
diagnosis (Figure 4) (14,15). A 12-lead ECG recording is
1. Diagnostic Evaluation
desirable during use of adenosine or carotid massage. If P
Whenever possible, a 12-lead ECG should be taken during
waves are not visible, then the use of esophageal pill
tachycardia but should not delay immediate therapy to termi-
electrodes can also be helpful.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
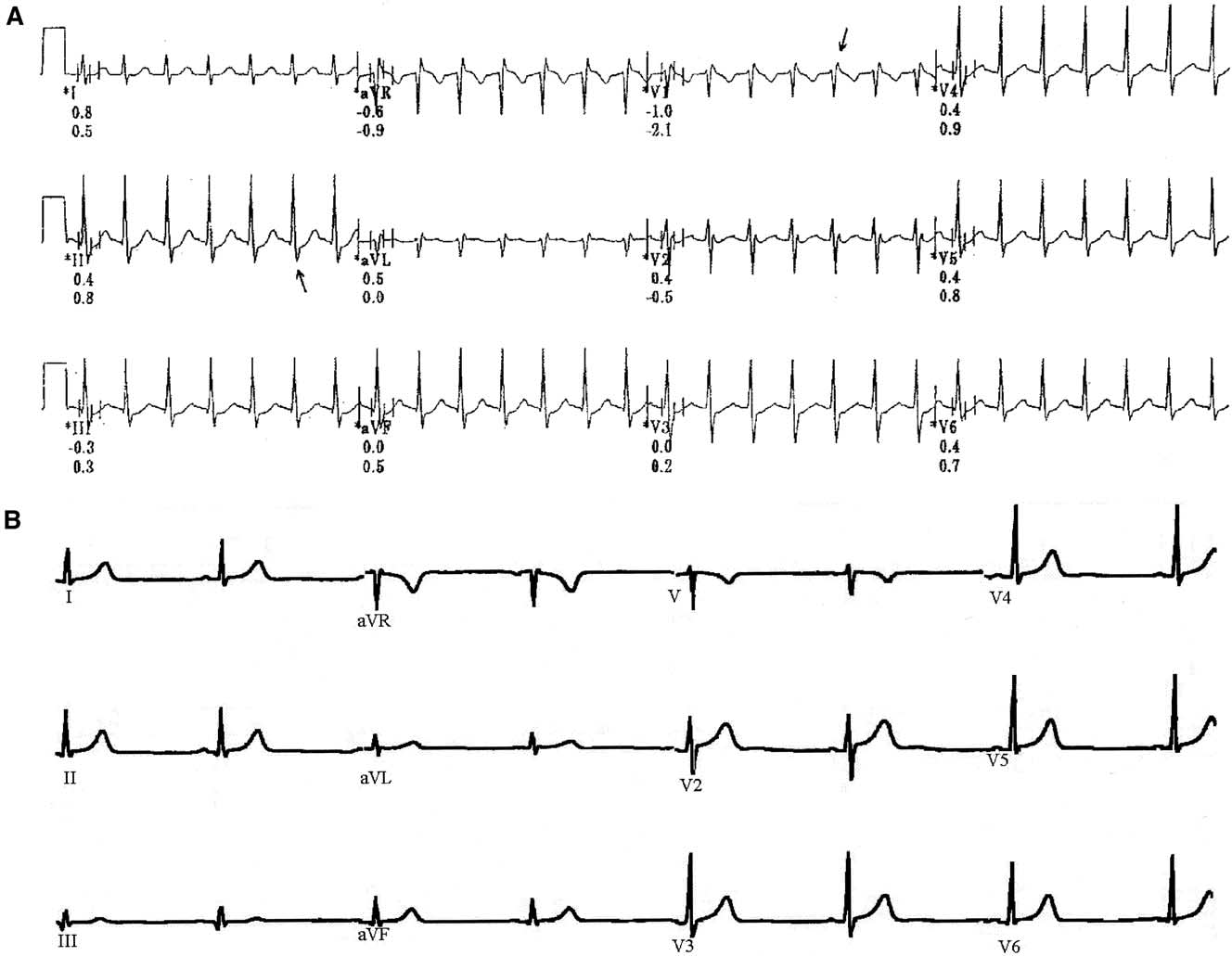
Figure 3. ECG pattern of typical AVNRT. Panel A: 12-Lead ECG shows a regular SVT recorded at an ECG paper speed of 25 mm/sec.
Panel B: After conversion to sinus rhythm, the 12-lead ECG shows sinus rhythm with narrow QRS complexes. In comparison with
Panel A: Note the pseudo r⬘ in V1 (arrow) and accentuated S waves in 2, 3, aVF (arrow). These findings are pathognomonic for AVNRT.
AVNRT indicates atrioventricular nodal reciprocating tachycardia; mm/sec, millimeters per second; QRS, ventricular activation on ECG;
SVT, supraventricular tachycardia; VF, ventricular fibrillation.
b. Differential Diagnosis for Wide
with any supraventricular arrhythmia. If a rate-related
BBB develops during orthodromic AVRT, then the
If the QRS is wide (more than 120 ms), then it is important to
tachycardia rate may slow if the BBB is ipsilateral to the
differentiate between SVT and ventricular tachycardia (VT)
bypass tract location.
(Figure 5). Intravenous medications given for the treatment of
(2) Supraventricular Tachycardia With Atrioventricular
SVT, particularly verapamil or diltiazem, may be deleterious
Conduction Over an Accessory Pathway. Supraventricu-
because they may precipitate hemodynamic collapse for a
lar tachycardia with AV conduction over an accessory
patient with VT. Stable vital signs during tachycardias are not
pathway may occur during AT, atrial flutter, AF,
helpful for distinguishing SVT from VT. If the diagnosis of
AVNRT, or antidromic AVRT. The latter is defined as
SVT cannot be proven or cannot be made easily, then the
anterograde conduction over the accessory pathway and
patient should be treated as if VT were present. Wide QRS
retrograde conduction over the AV node or a second
tachycardia can be divided into three groups: SVT with
accessory AV pathway. A wide-QRS complex with left
bundle-branch block (BBB) or aberration, SVT with AV
bundle-branch block (LBBB) morphology may be seen
conduction over an accessory pathway, and VT.
with anterograde conduction over other types of acces-sory pathways, such as atriofascicular, nodofascicular, or
Block. Bundle-branch block may be pre-existing or may
(3) Ventricular Tachycardia. Several ECG criteria have been
occur only during tachycardia when one of the bundle
described to differentiate the underlying mechanism of a
branches is refractory due to the rapid rate. Most BBBs
are not only rate-related but are also due to a long-short
(i) VENTRICULAR ARRHYTHMIA (VA) DISSOCIATION. VA
sequence of initiation. Bundle-branch block can occur
dissociation with a ventricular rate faster than the
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Figure 4. Responses of narrow complex tachycardias to adenosine. AT indicates atrial tachycardia; AV, atrioventricular; AVNRT, atrio-
ventricular nodal reciprocating tachycardia; AVRT, atrioventricular reciprocating tachycardia; IV, intravenous; QRS, ventricular activation
on ECG; VT, ventricular tachycardia.
atrial rate generally proves the diagnosis of VT
that the QRS patterns in all of the precordial leads are
(Figures 5 and 6) but is clearly discernible in only
similar, and with QS complexes). Positive concordance
30% of all VTs. Fusion complexes represent a
does not exclude antidromic AVRT over a left posterior
merger between conducted sinus (or supraventricu-
accessory pathway.
lar complexes) impulses and ventricular depolariza-
The presence of ventricular fusion beats indicates a ven-
tion occurring during AV dissociation. These com-
tricular origin of the tachycardia.
plexes are pathognomonic of VT. Retrograde VA
QR complexes indicate a myocardial scar and are present in
block may be present spontaneously or brought out
approximately 40% of patients with VTs after myocardial
by carotid massage. The demonstration that P waves
are not necessary for tachycardia maintenancestrongly suggests VT. P waves can be difficult to
The width and morphological criteria are less specific for
recognize during a wide-QRS tachycardia. There-
patients taking certain antiarrhythmic agents and those with
fore, one should also look for evidence of VA
hyperkalemia or severe heart failure. Despite ECG criteria,
dissociation on physical examination: irregular can-
patients presenting with wide QRS-complex tachycardia are
non A waves in the jugular venous pulse and
often misdiagnosed. A positive answer to two inquiries,
variability in the loudness of the first heart sound
namely the presence of a previous myocardial infarct and the
and in systolic blood pressure. If P waves are not
first occurrence of a wide QRS-complex tachycardia after an
visible, then the use of esophageal pill electrodes
infarct, strongly indicates a diagnosis of VT.
can also be useful.
(ii) WIDTH OF THE QRS COMPLEX. A QRS width of more
When a definitive diagnosis can be made on the basis of ECG
than 0.14 seconds with right bundle-branch block
and clinical criteria, acute and chronic treatment should be
(RBBB) or 0.16 seconds during LBBB pattern
initiated on the basis of the underlying mechanism (see
favors VT. The QRS width criteria are not helpful
sections on specific arrhythmias).
for differentiating VT from SVT with AV conduc-
If the specific diagnosis of a wide QRS-complex
tion over an accessory pathway. A patient with SVT
tachycardia cannot be made despite careful evaluation, then
can have a QRS width of more than 0.14 (RBBB) or
the patient should be treated for VT. Acute management of
0.16 (LBBB) in the presence of either pre-existing
patients with hemodynamically stable and regular tachycardia
BBB or AV conduction over an accessory pathway
is outlined in Figure 7.
or when class Ic or class Ia antiarrhythmic drugs are
The most effective and rapid means of terminating any
hemodynamically unstable narrow or wide QRS-complex
(iii) CONFIGURATIONAL CHARACTERISTICS OF THE QRS
tachycardia is DC cardioversion.
COMPLEX DURING TACHYCARDIA. Leads V1 and V6are helpful in differentiating VT from SVT.
a. Acute Management of NarrowQRS-Complex Tachycardia
An RS (from the initial R to the nadir of S) interval longer
In regular narrow QRS-complex tachycardia, vagal maneu-
than 100 ms in any precordial lead is highly suggestive of
vers (ie, Valsalva, carotid massage, and facial immersion in
cold water) should be initiated to terminate the arrhythmia or
A QRS pattern with negative concordance in the precordial
to modify AV conduction. If this fails, then intravenous (IV)
leads is diagnostic for VT ("negative concordance" means
antiarrhythmic drugs should be administered for arrhythmia
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Figure 5. Differential diagnosis for wide QRS-complex tachycardia (more than 120 ms). A QRS conduction delay during sinus rhythm,
when available for comparison, reduces the value of QRS morphology analysis. Adenosine should be used with caution when the diag-
nosis is unclear because it may produce VF in patients with coronary artery disease and AF with a rapid ventricular rate in pre-excited
tachycardias. Various adenosine responses are shown in Figure 4. *Concordant indicates that all precordial leads show either positive
or negative deflections. Fusion complexes are diagnostic of VT. †In pre-excited tachycardias, the QRS is generally wider (ie, more pre-
excited) compared with sinus rhythm. A indicates atrial; AP, accessory pathway; AT, atrial tachycardia; AV, atrioventricular; AVRT, atrio-
ventricular reciprocating tachycardia; BBB, bundle-branch block; LBBB, left bundle-branch block; ms, milliseconds; QRS, ventricular
activation on ECG; RBBB, right bundle-branch block; SR, sinus rhythm; SVT, supraventricular tachycardias; V, ventricular; VF, ventricu-
lar fibrillation; VT, ventricular tachycardia.
termination in hemodynamically stable patients. Adenosine
therapeutic effect is essential. Potential adverse effects of
(or adenosine triphosphate [ATP]) or nondihydropyridine
adenosine include initiation of AF (1% to 15%), which is
calcium-channel antagonists are the drugs of choice (Figure
usually transient and may be particularly problematic for
4). The advantage of adenosine relative to IV calcium-
those with ventricular pre-excitation. Adenosine should be
channel or beta blockers relates to its rapid onset and short
avoided in patients with severe bronchial asthma. It is
half-life. Intravenous adenosine is, therefore, the preferred
important to use extreme care with concomitant use of IV
agent except for patients with severe asthma. Patients treated
calcium-channel blockers and beta blockers because of pos-
with theophylline may require higher doses of adenosine for
sible potentiation of hypotensive and/or bradycardic effects.
effect, and adenosine effects are potentiated by dipyridamole.
An ECG should be recorded during vagal maneuvers or drug
In addition, higher rates of heart block may be seen when
administration because the response may aid in the diagnosis
adenosine is concomitantly administered with carbamaz-
even if the arrhythmia does not terminate (Figure 4). Termi-
epine. Longer-acting agents (eg, IV calcium-channel blockers
nation of the tachycardia with a P wave after the last QRS
or beta blockers [ie, verapamil/diltiazem or metoprolol]) are
complex favors a diagnosis of AVRT or AVNRT.
of value, particularly for patients with frequent atrial prema-
Tachycardia termination with a QRS complex favors AT,
ture beats or ventricular premature beats, which may serve to
which is often adenosine insensitive. Continuation of
trigger early recurrence of PSVT. Adenosine or DC cardio-
tachycardia with AV block is virtually diagnostic of AT or
version is preferred for those with PSVT in whom a rapid
atrial flutter, excludes AVRT, and makes AVNRT very unlikely.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
with WPW syndrome (ie, pre-excitation and arrhythmias)should be referred for further evaluation. Table 1 listsrecommendations for acute management of hemodynamicallystable and regular tachycardia.
V. Specific Arrhythmias
A. Sinus Tachyarrhythmias
Sinus tachycardia usually occurs in response to an appropri-
ate physiological stimulus (eg, exercise) or to an excessive
stimulus (eg, hyperthyroidism). Failure of the mechanisms
that control the sinus rate may lead to an inappropriate sinus
tachycardia. Excessive sinus tachycardia may also occur in
response to upright posture (postural orthostatic tachycardia
syndrome [POTS]). A re-entry mechanism may also occur
within or close to the sinus node, resulting in so-called sinus
node re-entrant tachycardia, which is also sometimes known
as sinoatrial re-entry.
1. Physiological Sinus Tachycardia
The normally innervated sinus node generates an impulse
approximately 60 to 90 times per minute and responds to
autonomic influences. Nevertheless, the sinus node is a
versatile structure and is influenced by many other factors,
Figure 6. Electrocardiogram showing AV dissociation during VT
including hypoxia, acidosis, stretch, temperature, and hor-
in a patient with a wide QRS-complex tachycardia. The P waves
mones (eg, tri-iodothyronine, serotonin).
are marked with arrows.
a. Definition
b. Acute Management of Wide QRS-Complex Tachycardia
Sinus tachycardia is defined as an increase in sinus rate to
Immediate DC cardioversion is the treatment for hemody-
more than 100 bpm in keeping with the level of physical,
namically unstable tachycardias. If the tachycardia is hemo-
emotional, pathological, or pharmacologic stress. Pathologi-
dynamically stable and definitely supraventricular, then man-
cal causes of sinus tachycardia include pyrexia, hypovolemia,
agement is as described for narrow QRS tachycardias (Figure
or anemia, which may result from infections. Drugs that
4). For pharmacologic termination of a stable wide QRS-
induce sinus tachycardia include stimulants (eg, caffeine,
complex tachycardia, IV procainamide and/or sotalol are
alcohol, nicotine); prescribed compounds (eg, salbutamol,
recommended on the basis of randomized but small studies.
aminophylline, atropine, catecholamines); and certain recre-
Amiodarone is also considered acceptable. Amiodarone is
ational/illicit drugs (eg, amphetamines, cocaine, "ecstasy,"
preferred compared with procainamide and sotalol for pa-
cannabis) (33). Anticancer treatments, in particular anthracy-
tients with impaired left ventricular (LV) function or signs of
cline compounds such as doxorubicin (or Adriamycin) and
heart failure. These recommendations are in accord with the
daunorubicin, can also trigger sinus tachycardia as part of the
current Advanced Cardiovascular Life Support guidelines
acute cardiotoxic response that is predominantly catechol-
(16). Special circumstances may require alternative therapy
amine/histamine induced (34) or part of a late cardiotoxic
(ie, pre-excited tachycardias and VT caused by digitalis
response. Sinus tachycardia may signal severe underlying
toxicity). For termination of an irregular wide QRS-complex
pathologies and often requires comprehensive evaluation.
tachycardia (ie, pre-excited AF), DC cardioversion is recom-
Atrial and sinus tachycardias may be difficult to differentiate.
mended. Or, if the patient is hemodynamically stable, thenpharmacologic conversion using IV ibutilide or flecainide is
b. Mechanism
Sinus tachycardia results from physiological influences onindividual pacemaker cells and from an anatomical shift in
c. Further Management
the site of origin of atrial depolarization superiorly within the
After successful termination of a wide QRS-complex
tachycardia of unknown etiology, patients should be referredto an arrhythmia specialist. Patients with stable narrow
c. Diagnosis
QRS-complex tachycardia, normal LV function, and a normal
In normal sinus rhythm, the P wave on a 12-lead ECG is
ECG during sinus rhythm (ie, no pre-excitation) may require
positive in leads I, II, and aVF and negative in aVR. Its axis
no specific therapy. Referral is indicated for those with drug
in the frontal plane lies between 0 and ⫹90; in the horizontal
resistance or intolerance as well as for patients desiring to be
plane, it is directed anteriorly and slightly leftward and can,
free of lifelong drug therapy. When treatment is indicated,
therefore, be negative in leads V1 and V2 but positive in leads
options include catheter ablation or drug therapy. Finally,
V3 to V6. The P waves have a normal contour, but a larger
because of the potential for lethal arrhythmias, all patients
amplitude may develop and the wave may become peaked
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Figure 7. Acute management of patients with hemodynamically stable and regular tachycardia. *A 12-lead ECG during sinus rhythm
must be available for diagnosis. †Adenosine should be used with caution in patients with severe coronary artery disease and may pro-
duce AF, which may result in rapid ventricular rates for patients with pre-excitation. **Ibutilide is especially effective for patients with
atrial flutter but should not be used in patients with EF less than 30% due to increased risk of polymorphic VT. AF indicates atrial fibril-
lation; AV, atrioventricular; BBB, bundle-branch block; DC, direct current; IV, intravenous; LV, left ventricle; QRS, ventricular activation
on ECG; SVT, supraventricular tachycardia; VT, ventricular tachycardia.
(35). Sinus tachycardia is nonparoxysmal, thus differentiating
for symptomatic thyrotoxicosis in combination with carbima-
it from re-entry.
zole or propylthiouracyl while these palliative agents takeeffect (42). Nondihydropyridine calcium-channel blockers,
d. Treatment
such as dilitiazem or verapamil, may be of benefit in patients
The mainstay in the management of sinus tachycardias
with symptomatic thyrotoxicosis if beta blockade is
primarily involves identifying the cause and either eliminat-ing or treating it. Beta blockade, however, can be extremely
useful and effective for physiological symptomatic sinustachycardia triggered by emotional stress and other anxiety-
2. Inappropriate Sinus Tachycardia
related disorders (36 –38); for prognostic benefit after myo-cardial infarction (39); for the symptomatic and prognostic
a. Definition
benefits in certain other irreversible causes of sinus
Inappropriate sinus tachycardia is a persistent increase in
tachycardias, such as congestive cardiac failure (40,41); and
resting heart rate or sinus rate unrelated to, or out of
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Recommendations for Acute Management of Hemodynamically Stable and Regular Tachycardia
Level of Evidence
Narrow QRS-complex tachycardia (SVT)
Verapamil, diltiazem
Wide QRS-complex tachycardia
Pre-excited SVT/AF†
Wide QRS-complex tachycardia of unknown
Wide QRS-complex tachycardia of unknown
origin in patients with poor LV function
DC cardioversion, lidocaine
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily
reflect a preferred sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer tothe ACC/AHA/ESC Guidelines on the Management of Patients With Atrial Fibrillation.
*All listed drugs are administered intravenously.
†See Section V-D.
‡Should not be taken by patients with reduced LV function.
§Adenosine should be used with caution in patients with severe coronary artery disease because vasodilation of normal coronary
vessels may produce ischemia in vulnerable territory. It should be used only with full resuscitative equipment available.
¶Beta blockers may be used as first-line therapy for those with catecholamine-sensitive tachycardias, such as right ventricular
**Verapamil may be used as first-line therapy for those with LV fascicular VT.
AF indicates atrial fibrillation; BBB, bundle-branch block; DC, direct current; ECG, electrocardiogram; LV, left ventricular; QRS,
ventricular activation on ECG; SVT, supraventricular tachycardia; VT, ventricular tachycardia.
proportion with, the level of physical, emotional, pathologi-
presentation is that of palpitations, symptoms such as chest
cal, or pharmacologic stress.
pain, shortness of breath, dizziness, lightheadedness, andpre-syncope have also been reported. The degree of disability
b. Mechanism
can vary tremendously, from totally asymptomatic patients
The underlying pathological basis for inappropriate sinus
identified during routine medical examination to individuals
tachycardia is likely to be multifactorial, but two main
who are fully incapacitated. Clinical examination and routine
mechanisms have been proposed:
investigations allow elimination of a secondary cause for thetachycardia but are generally not helpful in establishing the
1. Enhanced automaticity of the sinus node
2. Abnormal autonomic regulation of the sinus node with
excess sympathetic and reduced parasympathetic tone.
d. DiagnosisSinus tachycardia is diagnosed on the basis of invasive and
c. Presentation
noninvasive criteria (43):
A high proportion of patients with inappropriate sinustachycardia are healthcare professionals, and approximately
1. The presence of a persistent sinus tachycardia (heart
90% are female. The mean age of presentation is 38 plus or
rate more than 100 bpm) during the day with excessive
minus 12 years. Although the predominant symptom at
rate increase in response to activity and nocturnal
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Recommendations for Treatment of Inappropriate Sinus Tachycardia
Level of Evidence
Verapamil, diltiazem
Interventional Catheter ablation—sinus node
The order in which treatment recommendations appear in this table within each class of
recommendation does not necessarily reflect a preferred sequence of administration. Please refer totext for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines onthe Management of Patients With Atrial Fibrillation.
*Used as a last resort.
normalization of rate as confirmed by a 24-hour Holter
usually triggered and terminated abruptly by an atrial prema-
2. The tachycardia (and symptoms) is nonparoxysmal3. P-wave morphology and endocardial activation identical
b. Mechanism
Heterogeneity of conduction within the sinus node provides a
4. Exclusion of a secondary systemic cause (eg, hyperthy-
substrate for re-entry, but it is still not known whether the
roidism, pheochromocytoma, physical deconditioning)
re-entry circuit is isolated within the sinus node itself,whether perisinus atrial tissue is necessary, or whether re-
e. Treatment
entry around a portion of the crista terminalis is responsible.
The treatment of inappropriate sinus tachycardia is predom-
The fact that this arrhythmia, like AVNRT, responds to vagal
inantly symptom driven. The risk of tachycardia-induced
maneuvers and adenosine, however, suggests that sinus node
cardiomyopathy in untreated patients is unknown but is likely
tissue is involved in the re-entrant circuit.
to be small.
Although no randomized, double-blinded, placebo-
c. Presentation
controlled clinical trials exist, beta blockers may be useful
The incidence of sinus node re-entry tachycardia in patients
and should be prescribed as first-line therapy in the majority
undergoing electrophysiological study for SVT ranges be-
of these patients. Anecdotal evidence suggests that nondihy-
tween 1.8% and 16.9% and up to 27% for those with focal
dropyridine calcium-channel blockers, such as verapamil and
AT. Contrary to popular belief, there is a high incidence of
diltiazem, are also effective.
underlying organic heart disease in patients with sinus node
Sinus node modification by catheter ablation remains a
re-entry tachycardia. Patients present with symptoms of
potentially important therapeutic option in the most refractory
palpitations, lightheadedness, and presyncope. Syncope is
cases of inappropriate sinus tachycardia. Potential adverse
extremely rare, as the rates of the tachycardia are rarely
effects include pericarditis, phrenic nerve injury, superior
higher than 180 bpm. An important clue for diagnosis is the
vena cava (SVC) syndrome, or need for permanent pacing. A
paroxysmal nature of the attacks.
number of case reports have recorded successful surgical
d. Diagnosis
excision or radiofrequency (RF) ablation of the sinus node
Sinus node re-entry tachycardia is diagnosed on the basis of
(44,45). The diagnosis of POTS (see Section V-A-3) must be
invasive and noninvasive criteria (43). Clinically, the follow-
excluded before considering ablation. In a retrospective
ing features are highly suggestive of this arrhythmia:
analysis of 29 cases undergoing sinus node modification forinappropriate sinus tachycardia (46), a 76% acute success rate
1. The tachycardia and its associated symptoms are
(22 out of 29 cases) was reported. The long-term success rate
has been reported to be around 66%. Table 2 lists recommen-
2. P-wave morphology is identical to sinus rhythm with the
dations for treatment of inappropriate sinus tachycardia.
vector directed from superior to inferior and from right toleft.
3. Postural Orthostatic Tachycardia Syndrome
3. Endocardial atrial activation is in a high-to-low and
This section of the full-text guideline has not been included in
right-to-left pattern, with an activation sequence similar to
the executive summary because it is not a disorder of the
that of sinus rhythm.
sinus node. Please refer to Section V-A-3 of the full-text
4. Induction and/or termination of the arrhythmia occurs with
guideline for differential diagnosis and treatment recommen-
premature atrial stimuli.
dations on this topic.
5. Termination occurs with vagal maneuvers or adenosine.
6. Induction of the arrhythmia is independent of atrial or
4. Sinus Node Re-Entry Tachycardia
AV-nodal conduction time.
a. Definition
e. Treatment
Sinus node re-entry tachycardias arise from re-entrant circuits
There have been no controlled trials of drug prophylaxis
involving the sinus node's production of paroxysmal, often
involving patients with sinus node re-entrant tachycardia.
nonsustained bursts of tachycardia with P waves that are
Clinically suspected cases of symptomatic sinus node re-
similar, if not identical, to those in sinus rhythm. They are
entrant tachycardia may respond to vagal maneuvers, adeno-
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
sine, amiodarone, beta blockers, nondihydropyridine
3. Long-Term Pharmacologic Therapy
calcium-channel blockers, or even digoxin. Patients whose
For patients with frequent, recurrent sustained episodes of
tachyarrhythmias are well tolerated and easily controlled by
AVNRT who prefer long-term oral therapy instead of cathe-
vagal maneuvers and/or drug therapy should not be consid-
ter ablation, a spectrum of antiarrhythmic agents is available.
ered for electrophysiological studies. Electrophysiological
Standard therapy includes nondihydropyridine calcium-
studies are indicated for patients with frequent or poorly
channel blockers, beta blockers, and digoxin. In patients
tolerated episodes of tachycardia that do not adequately
without structural heart disease who do not respond to
respond to drug therapy and for patients in whom the exact
AV-nodal– blocking agents, the class Ic drugs flecainide and
nature of the tachycardia is uncertain and for whom electro-
propafenone have become the preferred choice. In most
physiological studies would aid appropriate therapy. Radio-
cases, class III drugs, such as sotalol or amiodarone, are
frequency catheter ablation of persistent sinus node re-entry
unnecessary (53). Class Ia drugs, such as quinidine, procain-
tachycardias identified through electrophysiological study is
amide, and disopyramide, have limited appeal due to their
generally successful (52).
multidosing regimens, modest efficacy, and adverse andproarrhythmic effects.
B. Atrioventricular Nodal Reciprocating
A major limitation in evaluating antiarrhythmic agents for
treating AVNRT is the general absence of large multicenter,
1. Definitions and Clinical Features
randomized, placebo-controlled studies.
Atrioventricular nodal reciprocating tachycardia is the most
a. Prophylactic Pharmacologic Therapy
common form of PSVT. It is more prevalent in females; isassociated with palpitations, dizziness, and neck pulsations;
(1) Calcium-Channel Blockers, Beta Blockers, and Digoxin.
and is not usually associated with structural heart disease.
Comments regarding the long-term efficacy of calcium-
Rates of tachycardia are often between 140 and 250 per
channel blockers, beta blockers, and digoxin taken orally
for management of AVNRT are limited by the small
Although the re-entrant circuit was initially thought to be
number of randomized patients studied. A small random-
confined to the compact AV node, a more contemporary view
ized (11 patients), double-blinded, placebo-controlled
recognizes the usual participation of perinodal atrial tissue as
trial showed that verapamil taken orally decreases thenumber and duration of both patient-reported and elec-
the most common component of the re-entrant circuit. It has
trophysiologically-recorded episodes. A similar finding
been shown convincingly, however, that AVNRT may persist
was demonstrated with doses of 360 to 480 mg/d with a
without participation of atrial tissue. Atrioventricular nodal
trend toward greater effect with higher doses; however,
reciprocating tachycardia involves reciprocation between two
the study was underpowered to detect a modest
functionally and anatomically distinct pathways. In most
cases, the fast pathway appears to be located near the apex of
Oral digoxin (0.375 mg/d), verapamil (480 mg/d), and
Koch's triangle. The slow pathway extends inferoposterior to
propranolol (240 mg/d) showed similar efficacy in 11
the compact AV-node tissue and stretches along the septal
patients in a randomized, double-blinded, crossover
margin of the tricuspid annulus at the level of, or slightly
study. There was no difference among the drugs with
superior to, the coronary sinus.
respect to frequency or duration of PSVT.
(2) Class I Drugs. The data showing efficacy of procain-
During typical AVNRT, the fast pathway serves as the
amide, quinidine, and disopyramide are from the older
retrograde limb of the circuit, whereas the slow pathway is
literature and are derived from small studies. These drugs
the anterograde limb (ie, slow–fast AV-node re-entry). After
are rarely used for treating AVNRT today.
conduction through the slow pathway to the His bundle and
Long-term benefits of oral flecainide in AVNRT were
ventricle, brisk conduction back to the atrium over the fast
initially shown in an open-labeled study. At doses be-
pathway results in inscription of the shorter duration (40 ms)
tween 200 and 300 mg/d, flecainide completely sup-
P wave during or close to the QRS complex (less than or
pressed episodes in 65% of patients. Several double-
equal to 70 ms) often with a pseudo-r⬘ in V1 (see Figure 3).
blinded, placebo-controlled trials have confirmed the
Less commonly (approximately 5% to 10%), the tachycardia
efficacy of flecainide for prevention of recurrences.
circuit is reversed such that conduction proceeds anterograde-
Events are reduced when compared with placebo, with an
ly over the fast pathway and retrogradely over the slow
increase in the median time to the first recurrence and agreater interval between attacks. Open-labeled, long-term
pathway (ie, fast–slow AV-node re-entry, or atypical
studies suggest excellent chronic tolerance and safety. In
AVNRT) producing a long R-P tachycardia (ie, atypical
patients without structural heart disease, 7.6% discontin-
AVNRT) but other circuits may also be involved. The P
ued the drug due to a suboptimal clinical response, and
wave, negative in leads III and aVF, is inscribed prior to the
5% discontinued it because of noncardiac (usually central
QRS. Infrequently, both limbs of the tachycardia circuit are
nervous system) side effects. Class Ic agents (ie, flecain-
composed of slowly conducting tissue (ie, slow–slow AV-
ide and propafenone) are contraindicated for patients
node re-entry), and the P wave is inscribed after the QRS (ie,
with structural heart disease. Moreover, class Ic drugs are
RP interval more than or equal to 70 ms).
often combined with beta-blocking agents to enhanceefficacy and reduce the risk of one-to-one conduction
2. Acute Treatment
over the AV node if atrial flutter occurs.
Acute evaluation and treatment of the patient with PSVT are
Flecainide appears to have greater long-term efficacy
discussed in Sections IV-A and IV-B.
than verapamil. Although both drugs (median doses 200
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
mg/d and 240 mg/d, respectively) have an equivalent
with PSVT in terms of conversion to sinus rhythm (54).
reduction in the frequency of episodes, 30% of patients
Favorable results comparing diltiazem plus propranolol with
had complete suppression of all symptomatic episodes
placebo have also been reported by others. Hypotension and
with flecainide, whereas 13% had complete suppression
sinus bradycardia are rare complications. Single-dose therapy
with verapamil. Discontinuation rates due to adverse
with diltiazem plus propranolol is associated with a signifi-
effects were equivalent, 19% and 24%, respectively.
cant reduction in emergency room visits in appropriately
Propafenone is also an effective drug for prophylaxis
of AVNRT. In a double-blinded, placebo-controlled trial,
selected patients (54).
in which time to treatment failure was analyzed, the RR
4. Catheter Ablation
of treatment failure for placebo versus propafenone was
Targeting the slow pathway along the posteroseptal region of
6.8. A single-center, randomized, double-blinded,
the tricuspid annulus markedly reduces the risk of heart block
placebo-controlled study showed that propafenone (300mg taken three times per day) reduced the recurrence rate
and is the preferable approach. A prospective, randomized
to one-fifth of that of placebo.
comparison of the fast- and slow-pathway approaches dem-
(3) Class III Drugs. Limited prospective data are available
onstrates equivalent success rates. Advantages of slow-
for use of class III drugs (eg, amiodarone, sotalol,
pathway ablation include a lower incidence of complete AV
dofetilide). Although many have been used effectively to
block (1% versus 8%) and the absence of the hemodynamic
prevent recurrences, routine use should be avoided due to
consequences of marked prolongation of the PR interval.
their toxicities, including proarrhythmia (ie, torsades de
Hence, slow pathway ablation is always used initially and fast
pointes). A placebo-controlled trial found sotalol to be
pathway ablation is considered only when slow pathway
superior to placebo in prolonging time to recurrence of
ablation fails.
PSVT. With regard to dofetilide, a multicenter, random-
The NASPE Prospective Catheter Ablation Registry in-
ized, placebo-controlled study showed that patients withPSVT had a 50% probability of complete symptomatic
cluded 1197 patients who underwent AV-nodal modification
suppression with dofetilide over a 6-month follow-up
for AVNRT. Success was achieved in 96.1%, and the only
(500 g taken twice per day), whereas the probability of
significant complication was a 1% incidence of second-
suppression in the control group was 6% (p less than
degree or third-degree AV block (55). These data have been
0.001). There were no proarrhythmic events (53). In this
confirmed by others (56). Atrioventricular block may com-
study, dofetilide was shown to be as effective as
plicate slow-pathway ablation caused by posterior displace-
propafenone (150 mg taken three times per day).
ment of the fast pathway, superior displacement of the slow
Little data exists regarding the effects of amiodarone
pathway (and coronary sinus), or inadvertent anterior dis-
on AVNRT. In one open-labeled study in the electro-
placement of the catheter during RF application. Pre-existing
physiology laboratory, IV amiodarone (5 mg · kg⫺1 · 5
first-degree AV block does not appear to increase appreciably
minutes⫺1) terminated tachycardia in seven out of ninepatients. Treatment with oral amiodarone (maintenance
the risk of developing complete AV block, although caution
dose 200 to 400 mg/d) for 66 plus or minus 24 days
is advised. The recurrence rate after ablation is approximately
prevented recurrence and inducibility in all patients, with
3% to 7% (56,57).
its predominant effect being the depression of conduction
Ablation of the slow pathway may be performed in patients
in the retrograde fast pathway. Of note, amiodarone has
with documented SVT (which is morphologically consistent
been shown to be safe in structural heart disease, partic-
with AVNRT) but in whom only dual AV-nodal physiology
ularly LV dysfunction.
(but not tachycardia) is demonstrated during electrophysio-
b. Single-Dose Oral Therapy (Pill-in-the-Pocket)
logical study. Because arrhythmia induction is not an avail-
Single-dose therapy refers to administration of a drug only
able endpoint for successful ablation in this circumstance, the
during an episode of tachycardia for the purpose of termina-
surrogate endpoint of an accelerated junctional rhythm during
tion of the arrhythmia when vagal maneuvers alone are not
ablation is a good indication of slow-pathway ablation.
effective. This approach is appropriate to consider for patients
Slow-pathway ablation may be considered at the discretion
with infrequent episodes of AVNRT that are prolonged (ie,
of the physician when sustained (more than 30 seconds)
lasting hours) but yet well tolerated (54), and obviates
AVNRT is induced incidentally during an ablation procedure
exposure of patients to chronic and unnecessary therapy
directed at a different clinical tachycardia.
between their rare arrhythmic events. This approach necessi-
Indications for ablation depend on clinical judgment and
tates the use of a drug that has a short time to take effect (ie,
patient preference. Factors that contribute to the therapeutic
immediate-release preparations). Candidate patients should
decision include the frequency and duration of tachycardia,
be free of significant LV dysfunction, sinus bradycardia, or
tolerance of symptoms, effectiveness and tolerance of antiar-
rhythmic drugs, the need for lifelong drug therapy, and the
A single oral dose of flecainide (approximately 3 mg/kg)
presence of concomitant structural heart disease. Catheter
has been reported to terminate acute episodes of AVNRT in
ablation has become the preferred therapy, over long-term
adolescents and young adults without structural heart disease,
pharmacologic therapy, for management of patients with
although it offered no benefit compared with placebo in other
AVNRT. The decision to ablate or proceed with drug therapy
studies (54).
as initial therapy is, however, often patient specific, related to
Single-dose oral therapy with diltiazem (120 mg) plus
lifestyle issues (eg, planned pregnancy, competitive athlete,
propranolol (80 mg) has been shown to be superior to both
recreational pilot), affected by individual inclinations or
placebo and flecainide in sequential testing in 33 patients
aversions with regard to an invasive procedure or the chro-
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Recommendations for Long-Term Treatment of Patients With Recurrent AVNRT
Clinical Presentation
Level of Evidence
Poorly tolerated AVNRT with hemodynamic
Catheter ablation
Verapamil, diltiazem, beta blockers, sotalol,
Recurrent symptomatic AVNRT
Catheter ablation
Diltiazem, beta blockers
Recurrent AVNRT unresponsive to beta
Flecainide,* propafenone,* sotalol
blockade or calcium-channel blocker and
patient not desiring RF ablation
AVNRT with infrequent or single episode in
Catheter ablation
patients who desire complete control of
arrhythmia
Documented PSVT with only dual AV-nodal
Verapamil, diltiazem, beta blockers, flecainide,*
pathways or single echo beats demonstrated
during electrophysiological study and no
other identified cause of arrhythmia
Catheter ablation‡
Infrequent, well-tolerated AVNRT
Verapamil, diltiazem, beta blockers
Catheter ablation
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily reflect a preferred
sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines on theManagement of Patients With Atrial Fibrillation.
*Relatively contraindicated for patients with coronary artery disease, LV dysfunction, or other significant heart disease.
†Digoxin is often ineffective because its pharmacologic effects can be overridden by enhanced sympathetic tone.
‡Decision depends on symptoms.
AV indicates atrioventricular; AVNRT, atrioventricular nodal reciprocating tachycardia; LV, left ventricular; PSVT, paroxysmal supraventricular
tachycardia; RF, radiofrequency.
nicity of drug therapy, and influenced by the availability of an
node are, in fact, ectopic. The term "automatic junctional
experienced center for ablation. Because drug efficacy is in
tachycardia" suggests that the dominant mechanism is abnor-
the range of 30% to 50%, catheter ablation may be offered as
mal automaticity; however, mechanisms other than abnormal
first-line therapy for patients with frequent episodes of
automaticity may be operative. The writing committee be-
tachycardia. Patients considering RF ablation must be willing
lieves it is reasonable to designate these arrhythmias as focal
to accept the risk, albeit low, of AV block and pacemaker
junctional tachycardia, which has a neutral connotation with
implantation. Table 3 lists recommendations for long-term
regard to arrhythmic mechanism.
treatment of patients with recurrent AVNRT.
b. DiagnosesThe unifying feature of focal junctional tachycardias is their
C. Focal and Nonparoxysmal
origin from the AV node or His bundle. This site of arrhythmia
origin results in varied ECG manifestations because the arrhyth-
1. Focal Junctional Tachycardia
mia requires participation of neither the atrium nor the ventriclefor its propagation. The ECG features of focal junctional
a. Definition
tachycardia include heart rates of 110 to 250 bpm and a narrow
Abnormally rapid discharges from the junctional region have
complex or typical BBB conduction pattern. Atrioventricular
been designated by a number of terms, each of which has
dissociation is often present (Figure 8), although one-to-one
deficiencies. For example, some refer to these disorders as
retrograde conduction may be transiently observed. On occasion,
"junctional ectopic tachycardia." The problem with this term
the junctional rhythm is quite erratic, suggesting AF. Finally,
is redundancy because all pacemakers outside of the sinus
isolated, concealed junctional extrasystoles that fail to conduct to
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
to the AV node but the procedure appears to be associatedwith risk (5% to 10%) of AV block.
In one series, 17 patients with focal junctional tachycardia
were referred for electrophysiological testing and possiblecatheter ablation. Ten of 11 patients undergoing RF catheterablation in this series had acute tachycardia elimination. Eightpatients remained symptom free during follow-up (68).
2. Nonparoxysmal Junctional Tachycardia
a. Definition and Clinical FeaturesNonparoxysmal junctional tachycardia is a benign arrhythmiathat is characterized by a narrow complex tachycardia with
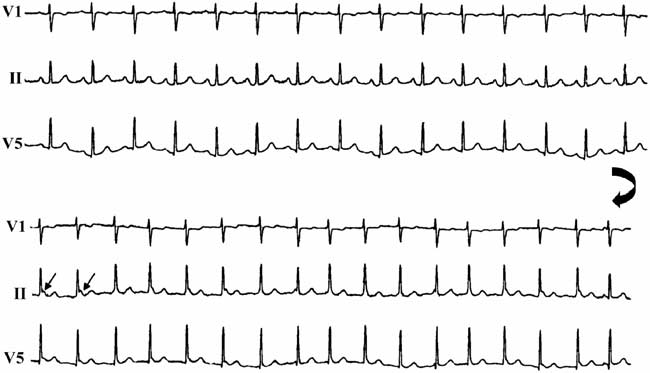
Figure 8. Surface ECG recording from leads V1, II, and V5 in a
rates of 70 to 120 bpm. The arrhythmia mechanism is thought
patient with focal junctional tachycardia. The upper panel shows
to be enhanced automaticity arising from a high junctional
sinus rhythm. The lower panel shows tachycardia onset with the
focus (14) or in response to a triggered mechanism. It shows
characteristic finding of isorhythmic AV dissociation (arrows).
The large arrow signifies continuous recording. AV indicates
a typical "warm-up" and "cool-down" pattern and cannot be
terminated by pacing maneuvers. The most important featureabout this tachycardia is that it may be a marker for a serious
the ventricles may produce episodic AV block by rendering the
underlying condition, such as digitalis toxicity, postcardiac
AV node intermittently refractory.
surgery, hypokalemia, or myocardial ischemia. Other associ-
During electrophysiological study, each ventricular depo-
ated conditions include chronic obstructive lung disease with
larization is preceded by a His bundle deflection (68). The
hypoxia, and inflammatory myocarditis. Unlike the more
precise electrophysiological mechanism of this arrhythmia is
rapid form of focal junctional tachycardia, there is commonly
thought to be either abnormal automaticity or triggered
one-to-one AV association. In some cases, particularly in the
activity based on its response to beta-adrenergic stimulation
setting of digitalis toxicity, anterograde AV-nodal Wenck-
and calcium-channel blockade.
ebach conduction block may be observed.
The diagnosis must be differentiated from other types of
c. Clinical FeaturesFocal junctional tachycardia, also known as automatic or
narrow complex tachycardia, including AT, AVNRT, and
paroxysmal junctional tachycardia, is a very uncommon
AVRT. Usually, the clinical setting in which the arrhythmia
arrhythmia. It is rare in the pediatric population and even less
presents and the ECG findings allow the clinician to ascertain
common in adults. Under the common umbrella of "focal
the arrhythmia mechanism. In some cases, however, the
junctional tachycardia" are several distinct clinical syn-
mechanism may be determined only with invasive electro-
dromes. The most prevalent among these, so-called "congen-
ital junctional ectopic tachycardia" and "postoperative junc-
b. Management
tional ectopic tachycardia," occur exclusively in pediatric
The mainstay of managing nonparoxysmal junctional
patients and are, therefore, outside of the scope of this
tachycardia is to correct the underlying abnormality. With-
holding digitalis when junctional tachycardia is the only
Focal junctional tachycardia usually presents in young
clinical manifestation of toxicity is usually adequate.If, how-
adulthood. It has been speculated that this form of arrhythmia
ever, ventricular arrhythmias or high-grade heart block are
is an adult extension of the pediatric disorder commonly
observed, then treatment with digitalis-binding agents may be
termed "congenital junctional ectopic tachycardia." If this is
indicated. It is not unusual for automatic activity from the AV
the case, then it appears to be more benign than is the
node to exceed the sinus rate, leading to loss of AV
pediatric form. This arrhythmia is usually exercise or stress
synchrony. This should be regarded as a physiological con-
related and may be found in patients with structurally normal
dition, and no specific therapy is indicated. Persisting junc-
hearts or in patients with congenital abnormalities, such as
tional tachycardia may be suppressed by beta blockers or
atrial or ventricular septal defects. The patients are often quite
calcium-channel blockers (14). In rare cases, the emergence
symptomatic and, if untreated, may develop heart failure,
of a junctional rhythm is the result of sinus node dysfunction.
particularly if their tachycardia is incessant.
Sympathetic stimulation of the AV-junction automaticity can
d. Management
lead to an AV-junctional rhythm that supersedes the sinus
Relatively little information is available about the response of
rhythm. In these cases, symptoms mimicking "pacemaker
rapid focal junctional tachycardia to suppressive drug ther-
syndrome" may occur due to retrograde conduction from the
apy. Patients typically show some responsiveness to beta
AV junction to the atrium and resultant atrial contraction
blockade. The tachycardia can be slowed or terminated with
against closed atrioventricular valves, resulting in cannon A
IV flecainide and shows some positive response to long-term
waves and possible hypotension. Atrial pacing is an effective
oral therapy. Drug therapy is only variably successful, and
treatment for this condition. Table 4 lists recommendations
ablative techniques have been introduced to cure tachycardia.
for treatment of focal and nonparoxysmal junctional
Catheter ablation can be curative by destroying foci adjacent
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Recommendations for Treatment of Focal and Nonparoxysmal Junctional Tachycardia Syndromes
Level of Evidence References
Focal junctional tachycardia
Catheter ablation
Nonparoxysmal junctional tachycardia
Reverse digitalis toxicity
Correct hypokalemia
Treat myocardial ischemia
Beta blockers, calcium-channel blockers
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily reflect a preferred
sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines on theManagement of Patients With Atrial Fibrillation.
*Data available for pediatric patients only.
D. Atrioventricular Reciprocating Tachycardia
The diagnosis of WPW syndrome is reserved for patients
(Extra Nodal Accessory Pathways)
who have both pre-excitation and tachyarrhythmias. Among
Typical accessory pathways are extra nodal pathways that
patients with WPW syndrome, AVRT is the most common
connect the myocardium of the atrium and the ventricle
arrhythmia, accounting for 95% of re-entrant tachycardias
across the AV groove. Delta waves detectable on an ECG
that occur in patients with an accessory pathway.
have been reported to be present in 0.15% to 0.25% of the
Atrioventricular re-entry tachycardia is further subclassi-
general population. Pathway conduction may be intermittent.
fied into orthodromic and antidromic AVRT. During ortho-
A higher prevalence of 0.55% has been reported in first-
dromic AVRT, the re-entrant impulse conducts over the AV
degree relatives of patients with accessory pathways. Acces-
node and the specialized conduction system from the atrium
sory pathways can be classified on the basis of their location
to the ventricle and utilizes the accessory pathway for
along the mitral or tricuspid annulus; type of conduction
conduction from the ventricle to the atrium. During anti-
(decremental [ie, progressive delay in accessory pathway
dromic AVRT, the re-entrant impulse travels in the reverse
conduction in response to increased paced rates] or nondec-
direction, with anterograde conduction from the atrium to the
remental); and whether they are capable of anterograde
ventricle occurring via the accessory pathway and retrograde
conduction, retrograde conduction, or both. Accessory path-
conduction over the AV node or a second accessory pathway.
ways usually exhibit rapid, nondecremental conduction, sim-
Antidromic AVRT occurs in only 5% to 10% of patients with
ilar to that present in normal His-Purkinje tissue and atrial or
WPW syndrome. Pre-excited tachycardias can also occur in
ventricular myocardium. Approximately 8% of accessory
patients with AT, atrial flutter, AF, or AVNRT, with the
pathways display decremental anterograde or retrograde con-
accessory pathway acting as a bystander (ie, not a critical part
duction. The term "permanent form of junctional reciprocat-
of the tachycardia circuit).
ing tachycardia" is used to refer to a rare clinical syndrome
Atrial fibrillation is a potentially life-threatening arrhyth-
involving a slowly conducting, concealed, usually postero-
mia in patients with WPW syndrome. If an accessory path-
septal (inferoseptal) accessory pathway. This syndrome is
way has a short anterograde refractory period, then rapid
characterized by an incessant SVT, usually with negative P
repetitive conduction to the ventricles during AF can result in
waves in leads II, III, and aVF and a long RP interval (RP
a rapid ventricular response with subsequent degeneration to
more than PR).
VF. It has been estimated that one-third of patients with
Accessory pathways that are capable of only retrograde
WPW syndrome also have AF. Accessory pathways appear to
conduction are referred to as "concealed," whereas those
play a pathophysiological role in the development of AF in
capable of anterograde conduction are "manifest," demon-
these patients, as most are young and do not have structuralheart disease. Rapid AVRT may play a role in initiating AF
strating pre-excitation on a standard ECG. The degree of
in these patients. Surgical or catheter ablation of accessory
pre-excitation is determined by the relative conduction to the
pathways usually eliminates AF as well as AVRT (81).
ventricle over the AV node His bundle axis versus theaccessory pathway. In some patients, anterograde conduction
1. Sudden Death in WPW Syndrome and Risk
is apparent only with pacing close to the atrial insertion site,
as, for example, for left-lateral–located pathways. Manifest
The incidence of sudden cardiac death in patients with the
accessory pathways usually conduct in both anterograde and
WPW syndrome has been estimated to range from 0.15% to
retrograde directions. Those that conduct in the anterograde
0.39% over 3- to 10-year follow-up. It is unusual for cardiac
direction only are uncommon, whereas those that conduct in
arrest to be the first symptomatic manifestation of WPW
the retrograde direction are common.
syndrome. Conversely, in about half of the cardiac arrest
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
cases in WPW patients, it is the first manifestation of WPW.
3. Long-Term Pharmacologic Therapy
Given the potential for AF among patients with WPW
Antiarrhythmic drugs represent one therapeutic option for
syndrome and the concern about sudden cardiac death result-
management of accessory pathway–mediated arrhythmias,
ing from rapid pre-excited AF, even the low annual incidence
but they have been increasingly replaced by catheter ablation.
of sudden death among patients with the WPW syndrome is
Antiarrhythmic drugs that primarily modify conduction
of note and supports the concept of liberal indications for
through the AV node include digoxin, verapamil, beta block-
catheter ablation.
ers, adenosine, and diltiazem. Antiarrhythmic drugs that
Studies of WPW syndrome patients who have experienced
depress conduction across the accessory pathway include
a cardiac arrest have retrospectively identified a number of
class I drugs, such as procainamide, disopyramide,
markers that identify patients at increased risk. These include
propafenone, and flecainide, as well as class III antiarrhyth-
1) a shortest pre-excited R-R interval less than 250 ms during
mic drugs, such as ibutilide, sotalol, and amiodarone.
spontaneous or induced AF, 2) a history of symptomatic
a. Prophylactic Pharmacologic Therapy
tachycardia, 3) multiple accessory pathways, and 4) Ebstein's
There have been no controlled trials of drug prophylaxis
anomaly. A high incidence of sudden death has been reported
involving patients with AVRT; however, a number of small,
in familial WPW. This familial presentation is, however,
nonrandomized trials have been performed (each involving
exceedingly rare (82). Several noninvasive and invasive tests
less than 50 patients), and they have reported the safety and
have been proposed as useful in risk-stratifying patients for
efficacy of drug therapy for maintenance of sinus rhythm in
sudden death risk. The detection of intermittent pre-
patients with supraventricular arrhythmias. A subset of the
excitation, which is characterized by an abrupt loss of the
patients in these studies had AVRT as their underlying
delta wave and normalization of the QRS complex, is
arrhythmia. Available data do not allow a comparison of the
evidence that an accessory pathway has a relatively long
efficacy of these drugs relative to one another. The drugs
refractory period and is unlikely to precipitate VF. The loss of
available to treat AVRT include any drug that alters either
pre-excitation after administration of the antiarrhythmic drug
conduction through the AV node (eg, nondihydropyridine
procainamide has also been used to indicate a low-risk
calcium-channel blockers, beta blockers, digoxin) or a drug
subgroup. Noninvasive tests are considered inferior to inva-
that alters conduction through the atrium, ventricle, or acces-
sive electrophysiological assessment for risk of sudden car-
sory pathway (eg, class Ia, Ic, or III antiarrhythmic agents).
diac death. For this reason, noninvasive tests currently play
The available data are outlined below. Of note is that no
little role in patient management.
studies have examined the efficacy of chronic oral beta
2. Acute Treatment
blockers in the treatment of AVRT and/or WPW syndrome.
The approach to acute evaluation and management during a
The absence of studies specifically examining the role of
sustained regular tachycardia is covered in Sections IV. A and
beta-blocker therapy in the treatment of WPW syndrome
IV. B. The approach to acute termination of these arrhythmias
likely reflects the fact that catheter ablation is the therapy of
generally differs from that used for long-term suppression
choice for these patients. Despite the absence of data from
and prevention of further episodes of SVT.
clinical trials, chronic oral beta-blocker therapy may be usedfor treatment of patients with WPW syndrome, particularly if
a. Special Considerations for Patients With Wide-Complex
their accessory pathway has been demonstrated during elec-
(Pre-Excited) TachycardiasIn patients with antidromic tachycardia, drug treatment may
trophysiological testing to be incapable of rapid anterograde
be directed at the accessory pathway or at the AV node
because both are critical components of the tachycardia
(1) Propafenone. The largest published study that reported
circuit. Atrioventricular nodal– blocking drugs would, how-
the efficacy of propafenone in adult patients involved 11
ever, be ineffective in patients who have anterograde conduc-
individuals. Propafenone resulted in anterograde conduc-
tion over one pathway and retrograde conduction over a
tion block in the accessory pathway in 4 of 9 patients and
separate accessory pathway because the AV node is not
retrograde block in 3 of 11 patients. Atrioventricular
involved in the circuit. Adenosine should be used with
re-entry tachycardia was rendered noninducible in 6 of 11
caution because it may produce AF with a rapid ventricular
patients. During 9 plus or minus 6 months of follow-up,
rate in pre-excited tachycardias. Ibutilide, procainamide, or
none of the 10 patients discharged on a combination of
flecainide, which are capable of slowing the conduction
propafenone and a beta blocker experienced a recurrence.
through the pathway, are preferred.
No major side effects were reported. Other small trials
Pre-excited tachycardias occurring in patients with either
have evaluated the efficacy of propafenone in the treat-
AT or atrial flutter with a bystander accessory pathway may
ment of AVRT in children. The largest of these involved
present with a one-to-one conduction over the pathway.
41 children. Chronic administration of propafenone waseffective in 69%. Side effects occurred in 25% of these
Caution is advised against AV-nodal– blocking agents, which
would obviously be ineffective in this situation. Antiarrhyth-
(2) Flecainide. A number of studies have examined the acute
mic drugs, which prevent rapid conduction through the
and long-term efficacy of oral and IV flecainide in the
bystander pathway, are preferable, even if they may not
treatment of patients with AVRT. The largest of these
convert the atrial arrhythmia. Similarly, it is preferable to
studies involved 20 patients with AVRT. The oral ad-
treat pre-excited AF by either IV ibutilide, flecainide, or
ministration of flecainide (200 to 300 mg/d) resulted in
an inability to induce sustained tachycardia in 17 of the
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
20 patients. The electrophysiological effects of flecainide
quent and hemodynamically tolerated tachycardia. A recent
were partially reversed by administration of isoprotere-
study reported that 94% of induced PSVT episodes were
nol. During 15 plus or minus 7 months of follow-up on
terminated in the electrophysiology laboratory within 32
oral flecainide treatment, 3 patients developed a recur-
minutes plus or minus 22 minutes by administration of a
rence of tachycardia. Other studies have reported similar
combination of diltiazem (120 mg) plus propranolol (80 mg).
findings. The addition of a beta blocker results in greater
This treatment was successful in terminating PSVT within 2
efficacy, with more than 90% of patients achieving
hours during outpatient follow-up in 81% of patients. Another
abolition of symptomatic tachycardia. In addition tostudies that specifically focused on patients with a known
finding of this study was that flecainide, when given as a
AVRT, several randomized trials have evaluated the
single dose for acute termination of PSVT, was significantly
efficacy of flecainide in the treatment of patients with
less effective than the combination of diltiazem and
PSVT of undetermined tachycardia mechanism. One
study enrolled 34 patients with PSVT into a double-blinded, placebo-controlled trial with an 8-week cross-
4. Catheter Ablation
over trial design. Flecainide was shown to be superior to
Catheter ablation of accessory pathways is performed in
placebo; 8 of the 34 patients had a recurrence during
conjunction with a diagnostic electrophysiological test. The
flecainide therapy, as compared with 29 of 34 patients
purposes of the electrophysiological test are to confirm the
having a recurrence on placebo. Treatment with flecain-
presence of an accessory pathway, determine its conduction
ide also increases the time to first symptomatic event and
characteristics, and define its role in the patient's clinical
time to subsequent events.
arrhythmia. Once the arrhythmia is localized, ablation is
(3) Sotalol. The efficacy of oral sotalol in the prevention of
performed using a steerable ablation catheter. There have
AVRT has been reported in a single study, which
been no prospective, randomized clinical trials that have
involved 17 patients with an accessory pathway. Fourteen
evaluated the safety and efficacy of catheter ablation of
of 15 patients with inducible sustained tachycardia during
accessory pathways; however, the results of catheter ablation
electrophysiological testing continued to have inducibletachycardia after administration of IV sotalol. Thirteen of
of accessory pathways have been reported in a large number
the 16 patients who were discharged taking oral sotalol
of single-center trials, one multicenter trial (57), and several
were free of symptomatic recurrences during a median of
prospective registries (55). The initial efficacy of catheter
36 months of follow-up.
ablation of accessory pathways is approximately 95% in most
(4) Amiodarone. Several studies have evaluated the efficacy
series (57). The success rate for catheter ablation of left
of amiodarone in the treatment of patients with accessory
free-wall accessory pathways is slightly higher than for
pathway–mediated tachycardias. These studies, however,
catheter ablation of accessory pathways in other locations.
do not demonstrate that amiodarone is superior to class Ic
After an initially successful procedure, resolution of the
antiarrhythmic agents or sotalol. As a result of these
inflammation or edema associated with the initial injury
findings, combined with the well-recognized organ tox-
allows recurrence of accessory pathway conduction in ap-
icity associated with amiodarone and the high rate ofdiscontinuation of this drug, amiodarone generally is not
proximately 5% of patients. Accessory pathways that recur
warranted for treatment of patients with accessory path-
can usually be successfully ablated during a second session.
ways. Exceptions are for patients with structural heart
Complications associated with catheter ablation of acces-
disease who are not thought to be candidates for catheter
sory pathways result from radiation exposure, vascular access
(eg, hematomas, deep venous thrombosis, arterial perforation,
(5) Verapamil. The efficacy of verapamil in the prevention of
arteriovenous fistula, pneumothorax), catheter manipulation
AVRT has been reported in a single study, which
(eg, valvular damage, microemboli, perforation of the coro-
involved seven patients. Four of these 17 patients con-
nary sinus or myocardial wall, coronary artery dissection,
tinued to have inducible AVRT during electrophysiolog-
thrombosis), or delivery of RF energy (eg, AV block, myo-
ical testing despite treatment with oral verapamil. Ade-
cardial perforation, coronary artery spasm or occlusion,
quate follow-up data in these patients were not provided
transient ischemic attacks, or cerebrovascular accidents)
in this manuscript. Intravenous verapamil can precipitatehemodynamic deterioration during AF. Verapamil and
(55,57). The procedure-related mortality reported for catheter
diltiazem should not be used as the sole therapy for
ablation of accessory pathways ranges from 0% to 0.2%
patients with accessory pathways that might be capable
(55,57). The voluntary Multicenter European Radiofrequency
of rapid conduction during AF. This concern also applies
Survey (MERFS) reported data from 2222 patients who
to digoxin, which also should not be used in this
underwent catheter ablation of an accessory pathway. The
overall complication rate was 4.4%, including 3 deaths
(6) Other Drugs. No studies have been performed to deter-
(0.13%). The 1995 NASPE survey of 5427 patients who
mine the short- or long-term efficacy of procainamide or
underwent catheter ablations of an accessory pathway re-
quinidine in the treatment of AVRT.
ported a total of 99 (1.82%) significant complications, includ-
b. Single-Dose Oral Therapy (Pill-in-the-Pocket)
ing 4 procedure-related deaths (0.08%). Among the 500
Some patients with infrequent episodes of tachycardia may be
patients who underwent catheter ablation of an accessory
managed with the single-dose "pill-in-the-pocket" approach:
pathway as part of a prospective, multicenter clinical trial,
taking an antiarrhythmic drug only at the onset of a
there was 1 death (0.2%). This patient died of dissection of
tachycardia episode (54). This approach to treatment is
the left main coronary artery during an attempt at catheter
reserved for patients without pre-excitation and with infre-
ablation of a left free-wall accessory pathway (57). The most
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
common major complications are complete AV block and
dynamic instability during their arrhythmia, should undergo
cardiac tamponade. The incidence of inadvertent complete
catheter ablation as first-line therapy. Patients who experi-
AV block ranges from 0.17% to 1.0%. Most occur in the
ence infrequent minimally symptomatic episodes of SVT
setting of attempted ablation of septal accessory pathways
who do not have evidence of pre-excitation can be treated
located close to the AV junction. The frequency of cardiac
with a variety of approaches. These patients with concealed
tamponade varies between 0.13% and 1.1%.
accessory pathways can be managed as patients withAVNRT. Patient preference is always an important consid-
5. Management of Patients With Asymptomatic
eration. Catheter ablation has sufficient efficacy and low risk
to be used for symptomatic patients, either as initial therapy
An ECG pattern of pre-excitation is occasionally encountered
or for patients experiencing side effects or arrhythmia recur-
in a subject who has no symptoms of arrhythmia. The role of
rence during drug therapy. Table 5 lists recommendations for
electrophysiological testing and catheter ablation in asymp-tomatic patients with pre-excitation is controversial. One-
long-term therapy of accessory pathway–mediated
third of asymptomatic individuals younger than 40 years of
age when pre-excitation was identified eventually developed
E. Focal Atrial Tachycardias
symptoms, whereas no patients in whom pre-excitation wasfirst uncovered after the age of 40 years developed symptoms.
1. Definition and Clinical Presentation
Most patients with asymptomatic pre-excitation have a good
Focal ATs are characterized by regular atrial activation from
prognosis; cardiac arrest is rarely the first manifestation of the
atrial areas with centrifugal spread (113). Focal ATs are
disease. Prior studies have reported that approximately 20%
usually manifest by atrial rates between 100 and 250 bpm and
of asymptomatic patients will demonstrate a rapid ventricular
rarely at 300 bpm. Neither the sinus nor the AV node plays a
rate during AF induced during electrophysiological testing.
role in the initiation or perpetuation of the tachycardia.
During follow-up, however, very few patients developed
Nonsustained AT is frequently found on Holter recordings
symptomatic arrhythmias, and none of these individuals
and seldom associated with symptoms. Sustained focal ATs
experienced a cardiac arrest. The positive predictive value of
are relatively rare; they are diagnosed in about 10 to 15% of
invasive electrophysiological testing is considered to be too
patients referred for catheter ablation of SVT (114). The
low to justify routine use in asymptomatic patients (83). The
prevalence of focal AT has been calculated to be 0.34% in
decision to ablate pathways in individuals with high-risk
asymptomatic patients versus 0.46% in symptomatic patients
occupations, such as school bus drivers, pilots, and scuba
divers (83), is made on the basis of individual clinical
The outlook of patients with focal AT is usually benign
considerations. These recommendations are likely to remain
with the exception of incessant forms, which may lead to
unchanged despite the results of a study that identified the
tachycardia-induced cardiomyopathy (116). In adults, focal
results of electrophysiological testing as an important predic-
AT can occur in the absence of cardiac disease, but it is often
tor of arrhythmic events in patients with asymptomatic
associated with underlying cardiac abnormalities (114). Atrial
pre-excitation (84). This study reported the follow-up of 212
tachycardia, usually with AV block, may be produced by
patients with asymptomatic pre-excitation, all of whom un-
digitalis excess. This arrhythmia may be exacerbated by
derwent a baseline electrophysiological study. After 38 plus
hypokalemia. Focal ATs may present as either paroxysmal or
or minus 16 months of follow-up, 33 patients became
symptomatic, and 3 of these patients experienced VF (result-
ing in death in 1 patient). The most important factor in
In ATs, the P waves generally occur in the second half of the
predicting outcome was the inducibility of AVRT or AF
tachycardia cycle (see Section IV-B).Therefore, in ATs, the P
during the baseline electrophysiological study. The presence
wave is frequently obscured by the T wave of the preceding
of multiple accessory pathways was also identified as a
QRS complex (Figure 9). The PR interval is directly influ-
predictor of future arrhythmic events. Of the 115 noninduc-
enced by the tachycardia rate. The presence of AV block
ible patients, only 3.4% developed a symptomatic supraven-
during tachycardia excludes AVRT and makes AVNRT very
tricular arrhythmia during follow-up. In contrast, 62% of the
unlikely. During ATs, an isoelectric baseline is usually
47 inducible patients developed a symptomatic arrhythmia
present between P waves, and it is used to distinguish AT
during follow-up (including the 3 patients who experienced
from typical or atypical flutter (ie, saw-toothed or sinusoidal
P-wave morphologies) (Figures 10 and 11). In the presence of
Patients with asymptomatic pre-excitation should be en-
rapid rates and/or atrial conduction disturbances, however, P
couraged to seek medical expertise whenever arrhythmia-
waves can be very wide without an isoelectric baseline, thus
related symptoms occur. The potential value of electrophys-
mimicking atrial flutter (113). It should also be emphasized
iological testing in identifying high-risk patients who may
that an ECG pattern of AT with discrete P waves and
benefit from catheter ablation must be balanced against the
isoelectric baselines does not rule out macro–re-entrant
approximately 2% risk of a major complication associated
tachycardia, especially if complex structural heart disease is
with catheter ablation.
present and/or there has been surgery for congenital heart
6. Summary of Management
disease. The diagnosis of AT can be established with cer-
In general, patients who have WPW syndrome (ie, pre-
tainty only by an electrophysiological study, including map-
excitation and symptoms), and particularly those with hemo-
ping and entrainment.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Recommendations for Long-Term Therapy of Accessory Pathway–Mediated Arrhythmias
Level of Evidence
WPW syndrome (pre-excitation and
Catheter ablation
symptomatic arrhythmias), well tolerated
Flecainide, propafenone
Sotalol, amiodarone, beta blockers
Verapamil, diltiazem, digoxin
WPW syndrome (with AF and rapid-conduction
Catheter ablation
or poorly tolerated AVRT)
AVRT, poorly tolerated (no pre-excitation)
Catheter ablation
Flecainide, propafenone
Sotalol, amiodarone
Verapamil, diltiazem, digoxin
Single or infrequent AVRT episode(s) (no
diltiazem, beta blockers
Catheter ablation
Sotalol, amiodarone
Flecainide, propafenone
Catheter ablation
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily reflect a preferred
sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines on theManagement of Patients With Atrial Fibrillation.
AF indicates atrial fibrillation; AVRT, atrioventricular reciprocating tachycardia; WPW, Wolff-Parkinson-White.
Although definite localization of the source of AT requires
Focal ATs are characterized by radial spread of activation
intracardiac mapping, the P-wave morphology on the 12-lead
from a focus, with endocardial activation not extending
surface ECG is different from sinus rhythm and may be useful
through the entire atrial cycle. The mechanism of focal
for the determination of the site of origin of the focal AT. A
discharge is difficult to ascertain by clinical methods. Avail-
negative P wave in lead I or aVL, or a positive P wave in lead
able information suggests that focal activity can be caused by
V1, favors a left atrial origin. In addition, negative P waves in
abnormal or enhanced automaticity, triggered activity (due to
the inferior leads are suggestive of a caudal origin, whereas a
delayed afterdepolarization), or micro–re-entry. The progres-
positive P wave in those leads suggests a cranial origin. Of
sive increase in atrial rate with tachycardia onset (ie, "warm-
interest, the P waves during sinus rhythm may be similar to
up") and/or progressive decrease before tachycardia termina-
those originating from the high crista terminalis or right
tion (ie, "cool-down") are suggestive of an automatic
superior pulmonary vein (117). The latter site will, however,
mechanism. Automatic ATs tend to be incessant, especially
often show a positive P wave in lead V1; hence, a change in
in children, whereas those attributed to triggered activity may
P-wave polarity from sinus rhythm should arouse suspicion
be either incessant or paroxysmal.
of a right superior pulmonary vein (PV) site. Multilead body
a. Drug-Induced Atrial Tachycardia
surface potential mapping can be used to help localize the
The drug most commonly associated with induction of focal
tachycardia site of origin (118).
AT is digitalis. This drug-induced AT is usually characterizedby development of AT with AV block; hence, the ventricular
3. Site of Origin and Mechanisms
rate is not excessively rapid. Serum digoxin levels are helpful
Focal ATs are not randomly distributed but rather tend to
for diagnoses. Treatment consists of discontinuing the digi-
cluster over certain anatomical zones. The majority of right-
talis. In cases of persistent advanced AV block, digitalis-
sided ATs originate along the crista terminalis from the
binding agents may be considered.
sinoatrial node to the AV node (119,120). In the left atrium,foci are often found in the pulmonary veins, in the atrial
septum, or on the mitral annulus (121); in many cases, they
The efficacy of antiarrhythmic drugs is poorly defined be-
are generators for AF.
cause the clinical definition of focal ATs is often not very
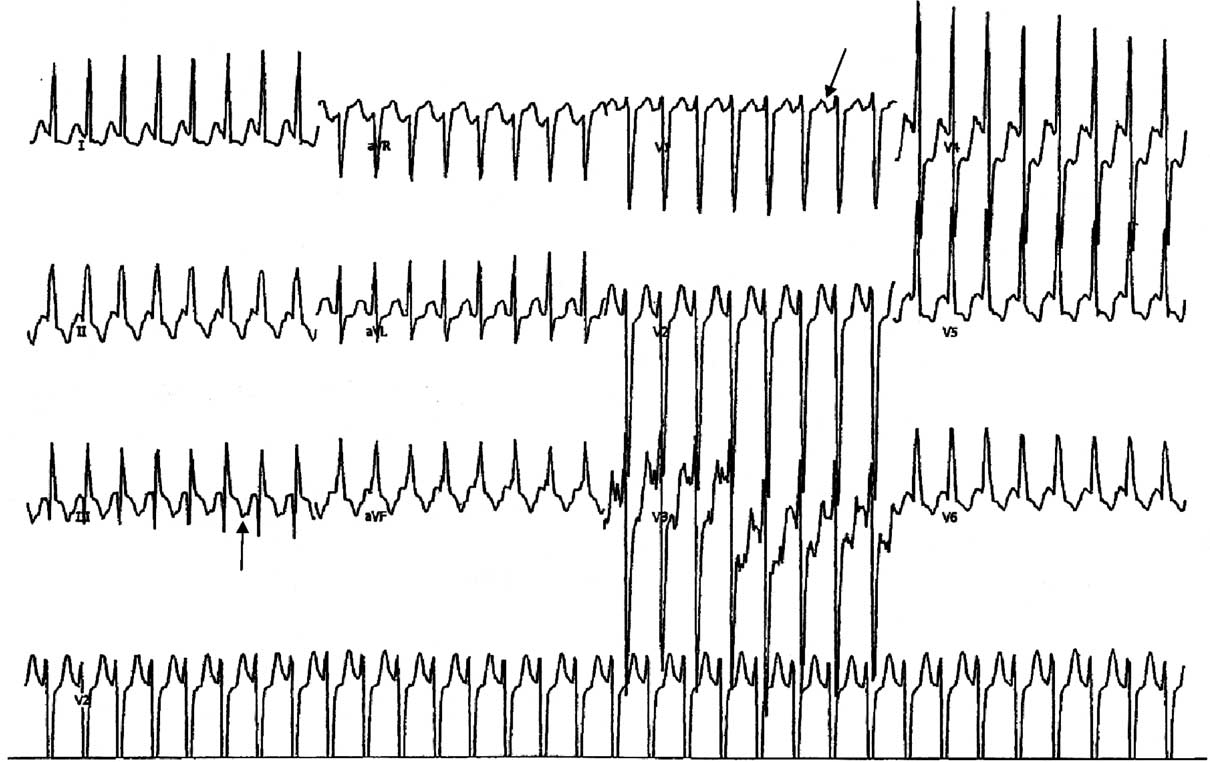
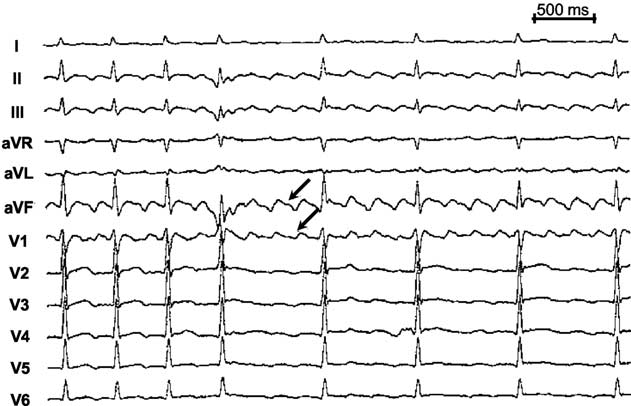
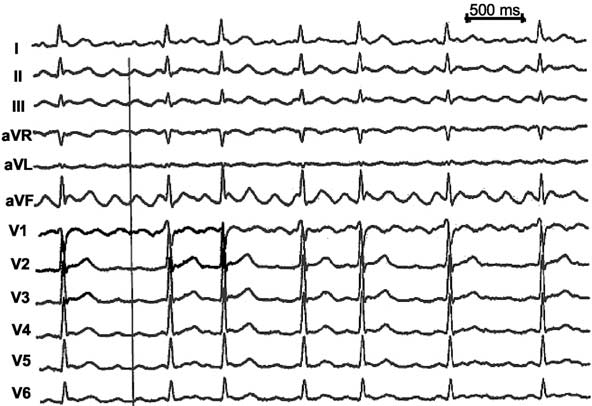
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Figure 9. Focal atrial tachycardia showing a long RP interval relationship. The P wave in AT usually occurs in the latter part of the
tachycardia cycle (arrows) but can appear earlier, depending on the rate and status of AV-nodal conduction. AT indicates atrial
tachycardia; AV, atrioventricular.
rigorous. No large studies have been conducted to assess the
verapamil or beta blockers have been reported. It is
effect of pharmacologic treatment on patients with focal ATs,
conceivable that the mechanism of AT in these patients
but both paroxysmal and incessant ATs are reported to be
relates either to micro–re-entry, involving tissue with slow
difficult to treat medically.
conduction, or to triggered activity. Class Ia or class Icdrugs may suppress automaticity or prolong action-
a. Acute Treatment
potential duration and, hence, may be effective for some
On rare occasions, ATs may be terminated with vagal
patients with AT.
maneuvers. A significant proportion of ATs will terminatewith administration of adenosine. Adenosine-sensitive
For patients with automatic AT, atrial pacing (or adeno-
ATs are usually focal in origin (122,123). Persistence of
sine) may result in transient postpacing slowing but no
the tachycardia with AV block is also a common response
tachycardia termination. Similarly, DC cardioversion seldom
to adenosine. In addition, ATs that are responsive to IV
terminates automatic ATs, but DC cardioversion may besuccessful for those in whom the tachycardia mechanism is
Figure 10. 12-Lead ECG from a patient with counterclockwise
cavotricuspid isthmus– dependent flutter. Note that the flutter
Figure 11. 12-Lead ECG from a patient with clockwise cavotri-
waves in the inferior leads are predominantly negative (arrow),
cuspid isthmus– dependent flutter. Note that the flutter waves
whereas the flutter waves in lead V1 are positive (arrow). ms
are positive in the inferior leads and predominantly negative
double waves in lead V1. ms indicates milliseconds.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
micro–re-entry or triggered automaticity. An attempt at DC
caused by digitalis excess. There is seldom success using
cardioversion should, therefore, be considered for patients
antiarrhythmic agents, but a modicum of success has been
with drug-resistant arrhythmia.
reported using calcium-channel blockers. Beta blockers are
The usual acute therapy for AT consists of IV beta blockers
usually contraindicated because of the presence of severe
or calcium-channel blockers for either termination, which is
underlying pulmonary disease. Therapy is instead directed at
rare, or to achieve rate control through AV block, which is
correction of pulmonary disease and/or electrolyte abnormal-
often difficult to achieve. Direct suppression of the
ities. Chronic therapy often requires use of calcium-channel
tachycardia focus may be achieved by use of IV class Ia and
blockers, as there is no role for DC cardioversion, antiar-
Ic or class III (eg, sotalol, amiodarone) agents. Intravenous
rhythmic drugs, or ablation.
class Ia or Ic agents may be taken by patients without cardiacfailure, whereas IV amiodarone is preferred for those with
F. Macro–Re-entrant Atrial Tachycardia
poor ventricular function (116).
1. Isthmus-Dependent Atrial Flutter
b. Long-Term Pharmacologic Therapy
Atrial flutter is characterized by an organized atrial rhythm
The available studies pertaining to long-term pharmaco-
with a rate typically between 250 and 350 bpm. Electrophys-
logic therapy are observational, and there are problems in
iological studies have shown that this simple ECG definition
discerning whether the tachycardias were carefully differen-
includes tachycardias using a variety of re-entry circuits. The
tiated from other mechanisms (ie, AVRT or AVNRT) or from
re-entry circuits often occupy large areas of the atrium and are
other forms of ATs. Review of the available data supports a
referred to as "macro–re-entrant." The classic type of atrial
recommendation for initial therapy with calcium-channel
flutter (ie, typical flutter) is dependent on the cavotricuspid
blockers or beta blockers because these agents may prove to
isthmus (CTI). The precise type of flutter and, in particular,
be effective and have minimal side effects. If these drugs are
dependence on a defined isthmus (see below) is an important
unsuccessful, then class Ia, class Ic (flecainide and
consideration for catheter ablation but does not alter the
propafenone) in combination with an AV-nodal– blocking
initial approach to management.
agent, or class III agents (sotalol and amiodarone) may betried because they may prove to be effective. The potential
a. Definitions of Cavotricuspid Isthmus–Dependent
benefit should be balanced by the potential risks of proar-
Flutter Circuits
rhythmia and toxicity. Because ATs often occur in older
Isthmus-dependent flutter refers to circuits in which the
patients and in the context of structural heart disease, class Ic
arrhythmia involves the CTI. The most common patterns
agents should be used only after coronary artery disease is
include a tachycardia showing a counterclockwise rotation
(ie, left anterior oblique view) around the tricuspid valve(113). A less common pattern involves clockwise rotation
c. Catheter Ablation
around the tricuspid annulus (ie, reverse typical flutter).
Regardless of whether the arrhythmia is due to abnormal
Counterclockwise atrial flutter is characterized electrocardio-
automaticity, triggering, or micro–re-entry, focal AT is ab-
graphically by dominant negative flutter waves in the inferior
lated by targeting the site of origin of the AT.
leads and a positive flutter deflection in lead V1 with
Pooled data from 514 patients (124) who underwent
transition to a negative deflection in lead V6 at rates of 250
catheter ablation for focal AT showed an 86% success rate,
to 350 bpm (Figure 10). Clockwise isthmus-dependent flutter
with a recurrence rate of 8% (119,125–129). In these series,
shows the opposite pattern (ie, positive flutter waves in the
left atrial origins accounted for 18% of ATs, and 10% of
inferior leads and wide, negative flutter waves in lead V1,
patients had multiple foci. The incidence of significant
transitioning to positive waves in lead V6) (Figure 11).
complications is low (1% to 2%) in experienced centers, but
Patients may at times show unusual ECG patterns; hence,
includes cardiac perforation, damage to the right and left
confirmation of isthmus involvement can be made only by
phrenic nerves and sinus node dysfunction. Ablation of AT
entrainment pacing of the CTI during electrophysiological
from the atrial septum or Koch's triangle may produce AV
For patients with drug refractory AT or incessant AT,
b. Other CTI-Dependent Flutter Circuits
especially, when tachycardia-induced cardiomyopathy has
Isthmus-dependent flutter may also occur as double-wave
developed, the best therapy is catheter ablation of the focus.
or lower-loop re-entry. Double-wave re-entry is defined as a
Table 6 lists recommendations for treatment of focal atrial
circuit in which two flutter waves simultaneously occupy the
usual flutter pathway (144). This arrhythmia is transient,
5. Multifocal Atrial Tachycardia
usually terminating within three to six complexes but may, on
The diagnosis of MAT is made on the basis of finding an
rare occasions, deteriorate into AF (144). Lower-loop re-
irregular tachycardia characterized by three or more different
entry is defined as a flutter circuit in which the re-entry
P-wave morphologies at different rates. The rhythm is always
wavefront circulates around the inferior vena cava due to
irregular and frequently confused with AF, but the rate is not
conduction across the crista terminalis (145–147). The result-
excessively rapid. This arrhythmia is most commonly asso-
ant circuit may produce unusual surface ECG patterns, but
ciated with underlying pulmonary disease but may result
these arrhythmias are still dependent on CTI conduction and,
from metabolic or electrolyte derangements. It is seldom
hence, are amenable to ablation of the isthmus.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Recommendations for Treatment of Focal Atrial Tachycardia*
Clinical Situation
Level of Evidence
Hemodynamically stable patient
Verapamil, diltiazem
Amiodarone, sotalol
B. Rate regulation (in absence of
digitalis therapy)
Verapamil, diltiazem
Recurrent symptomatic AT
Catheter ablation
Beta blockers, calcium-channel
Sotalol, amiodarone
Asymptomatic or symptomatic
Catheter ablation
Nonsustained and asymptomatic
Catheter ablation
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily reflect a preferred
sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines on theManagement of Patients With Atrial Fibrillation.
*Excluded are patients with MAT in whom beta blockers and sotalol are often contraindicated due to pulmonary disease.
†All listed drugs for acute treatment are administered intravenously.
‡Flecainide, propafenone, and disopyramide should not be used unless they are combined with an AV-nodal– blocking agent.
AT indicates atrial tachycardia; DC, direct current; MAT, multifocal atrial tachycardia.
c. Pathophysiology and Treatment Rationale
and orthodromic) in the circuit. In addition, the efficacy of
Cavotricuspid isthmus– dependent flutter is caused by a
pacing can be enhanced by antiarrhythmic drug therapy that
macro–re-entrant right atrial circuit around the tricuspid
facilitates penetration of the circuit by pacing impulses.
annulus. This circuit contains a propagating wavefront and an
Direct current cardioversion is a very effective mode of
excitable gap. The crista terminalis or sinus venosa (ie, area
therapy because of rapid homogeneous depolarization of the
between superior and inferior cava) is thought to be the
entire atrium. The practical implications of these findings are
functional posterior barrier, whereas the tricuspid annulus
discussed in the appropriate therapy sections.
forms the anterior barrier. General mechanisms discussed
d. Clinical Presentation
previously (see Section III) apply to flutter circuits. For
Patients with atrial flutter commonly present with acute
example, class Ia drugs have been shown to decrease con-
symptoms of palpitations, dyspnea, fatigue, or chest pain. In
duction velocity and prolong refractoriness in the flutter
contrast, this arrhythmia may also present with more insidi-
circuit; overall, these drugs tend to shorten the excitable gap.
ous symptoms or conditions, such as exercise-induced fa-
Class Ic drugs depress conduction and can slow flutter. In
tigue, worsening heart failure, or pulmonary disease.
contrast, class III drugs (ie, ibutilide, dofetilide, or amiod-
Atrial flutter occurs in approximately 25% to 35% of
arone) prolong refractoriness and may terminate flutter be-
patients with AF and may be associated with more intense
cause the circulating wavefront encounters tissue that is
symptoms owing to more rapid ventricular rates. In most
refractory. Rapid, atrial overdrive pacing can terminate the
instances, patients with atrial flutter present with a two-to-one
arrhythmia when capturing stimuli penetrate the circuit early
AV-conduction pattern. The flutter rate is approximately 300
enough to produce block in both directions (ie, antidromic
per minute with a ventricular response of 150 bpm. (Flutter
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Figure 12. Management of atrial flutter
depending on hemodynamic stability.
Attempts to electively revert atrial flutter
to sinus rhythm should be preceded and
followed by anticoagulant precautions, as
per AF. AF indicates atrial fibrillation; AV,
atrioventricular; CHF, congestive heart
failure; DC, direct current; MI, myocardial
infarction.
with varying AV block can result in a grossly irregular
hours in duration, anticoagulant therapy is deemed important
rhythm.) In exceptional circumstances, one-to-one AV con-
prior to any mode of cardioversion (see below). Moreover, if
duction may occur in patients during exercise or in those with
acute chemical cardioversion is planned, then rate control is
rapid AV-nodal conduction and may be associated with
desirable because antiarrhythmic drugs, such as class Ic
life-threatening symptoms. Class Ic drugs may, by slowing
agents, may slow the flutter rate and cause a paradoxical
the atrial rate, also cause one-to-one AV conduction and
increase in the ventricular response owing to decreased
should, therefore, be combined with AV-nodal– blocking
concealed conduction into the AV node.
agents. Patients with accessory AV pathways capable of rapid
In approximately 60% of patients, atrial flutter occurs as
conduction also present with rapid ventricular rate and
part of an acute disease process, such as exacerbation of
life-threatening symptoms. Patients with impaired cardiac
pulmonary disease, postoperative cardiac or pulmonary sur-
function, in whom the coordinated contribution of atrial
gery, or during acute myocardial infarction. If the patient
function and regular rate are hemodynamically important, can
survives the underlying disease process, then chronic therapy
experience hemodynamic deterioration with the development
for the arrhythmia is usually not required after sinus rhythm
of atrial flutter even if the ventricular rate is not excessively
is restored. In summary, acute treatment of atrial flutter might
rapid. Atrial flutter, if untreated and accompanied by an
include the initial use of electrical pacing, DC or chemical
excessive ventricular rate, may also by itself promote cardio-
cardioversion, or AV-nodal– blocking agents. The anticipated
myopathy. Hemodynamic deterioration due to atrial flutter is
effects of these modalities are detailed below.
a problem late after repair of congenital heart disease,
(1) Atrioventricular-Nodal–Blocking Agents. Available
particularly after Senning or Fontan operations (148,149). In
randomized, controlled trials of AV-nodal– blocking agents
these patients, flutter is associated with a worse hemodynam-
include patients with AF and atrial flutter. It is often difficult
ic profile and is a marker for worse prognosis.
to isolate the data for atrial flutter patients alone, and the
e. Acute Treatment
general impression is that rate control may be especially
Acute therapy for patients with atrial flutter depends on
difficult to achieve in patients with atrial flutter.
clinical presentation. If the patient presents with acute hemo-
Two randomized, placebo-controlled, double-blinded trials
dynamic collapse or congestive heart failure (CHF), then
assessed use of IV diltiazem for rate control in patients with
emergent DC-synchronized shock is indicated (Figure 12).
AF or atrial flutter. Both studies showed rapid reductions in
Atrial flutter can most often be successfully reverted to sinus
heart rate, but this drug was less effective for rate control in
rhythm with energies less than 50 joules by using monophasic
patients with atrial flutter compared with AF. Hypotension
shocks and with less energy using biphasic shocks. In most
was the chief adverse effect for the group as a whole,
instances, patients present with two-to-one or higher grades
occurring in approximately 10% of patients. A prospective,
of AV block and are hemodynamically stable. In this situa-
randomized, open-labeled trial compared IV diltiazem with
tion, the clinician may elect to use AV-nodal– blocking drugs
IV digoxin for rate control. Rate control was usually achieved
for rate control. Adequate rate control, albeit frequently
within 30 minutes with IV diltiazem compared with more
difficult to achieve, is especially important if conversion to
than 4 hours with IV digoxin.
sinus rhythm is deferred. Atrial overdrive pacing, either
Intravenous verapamil is also efficacious in slowing the
through the transesophageal route or with atrial electrodes, if
ventricular rate. One prospective, randomized, double-
present, should be considered as an option for conversion to
blinded crossover trial compared the safety and efficacy of IV
sinus rhythm. For those with atrial flutter of more than 48
diltiazem and IV verapamil for patients with either AF (7
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
patients) or atrial flutter (10 patients) and decreased ejection
sinus rhythm (151). High-dose (2 mg) ibutilide was more
fraction. In this relatively small sample, both drugs had
effective than sotalol (1.5 mg/kg) in conversion of patients
comparable efficacy in terms of rate control and effect on
with atrial flutter (70% versus 19%) to sinus rhythm.
systolic function. The incidence of symptomatic hypotension,
A review of the existing literature for IV antiarrhythmic
however, was significantly higher for those initially random-
drugs taken by patients with atrial flutter suggests that
ized to IV verapamil.
dofetilide or ibutilide are more effective than sotalol or class
The decrease in heart rate achieved with calcium-channel
I agents but are associated with a significant incidence of
blockers is similar to that observed for IV beta blockers. A
torsades de pointes (1.5% to 3%). Controlled trials have
randomized, open-labeled study comparing IV digoxin to IV
demonstrated the greater efficacy of IV class III agents (eg,
amiodarone showed the superiority of IV amiodarone for
dofetilide, ibutilide) compared with IV amiodarone or class Ia
more rapid achievement of rate control. Intervenous amiod-
(eg, procainamide) or class Ic agents (eg, flecainide,
arone, however, appears to be less effective than IV calcium-
propafenone). Neither IV AV-nodal– blocking agents nor
channel or beta blockers because adequate rate control (ie,
amiodarone appears to be effective for arrhythmia conver-
fewer than100 bpm) was not achieved for 6 hours. In
sion, but they may be effective in rate control.
addition, IV calcium-channel blockers, beta blockers, or
(3) Acute Nonpharmacologic Therapy
amiodarone are seldom associated with conversion of atrial
(i) EXTERNAL DIRECT CURRENT CARDIOVERSION. The suc-
flutter to sinus rhythm.
cess rate for external DC cardioversion for patients with
(2) Acute Intravenous Drugs for Pharmacologic Conver-
flutter is between 95% and 100%. Conversion can often be
sion. A number of drugs have been shown to be effective in
achieved with relatively small amounts of energy (ie, 5 to 50
conversion of atrial flutter to sinus rhythm.
joules), especially when biphasic wave forms are used, but
(i) INTRAVENOUS IBUTILIDE. Placebo-controlled IV ibutilide
higher-energy initial shocks are warranted for emergent
trials show an efficacy rate of 38% to 76% for conversion of
cardioversion of patients with hemodynamic embarrassment.
atrial flutter to sinus rhythm. In these studies, conversion
Direct current cardioversion is the procedure of choice when
rates of atrial flutter were not related to duration of the
rapid termination of flutter is required.
arrhythmia. For patients who responded to ibutilide, the mean
(ii) ATRIAL OVERDRIVE PACING. The use and efficacy of
time to conversion was 30 minutes. The incidence of sus-
rapid atrial pacing to terminate atrial flutter has been long
tained polymorphic VT for the group as a whole was 1.2% to
established, and a comprehensive review showed a cumula-
1.7%; for nonsustained VT (not requiring DC cardioversion),
tive success rate of 82% (range 55% to 100%). Overdrive
the incidence was 1.8% to 6.7%. Randomized, double-
pacing is particularly useful in atrial flutter after cardiac
blinded studies comparing IV ibutilide and IV procainamide
surgery, as these patients frequently have epicardial atrial
are available (150). In the largest study available (150), the
pacing wires. A number of studies have demonstrated the
efficacy of IV ibutilide was significantly greater than that of
efficacy of transesophageal pacing (152,153). In addition, it
IV procainamide for patients with atrial flutter—13 out of 17
has been clearly shown that use of antiarrhythmic drugs,
patients (76%) versus 3 out of 22 (14%). One patient treated
including procainamide (153), ibutilide, and propafenone,
with ibutilide developed polymorphic VT, while 7 of those
may facilitate conversion of atrial flutter by pacing because
treated with procainamide developed hypotension. Procain-
they facilitate impulse penetration of the flutter circuit and
amide was administered at a faster infusion rate in this study
reduce the risk of provoking AF (152). Moreover, high-
than what is recommended, perhaps accounting for the
frequency atrial pacing or overdrive pacing with atrial extra-
hypotension. Intravenous ibutilide should not be taken by
stimuli have been shown to be effective in cases in which
patients with severe structural cardiac diseases or prolonged
atrial overdrive alone is not effective, an option available in
QT interval, or in those with underlying sinus node disease.
most modern pacemaker technologies. It is important to
(ii) INTRAVENOUS CLASS IC DRUGS. Several single-blinded,
recognize that atrial overdrive pacing may result in the
randomized, controlled trials comparing IV flecainide with
induction of sustained AF. In addition, periods of AF may
either IV propafenone or IV verapamil have shown relatively
precede conversion to sinus rhythm.
poor efficacy for acute conversion. In one study, only 13% ofpatients converted after IV flecainide administration; 40%
f. Chronic Pharmacologic Treatment
responded to propafenone (not statistically significant); and
(1) Class I Drugs. It is difficult to evaluate long-term
only 5% reverted with verapamil. Similar results were found
antiarrhythmic therapy for patients with atrial flutter be-
in one additional randomized study comparing IV flecainide
cause most studies combine patients with AF and atrial
with propafenone. Adverse effects included QRS widening,
flutter without specifying the results for each arrhythmia.
dizziness, and paresthesias.
Review of the flecainide database showed the long-term
efficacy of this drug to be 50% for patients with atrial
NTRAVENOUS SOTALOL. A randomized trial of IV
flutter, but the results were available for only 36 patients.
sotalol versus placebo for patients with SVT included only a
Randomized, prospective, long-term trials comparing fle-
limited number of patients with atrial flutter. The conversion
cainide and quinidine are available for patients with AF or
rate varied from 20% to 40%, depending on the sotalol dose,
atrial flutter. No mention is made of patients with atrial
but was not different from placebo. Adverse effects included
flutter as a distinct group, but the incidence of adverse side
hypotension and dyspnea. A large double-blinded, random-
effects for the group as a whole was significantly higher
ized trial involving 308 patients compared IV sotalol with IV
with quinidine compared with flecainide. Beta blockers or
ibutilide for conversion of patients with AF or atrial flutter to
calcium-channel blockers should always be used in con-
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
junction with class Ic agents for treatment of patients with
catheter ablation remained in sinus rhythm. In addition, 63% of
atrial flutter because the class Ic drugs may slow the flutter
patients in the drug-treatment group required one or more
rate and encourage one-to-one AV conduction.
hospitalizations, compared with 22% for those treated with
(2) Class III Drugs. The efficacy of oral dofetilide has been
ablation. Quality of life was significantly improved in those
assessed in several randomized, placebo-controlled trials
treated with ablation.
(154,155). At the highest dose of dofetilide tested (500 g
A number of studies have documented that patients with
twice per day), maintenance of sinus rhythm more than or
AF who are treated with propafenone, flecainide, or amiod-
equal to 350 days occurred in 73% of patients with atrial
arone have a 15% to 20% risk of developing atrial flutter
flutter compared with 40% of patients with AF. Contrain-
(165–167). Prospective trials have shown that, if atrial flutter
dications for dofetilide include creatinine clearance less
becomes the dominant rhythm, then ablation of the CTI and
than 20, hypokalemia, hypomagnesemia, and prolonged
continued use of the antiarrhythmic drug result in a decreased
QT at baseline. Other randomized dose-titration studies
incidence of atrial flutter and facilitate the pharmacologic
have been reported (156) (ie, sotalol), but, unfortunately,
management of AF (168,169). The incidence of AF after
results for the atrial flutter patients are not distinguished
successful ablation of the CTI flutter circuit varies, depending
from those with AF.
on the presence of AF before ablation. For patients with ahistory of only atrial flutter, the occurrence of AF over a
g. Role of Anticoagulant Therapy for Patients With
follow-up of 18 plus or minus 14 months was only 8%. In
Atrial Flutter
contrast, for those with a history (follow-up 20 plus or minus
The role of anticoagulant therapy for patients with AF is
14 months) of both AF and predominant atrial flutter, the
determined on the basis of a number of prospective, random-
recurrent rate of AF was 38%; whereas AF recurred in 86%
ized trials. Such trials are not available for patients with atrial
of those in whom AF predominated prior to ablation. It
flutter. It was initially thought, on the basis of observational
appears that the best results of catheter ablation are achieved
studies, that the risk of embolization during cardioversion for
in patients who have sole or predominant atrial flutter.
atrial flutter was negligible. Observational studies, however,have shown a significant risk of embolization for these
i. Treatment of Atrial Flutter in Special Circumstances
patients, ranging from 1.7% to 7% (157,158).
Atrial fibrillation is the most common arrhythmia, occur-
In addition, a number of studies (159) have shown that the
ring in 20% to 50% of patients who have undergone surgery,
incidence of atrial echo-dense material or clot varies from 0%
depending on the nature of the surgery (ie, higher incidence
to 34% in nonanticoagulated patients with atrial flutter. The
with mitral valve surgery). Likewise, atrial flutter also occurs
incidence of echo-dense material or clot increases with atrial
after cardiac surgery. Pathogenetic factors that may be in-
flutter duration longer than or equal to 48 hours. Another area
volved in the development of postoperative flutter include
of concern is the finding of atrial stunning after conversion of
pericarditis, a change in autonomic tone, or atrial ischemia.
atrial flutter, which appears to persist for several weeks (160).
Because atrial electrodes are usually left in place after cardiac
In several studies, risk factors for development of embolic
surgery, atrial overdrive pacing for conversion to sinus
events were similar to those described for AF (158).
rhythm is often a useful therapeutic technique to restore sinus
In a collective review of the risk of embolization after
rhythm. If this approach fails, then a number of antiarrhyth-
DC cardioversion for atrial flutter, the risk of embolism for
mic drugs have been utilized, and a number of prospective,
inadequately anticoagulated patients was 2.2%, signifi-
randomized, controlled trials have been published using a
cantly lower than that reported for patients with AF (5% to
variety of agents. One randomized, placebo-controlled, drug-
7%) (158). Although randomized, controlled trials of
titration trial used IV ibutilide for 101 postoperative patients
thromboembolic prophylaxis for atrial flutter are not avail-
with atrial flutter (170). The conversion rate for atrial flutter
able, it is our consensus that the guidelines for anticoag-
was 78% (44% for those with AF) and usually occurred
ulation for patients with AF should be extended to those
within 90 minutes of the infusion. Polymorphic VT was
with atrial flutter (144,161). Cardioversion— electrical,
observed in 1.8% of the patients and typically occurred within
chemical, or by ablation—should thus be considered only
several minutes of the ibutilide infusion. Intravenous dofeti-
if the patient is anticoagulated (international normalized
lide has also been reported to be effective for patients with
ratio [INR] equals 2 to 3), the arrhythmia is less than 48
postoperative AF or atrial flutter.
hours in duration, or the transesophageal echocardiography
Atrial flutter may occur in patients with a variety of
(TEE) shows no atrial clots. Negative TEE should be
comorbid conditions. These include chronic lung disease,
followed by anticoagulation, as by itself it is not protective
acute pneumonia, after pulmonary surgery, or as a complica-
tion of acute myocardial infarction. Rate control may be
h. Catheter Ablation of the Cavotricuspid Isthmus for
achieved with either AV-nodal– blockers or IV amiodarone
(171). If the arrhythmia is associated with severe CHF or
A technique for placing lesions between the tricuspid annulus
hypotension, then urgent DC cardioversion is appropriate.
and the inferior vena cava to block the atrial flutter circuit and
2. Non–Cavotricuspid Isthmus–Dependent Atrial Flutter
cure patients with atrial flutter is available. Initially, success was
Atrial flutter caused by macro–re-entry circuits that do not use
deemed present when ablation simply terminated the arrhythmia.
the CTI are less common than CTI-dependent atrial flutter. Most
Using more stringent criteria to prove the existence of bidirec-
are related to an atrial scar that creates conduction block and a
tional conduction block in the CTI results in better chronicsuccess rates (90% to 100%) (162,163). One prospective, ran-
central obstacle for re-entry. Prior cardiac surgery involving the
domized study compared chronic oral antiarrhythmic therapy (in
atrium, such as repair of congenital heart disease, mitral valve
61 patients with atrial flutter) to RF ablation (164). After a mean
surgery, or the atrial maze procedure, is a common cause. The
follow-up of 21 plus or minus 11 months, only 36% of patients
resulting arrhythmias are referred to as "lesion-related macro–
treated with drugs compared with 80% of those treated with
re-entrant ATs (113,172–175)."
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Recommendations for Acute Management of Atrial Flutter
Clinical Status/Proposed Therapy
Level of Evidence
Verapamil or diltiazem
Atrial or transesophageal pacing
Diltiazem or verapamil
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily
reflect a preferred sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer tothe ACC/AHA/ESC Guidelines on the Management of Patients With Atrial Fibrillation.
Cardioversion should be considered only if the patient is anticoagulated (INR equals 2 to 3), the arrhythmia is less than 48 hours
in duration, or the TEE shows no atrial clots.
*All drugs are administered intravenously.
†Digitalis may be especially useful for rate control in patients with heart failure.
‡Ibutilide should not be taken by patients with reduced LV function.
§Flecainide, propafenone, and procainamide should not be used unless they are combined with an AV-nodal– blocking agent.
AV indicates atrioventricular; DC, direct current; INR, international normalized ratio; LV, left ventricular; TEE, transesophageal
Although CTI-dependent flutter is the most common un-
Surgical incisions in the right atrium for repair of atrial
derlying mechanism in these circumstances, it often coexists
septal defects (ASDs) are probably the most common cause
with incisional macro–re-entrant ATs, resulting in multiple
of lesion-related re-entry in adults (113,172,173,176-183).
re-entry circuits.
The incision is often placed in the lateral right atrium; the
The appearance of the flutter waves on ECG usually differs
re-entry wavefront circulates around the incision. A line of
from CTI-dependent flutter but can resemble typical patterns
ablation lesions extending from the inferior margin of the scar
(see Figures 10 and 11) (113). In some cases, discrete P
to the inferior vena cava, or from the superior margin of the
waves are difficult to identify, possibly because of extensive
scar to the SVC, can interrupt the circuit, but it can also be
atrial scar. Definitive diagnosis requires intracardiac
difficult to complete.
In six series, including 134 patients (predominantly young
a. Catheter Ablation and Mapping of Non–Cavotricuspid
adults with various types of surgically corrected congeni-
tal heart disease), ablation abolished arrhythmia recur-
Ablation of non–CTI-dependent flutter can be substantially
rences in 50% to 88% of patients during average follow-up
more difficult than for CTI-dependent flutter. When this type
periods of up to 2 years (172,176 –178). Complications of
of atrial flutter is suspected, such as in patients with congen-
diaphragmatic paralysis caused by phrenic nerve injury
ital heart disease who have had surgery, referral to an
and thromboembolism after conversion from atrial flutter
experienced center should be considered. Cavotricuspid isth-
have occurred.
mus– dependent flutter is common in patients with prior atrial
Macro–re-entry circuits occur in the left atrium, but are much
surgery, and both CTI- and non–CTI-dependent macro–re-
less common than right atrial circuits (113,180,184,185). Abla-
entry circuits often coexist in a single patient (173,176-180).
tion can be effective, but the number of patients studied is small
Successful ablation is dependent on identifying a critical
and the efficacy and adverse effects of ablation are not yet well
portion of the re-entry circuit where it can be interrupted with
defined (184). Tables 7 and 8 list recommendations for acute and
either one or a line of RF applications.
long-term management of atrial flutter.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
Recommendations for Long-Term Management of Atrial Flutter
Clinical Status/Proposed Therapy
Level of Evidence
First episode and well-tolerated atrial flutter
Cardioversion alone
Catheter ablation*
Recurrent and well-tolerated atrial flutter
Catheter ablation*
Amiodarone, sotalol, flecainide,†‡
Poorly tolerated atrial flutter
Catheter ablation*
Atrial flutter appearing after use of class Ic
Catheter ablation*
agents or amiodarone for treatment of AF
Stop current drug and use another
Catheter ablation*
after failed antiarrhythmic drug therapy
The order in which treatment recommendations appear in this table within each class of recommendation does not necessarily reflect a preferred
sequence of administration. Please refer to text for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines on theManagement of Patients With Atrial Fibrillation.
*Catheter ablation of the AV junction and insertion of a pacemaker should be considered if catheter ablative cure is not possible and the patient
fails drug therapy.
†These drugs should not be taken by patients with significant structural cardiac disease. Use of anticoagulants is identical to that described for
‡Flecainide, propafenone, procainamide, quinidine, and disopyramide should not be used unless they are combined with an AV-nodal– blocking
AF indicates atrial fibrillation; AV, atrioventricular; CTI, cavotricuspid isthmus.
VI. Special Circumstances
be regarded as potentially toxic to the fetus and should beavoided if possible, especially during the first trimester. All
A. Pregnancy
currently available antiarrhythmic drugs that are used for
Premature atrial beats are observed in approximately 50% ofpatients during pregnancy, but they are generally benign and
SVT are categorized as class C drugs (using the US Food and
well tolerated. Although sustained arrhythmias are relatively
Drug Administration [FDA] drug classification system), ex-
rare (2 to 3 per 1000) in those who have supraventricular
cept for sotalol (a class B agent) and for atenolol and
arrhythmias, symptomatic exacerbation of paroxysmal SVT
amiodarone (class D agents).
occurs during pregnancy in approximately 20%.
In patients with mild symptoms and structurally normal
The major concern during treatment of SVT during preg-
hearts, no treatment other than reassurance should be pro-
nancy is the potential for adverse effects on the fetus, as all
vided. Antiarrhythmic drug therapy should be used only if
commonly used antiarrhythmic drugs cross the placental
symptoms are intolerable or if the tachycardia causes hemo-
barrier to some extent. Although the first 8 weeks after
dynamic compromise.
conception is the period associated with the greatest terato-
Catheter ablation should be recommended in women with
genic risk, other adverse effects may occur with drug expo-
symptomatic tachyarrhythmias before they contemplate preg-
sure later in pregnancy. The major concern with antiarrhyth-
nancy. Because of the potential problem of recurring
mic drugs taken during the second and third trimesters is the
tachyarrhythmias during pregnancy, the policy of withdraw-
adverse effect on fetal growth and development as well as the
ing antiarrhythmic drugs and resuming them later can be
risk of proarrhythmia. Several of the physiological changes
recommended only as an alternative in selected cases. A
that occur during pregnancy, such as increased cardiac output
large-scale clinical experience with catheter ablation proce-
and blood volume, decreased serum protein concentration,
dures performed during pregnancy will never be reported,
alterations in gastric secretion and motility, and hormonal
although fetal radiation dose and risk from the procedures
stimulation of liver enzymes, can affect absorption, bioavail-
have been calculated (203). Catheter ablation is the procedure
ability, and elimination of many drugs. More careful moni-
of choice for drug-refactory, poorly tolerated SVT. If needed,
toring of the patient and dose adjustments are, therefore,
it should be performed in the second trimester.
necessary because the above-mentioned changes vary inmagnitude during different stages of pregnancy (202).
1. Acute Conversion of Atrioventricular Node–Dependent
As with many other drugs used in pregnancy, use of certain
antiarrhythmic agents has crept into common practice be-
Intravenous adenosine is the drug of choice if vagal maneu-
cause of an absence of reported ill effects, rather than as a
vers fail to terminate an episode of PSVT. This drug has been
result of controlled studies. All antiarrhythmic drugs should
used safely in pregnant women, although most of the reports
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
Recommendations for Treatment Strategies for SVT During Pregnancy
Treatment Strategy
Acute conversion of PSVT
Metoprolol, propranolol
Sotalol,* flecainide†
Quinidine, propafenone,† verapamil
Catheter ablation
The order in which treatment recommendations appear in this table within each class of
recommendation does not necessarily reflect a preferred sequence of administration. Please refer totext for details. For pertinent drug dosing information please refer to the ACC/AHA/ESC Guidelines onthe Management of Patients With Atrial Fibrillation.
*Beta-blocking agents should not be taken in the first trimester, if possible.
†Consider AV-nodal– blocking agents in conjunction with flecainide and propafenone for certain
tachycardias (see Section V).
‡Atenolol is categorized in class C (drug classification for use during pregnancy) by legal authorities
in some European countries.
AV indicates atrioventricular; DC, direct current; PSVT, paroxysmal supraventricular tachycardia.
of adenosine administration were in the second and third
be avoided during the first trimester, if possible. Beta blockers
trimesters (202).
with selective B1 properties are theoretically preferable because
If adenosine fails, then IV propranolol or metoprolol are
they may interfere less with peripheral vasodilatation and uterine
recommended. Intravenous administration of verapamil may
be associated with a greater risk of maternal hypotension and
If the above-mentioned drugs fail, then sotalol may be
subsequent fetal hypoperfusion.
considered. Although sotalol has been used successfully during
Available data suggest that DC cardioversion is safe in all
pregnancy for other indications, the experience is limited; so,
phases of pregnancy and can be used when necessary.
caution is still advised. The reported experience with flecainideis also limited, but it appears to be relatively safe during
2. Prophylactic Antiarrhythmic Drug Therapy
pregnancy (205). The experience with propafenone is even more
If prophylactic drug therapy is needed, then digoxin or a
limited, although no adverse effects to the fetus have been
beta-blocking agent (ie, propranolol or metoprolol) is the
reported when it is taken during the third trimester. Quinidine is
first-line agent. The experience with digoxin is extensive, and
considered to be relatively well tolerated, although isolated cases
it is considered one of the safest antiarrhythmic drugs to take
of adverse effects, such as fetal thrombocytopenia and eighth-
during pregnancy (202); however, its efficacy for arrhythmia
nerve toxicity, have been reported (202). Procainamide is con-
treatment or prophylaxis has never been demonstrated. Propran-
sidered to be well tolerated and appears to be relatively safe for
olol and metoprolol are generally considered to be safe but are
short-term therapy. The use of amiodarone, a category D agent,
best avoided in the first trimester. Rare cases of adverse effects
in pregnancy should be restricted to arrhythmias that are resistant
on the fetus, including bradycardia, hypoglycemia, premature
to other drugs or are life threatening (206). Table 9 lists
labor, and metabolic abnormalities, have been reported but may
recommendations for treatment strategies for SVT during
be secondary to fetal distress in high-risk pregnancies. Prospec-
tive, randomized studies have failed to demonstrate a higher
It should be emphasized that these recommendations rely
incidence of these complications with beta-blocking agents as
mainly on observational data; the cited references are, there-
compared with placebo. The potential for intrauterine growth
fore, not all inclusive.
retardation has been reported with propranolol and has raisedconcerns, especially when it is taken in the first trimester (202).
B. Supraventricular Tachycardias in Adult
Later studies reported growth retardation in babies receiving
Patients With Congenital Heart Disease
atenolol in the first trimester and a higher prevalence of preterm
delivery (204). Atenolol is, therefore, classified as a category D
An increasing number of patients with congenital heart
agent by the FDA. In view of these results, beta blockers should
disease are surviving to adulthood. Supraventricular arrhyth-
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
mias are an important cause of morbidity and, in some of
atrial flutter is likely to be dependent on conduction through
these patients, mortality. In patients who have not had
the CTI and susceptible to catheter ablation. If closure of the
operative repair of their malformation, AF and atrial flutter
ASD is not warranted by hemodynamic criteria, then catheter
are the most common arrhythmias. Increased atrial filling
ablation of the atrial flutter is preferable to surgical closure of
pressures may contribute to the cause of AF or atrial flutter.
the ASD, which is unlikely to abolish the atrial flutter. Ifclosure of the septal defect is warranted in a patient with atrial
Surgical repairs that place incisions in the atria predispose to
flutter, then electrophysiological study with catheter ablation
incisional-related atrial flutter late after surgery.
prior to surgery may still be considered or ablation of the
Many patients warrant referral to an experienced spe-
atrial flutter isthmus may be performed during surgery in a
cialist. The new development of atrial arrhythmias can be
center with experience in arrhythmia surgery.
an indication of deteriorating hemodynamic function,
In patients with prior surgical repair, both CTI-dependent and
which in some cases warrants specific investigation and
non–CTI-dependent (so-called "incisional" or scar) atrial flutter
occasionally operative treatment. An SVT itself dramati-
occur and can coexist in a single patient (113,172,173,176,178 –
cally impairs hemodynamic performance in some patients.
183,210). Management is as discussed above. If catheter abla-
Coexistent sinus node dysfunction is common after surgi-
tion is warranted, then the possibility that the flutter will have a
cal repair of many of these conditions and can be further
non–CTI-dependent mechanism should be considered. Ablation
aggravated by antiarrhythmic therapy, requiring pace-
may be best performed in an experienced center with advanced,three-dimensional mapping equipment for defining non–CTI-
maker implantation to allow management of the supraven-
tricular arrhythmia. Cardiac malformations often increasethe difficulty of pacemaker implantation and catheter
b. Transposition of the Great Vessels
ablation procedures. The presence of intracardiac shunts
Atrial arrhythmias are uncommon late after arterial switch
creates a risk of systemic embolism from clots that may
procedures. The Mustard and Senning repairs reroute sys-
form on pacing leads even though they are in the right-
temic venous blood to the morphological LV that is con-
sided (ie, systemic venous) cardiac chambers.
nected to the pulmonary artery, and they reroute the pulmo-nary venous blood to the morphological right ventricle that is
2. Specific Disorders
connected to the aorta. The atrial surgery is extensive, andsinus node dysfunction is common (211,212). Of 478 patients
a. Atrial Septal Defect
who survived the perioperative period after Mustard repair in
Atrial fibrillation or atrial flutter occurs in approximately 20%
a study reported by Gelatt and coworkers, atrial flutter
of adults who have an unrepaired ASD (207,208). Atrial fibril-
subsequently occurred in 14%, and ectopic AT occurred in
lation, rather than atrial flutter, predominates in the majority;
1% (3 patients). The actuarial rate of atrial flutter at 20 years
incidence increases with patient age. Surgical or percutaneous
after repair was 24%. An even greater incidence of atrial
closure of ASDs associated with pulmonary blood flow/systemic
arrhythmias was observed in earlier series.
blood flow (Qp/Qs) more than 1.5 and or symptoms before the
Loss of coordinated atrial activity and acceleration of rate
age of 40 years may reduce atrial arrhythmias but has little effect
can produce severe symptoms and hemodynamic compro-
after the age of 40 years (207–209).
mise. Development of atrial arrhythmias is also associated
Gatzoulis and coworkers retrospectively reviewed 218
with impaired ventricular function (149,213). For these rea-
adults who had surgical closure of an isolated ASD (207).
sons, development of atrial arrhythmias has been associated
Sustained atrial flutter or AF was present in 19% of patients
with an increased risk of death and sudden death in some, but
prior to surgery, 5% had atrial flutter, 2.8% had AF and atrial
not all, studies (212).
flutter, and 11% had AF. During a mean follow-up of 3.8
Acute management of rapid SVT is as discussed above (see
years, 60% of patients with preoperative AF or atrial flutter
Sections IV and V). These arrhythmias tend to be recurrent,
continued to have arrhythmias, and new AF or atrial flutter
and attempts to maintain sinus rhythm are usually warranted
developed in 2.3% of patients. All of the patients with
due to the hemodynamic compromise produced by the ar-
persistent arrhythmias and those who developed new atrial
rhythmia. Associated ventricular dysfunction and risk of
arrhythmias were older than 40 years of age at the time of
sudden death and sinus node dysfunction can complicate
repair. None of the 106 patients younger than 40 years of age
selection of antiarrhythmic drug therapy. Referral to a spe-
at the time of surgery had late atrial arrhythmias during this
cialist with experience in the care of these patients is usually
follow-up period (P⫽0.008).
warranted. Catheter ablation of the lesion related to the atrial
Attie and coworkers randomized 521 adults older than 40
flutter can be effective but is more difficult than for patients
years of age who had isolated secundum or sinus venosal
without structural heart disease and should be attempted only
ASDs with a Qp/Qs more than 1.7 and pulmonary artery
at experienced centers (210).
systolic pressure less than 70 mm Hg to surgical closureversus medical therapy (208). Prior to randomization, 21% of
c. Tetralogy of Fallot
patients had a history of AF or atrial flutter managed with rate
Atrial incisions are commonly made at the time of repair,
control and anticoagulation, and 5% had a history of other
predisposing to the late development of incisional-related
types of SVT. During a median follow-up of 7.3 years, new
atrial flutter (148,214). During 35 years of follow-up after
atrial flutter or AF developed in 7.4% of patients in the
repair 10% of patients developed atrial flutter, 11% devel-
surgical group and 8.7% of patients in the medical group.
oped sustained VT, and 8% died suddenly (214).
Cerebral embolic events occurred in 2.1% of patients. The
The sinus rhythm ECG shows RBBB in the vast majority
risk was not different between the surgical and medically
of patients, such that SVTs are conducted with RBBB
treated patients.
aberrancy. Ventricular tachycardia arises due to re-entry in
Management of atrial flutter is the same as described in
the region of the right ventricular outflow tract or infundib-
Section V-F. In patients who have not had surgical repair,
ular septum. Although most of these VTs have a QRS
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
TABLE 10.
Recommendations for Treatment of SVTs in Adults With Congenital Heart Disease
Failed antiarrhythmic drugs and
symptomatic:
Catheter ablation in an experienced center
Mustard or Senning repair of
Catheter ablation in an experienced center
transposition of the great vessels
Unrepaired asymptomatic ASD not
Closure of the ASD for treatment of the arrhythmia
Closure of the ASD combined with ablation of the
significant ASD with atrial flutter*
PSVT and Ebstein's anomaly with
Surgical ablation of accessory pathways at the
hemodynamic indications for
time of operative repair of the malformation at an
experienced center
*Conversion and antiarrhythmic drug therapy initial management as described for atrial flutter (see Section V-F).
ASD indicates atrial septal defect; PSVT, paroxysmal supraventricular tachycardia.
configuration resembling LBBB, the VT QRS resembles
iological evaluation is often warranted. Failure to address
RBBB in approximately 25% of patients. An RBBB config-
potential accessory pathways can lead to recurrent arrhyth-
uration of the tachycardia is not, therefore, a reliable guide for
mias and instability in the perioperative period. Catheter
distinguishing a VT from an SVT. Atrial flutter precipitates
ablation prior to surgery is, therefore, recommended. Surgical
hemodynamic compromise in some patients. Acute manage-
division of accessory pathways may be considered as an
ment is dictated by hemodynamic stability (see Section IV.
option for selected patients in centers with experience.
B). Establishment of the correct diagnosis is critical to guide
In general, management of accessory pathways in Eb-
further management. Electrophysiological testing may be
stein's anomaly is as discussed in Section V-D. The associ-
required, and referral to a specialist is advised.
ated malformation and common coexistence of multiple
Atrial flutter can be CTI dependent or incisional related
accessory pathways, however, increase the difficulty of map-
(172,210). Development of atrial flutter can be an indication
ping and ablation. Of 65 patients reported in the Pediatric
of worsening ventricular function and tricuspid regurgitation
Radiofrequency Ablation Registry, short-term success rates
(131,148,214,215). Hemodynamic reassessment of the repair
ranged from 75% to 89%, depending on pathway location
and consideration for revision are sometimes warranted.
(septal versus free wall); late recurrences occurred in up to
Chronic management is as discussed above.
32% of patients (221).
d. Ebstein's Anomaly of the Tricuspid Valve
e. Fontan Repairs
Accessory AV and atriofascicular pathways occur in up to
Incisional-related atrial flutter or AF occurs in up to 57% of
25% of patients and are more often right sided and multiple
patients, depending on the particular type of repair (222,223).
than in patients without the disorder (216 –219). In addition to
Atrial arrhythmias can cause rapid hemodynamic deteriora-
AVRT, AF, atrial flutter, and ectopic AT can occur.
tion and are associated with more heart failure. Acute
Right bundle-branch block is usually present and, in the
management is as discussed for atrial flutter above. Referral
presence of a right-sided accessory pathway, ventricular
to a specialist is advised. Catheter ablation can be effective
pre-excitation can mask the ECG evidence of RBBB. Thus,
but is often difficult due to multiple circuits and should be
patients may present with orthodromic AVRT with RBBB
attempted only at experienced centers. In addition to the low
aberrancy and, after termination of the arrhythmia, there may
success rate of catheter ablation in the Fontan atriopulmonary
be evidence of a right-sided accessory pathway causing
connection, there is a high rate of recurrence after initially
pre-excitation during sinus rhythm. Left bundle-branch
successful ablation procedures, limiting the usefulness of this
block– configuration tachycardias can be due to antidromic
approach (210). Table 10 lists recommendations for treatment
AVRT or conduction over a bystander accessory pathway
of SVTs in adults with congenital heart disease.
during, for example, AT, AVRT, or atrial flutter.
The malformation can be mild, producing no symptoms.
C. Quality-of-Life and Cost Considerations
Alternatively, tricuspid regurgitation and a large ASD can
Improvement of quality of life is usually the major therapeu-
cause cyanosis and hemodynamic compromise that may be
tic goal of treatment for SVT. Although it was reported early
exacerbated by arrhythmias. Depending on the severity of the
that catheter ablation improves quality of life (227,228) and is
malformation and the arrhythmia, SVTs can produce cyanosis
cost effective compared with other strategies, these studies
and severe symptoms or death. Sudden death can also occur
were observational rather than randomized or were limited to
as a consequence of rapid repetitive conduction to the
more symptomatic patients on stable antiarrhythmic medical
ventricles during AF or atrial flutter when an accessorypathway is present (219).
therapy. A later study compared the effect on quality of life
When hemodynamic consequences of the malformation
between catheter ablation and pharmacologic therapy as an
warrant operative correction and supraventricular arrhyth-
initial strategy for patients with SVTs (229). Both treatments
mias are present, arrhythmia management should be coordi-
improved quality of life and decreased frequency of disease-
nated with the surgical team (220). Preoperative electrophys-
specific symptoms, but ablation improved quality of life in
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
more general health categories and resulted in complete
2. Baine WB, Yu W, Weis KA. Trends and outcomes in the hospitalization
amelioration of symptoms in more patients (74% versus 33%)
of older Americans for cardiac conduction disorders or arrhythmias,1991–1998. J Am Geriatr Soc 2001;49:763–70.
than did medication. Potential long-term costs were similar
3. Orejarena LA, Vidaillet H, Jr, DeStefano F, et al. Paroxysmal supraven-
for medication and ablation (229). Among patients who had
tricular tachycardia in the general population. J Am Coll Cardiol 1998;
monthly episodes of SVT, RF ablation was, however, the
31:150 –7.
more effective and less expensive therapy compared with
4. Granada J, Uribe W, Chyou PH, et al. Incidence and predictors of atrial
flutter in the general population. J Am Coll Cardiol 2000;36:2242– 6.
long-term drug therapy (230). Another prospective study
5. Kwong KF, Schuessler RB, Green KG, et al. Differential expression of
compared the long-term effects on health outcome of catheter
gap junction proteins in the canine sinus node. Circ Res 1998;82:
ablation and medical therapy as an initial treatment for
patients with newly documented PSVT, excluding those with
6. Wu J, Schuessler RB, Rodefeld MD, et al. Morphological and
membrane characteristics of spider and spindle cells isolated from rabbit
drug-refractory symptoms referred specifically for ablation
sinus node. Am J Physiol Heart Circ Physiol 2001;280:H1232– 40.
(231). At 5-year follow-up, patients who received ablation
7. Boyett MR, Honjo H, Yamamoto M, et al. Downward gradient in action
had improved quality-of-life scores and a reduction in
potential duration along conduction path in and around the sinoatrial
disease-specific symptoms when compared with patients who
node. Am J Physiol 1999;276:H686 –98.
8. Cheung DW. Electrical activity of the pulmonary vein and its interaction
continued to take medical therapy. More patients reported
with the right atrium in the guinea-pig. J Physiol 1981;314:445–56.
complete elimination of symptoms with ablation therapy
9. Cheung DW. Pulmonary vein as an ectopic focus in digitalis-induced
(70%) than did those taking medical therapy (43%). Over 5
arrhythmia. Nature 1981;294:582– 4.
years, the average cumulative cost for patients in the medical
10. Luchsinger JA, Steinberg JS. Resolution of cardiomyopathy after
ablation of atrial flutter. J Am Coll Cardiol 1998;32:205–10.
therapy group was statistically significantly lower than in
11. Wu EB, Chia HM, Gill JS. Reversible cardiomyopathy after radiofre-
patients initially treated with ablation therapy: $6249 plus or
quency ablation of lateral free- wall pathway-mediated incessant
minus $1421 per patient versus $7507 plus or minus $1098
supraventricular tachycardia. Pacing Clin Electrophysiol 2000;23:1308 –10.
per patient (231). It was concluded that patient preference
12. Crawford MH, Bernstein SJ, Deedwania PC, et al. ACC/AHA
remains the critical determinant in choosing a particular
guidelines for ambulatory electrocardiography: executive summary and
treatment in cases of mildly to moderately symptomatic
recommendations. a report of the American College of Cardiology/
American Heart Association Task Force on Practice Guidelines (Com-mittee to Revise the Guidelines for Ambulatory Electrocardiography).
Baseline quality-of-life scores appear to be lower for
Circulation 1999;100:886 –93.
patients with atrial flutter and AF than for those with other
13. Seidl K, Rameken M, Breunung S, et al. Diagnostic assessment of
arrhythmias who are undergoing RF ablation. Several studies
recurrent unexplained syncope with a new subcutaneously implantable
have described improvement in symptoms and quality of life
loop recorder. Reveal-Investigators. Europace 2000;2:256 – 62.
14. Lee KL, Chun HM, Liem LB, et al. Effect of adenosine and verapamil
after catheter ablation of atrial flutter (164,232–234). Abla-
in catecholamine-induced accelerated atrioventricular junctional
tion of atrial flutter resulted in an improvement in quality of
rhythm: insights into the underlying mechanism. Pacing Clin Electro-
life as well as reductions in symptom-frequency scores and
physiol 1999;22:866 –70.
symptom-severity scores compared with preablation values
15. Glatter KA, Cheng J, Dorostkar P, et al. Electrophysiologic effects of
adenosine in patients with supraventricular tachycardia. Circulation
(234). There was a reduction in the number of patients
1999;99:1034 – 40.
visiting accident and emergency departments, requiring car-
16. Advanced cardiovascular life support: introduction to ACLS 2000:
dioversion, and being admitted to a hospital for a rhythm
overview of recommended changes in ACLS from the Guidelines 2000
problem. Patients with atrial flutter and concomitant AF
Conference (abstr). Circulation 2000;102:I86 –9.
17. Cairns CB, Niemann JT. Intravenous adenosine in the emergency
before ablation and those with atrial flutter alone both derived
department management of paroxysmal supraventricular tachycardia.
significant benefit from atrial flutter ablation (234). Others
Ann Emerg Med 1991;20:717–21.
reported that patients who had atrial flutter associated with
18. Rankin AC, Brooks R, Ruskin JN, et al. Adenosine and the treatment of
AF before ablation had less improvement than those without
supraventricular tachycardia. Am J Med 1992;92:655– 64.
19. Waxman HL, Myerburg RJ, Appel R, et al. Verapamil for control of
AF (233). Moreover, in a prospective, randomized compari-
ventricular rate in paroxysmal supraventricular tachycardia and atrial
son of antiarrhythmic therapy versus first-line RF ablation in
fibrillation or flutter: a double-blind randomized cross-over study. Ann
patients with atrial flutter, the sense of well-being and
Intern Med 1981;94:1– 6.
function in daily life improved after ablation but did not
20. Amsterdam EA, Kulcyski J, Ridgeway MG. Efficacy of cardioselective
beta-adrenergic blockade with intravenously administered metoprolol in
change significantly in patients treated with drugs (164).
the treatment of supraventricular tachyarrhythmias. J Clin Pharmacol
Ablation was associated with a better success rate and effect
1991;31:714 – 8.
on quality of life, a lower occurrence of AF, and a lower need
21. Das G, Tschida V, Gray R, et al. Efficacy of esmolol in the treatment
for rehospitalization at follow-up.
and transfer of patients with supraventricular tachyarrhythmias toalternate oral antiarrhythmic agents. J Clin Pharmacol 1988;31:714 – 8.
22. Holt P, Crick JC, Davies DW, et al. Intravenous amiodarone in the acute
termination of supraventricular arrhythmias. Int J Cardiol 1985;8:67–79.
1. Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC guidelines for
23. Hohnloser SH, Zabel M. Short- and long-term efficacy and safety of
the management of patients with atrial fibrillation: executive summary:
flecainide acetate for supraventricular arrhythmias. Am J Cardiol 1992;
a report of the American College of Cardiology/American Heart Asso-
ciation Task Force on Practice Guidelines and the European Society of
24. Glatter KA, Dorostkar PC, Yang Y, et al. Electrophysiological effects of
Cardiology Committee for Practice Guidelines and Policy Conferences
ibutilide in patients with accessory pathways. Circulation 2001;104:
(Committee to Develop Guidelines for the Management of Patients With
Atrial Fibrillation) Developed in collaboration with the North American
25. Gorgels AP, van den DA, Hofs A et al. Comparison of procainamide and
Society of Pacing and Electrophysiology. Circulation 2001;104:
lidocaine in terminating sustained monomorphic ventricular tachycardia.
Am J Cardiol 1996;78:43– 6.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
26. Manz M, Mletzko R, Jung W, et al. Electrophysiological and haemo-
50. de Paola AA, Horowitz LN, Vattimo AC, et al. Sinus node artery
dynamic effects of lidocaine and ajmaline in the management of sus-
occlusion for treatment of chronic nonparoxysmal sinus tachycardia.
tained ventricular tachycardia. Eur Heart J 1992;13:1123– 8.
Am J Cardiol 1992;70:128 –30.
27. Ho DS, Zecchin RP, Richards DA, et al. Double-blind trial of lignocaine
51. Jayaprakash S, Sparks PB, Vohra J. Inappropriate sinus tachycardia
versus sotalol for acute termination of spontaneous sustained ventricular
(IST): management by radiofrequency modification of sinus node. Aust
tachycardia. Lancet 1994;344:18 –23.
N Z J Med 1997;27:391–7.
28. Part 1: Introduction to the International Guidelines 2000 for CPR and
52. Goya M, Iesaka Y, Takahashi A, et al. Radiofrequency catheter ablation
ECC : a consensus on science. Circulation 2000;102:I1–11.
for sinoatrial node re-entrant tachycardia: electrophysiologic features of
29. Boineau JP, Schuessler RB, Hackel DB, et al. Widespread distribution
ablation sites. Jpn Circ J 1999;63:177– 83.
and rate differentiation of the atrial pacemaker complex. Am J Physiol
53. Tendera M, Wnuk-Wojnar AM, Kulakowski P, et al. Efficacy and safety
of dofetilide in the prevention of symptomatic episodes of paroxysmal
30. Scheinman MM, Levine JH, Cannom DS, et al., for the Intravenous
supraventricular tachycardia: a 6-month double-blind comparison with
Amiodarone Multicenter Investigators Group. Dose-ranging study of
propafenone and placebo. Am Heart J 2001;142:93– 8.
intravenous amiodarone in patients with life-threatening ventricular
54. Alboni P, Tomasi C, Menozzi C, et al. Efficacy and safety of out-of-
hospital self-administered single-dose oral drug treatment in the man-
tachyarrhythmias. Circulation 1995;92:3264 –72.
agement of infrequent, well-tolerated paroxysmal supraventricular
31. Sharma AD, Klein GJ, Yee R. Intravenous adenosine triphosphate
tachycardia. J Am Coll Cardiol 2001;37:548 –53.
during wide QRS complex tachycardia: safety, therapeutic efficacy, and
55. Scheinman MM, Huang S. The 1998 NASPE prospective catheter
diagnostic utility. Am J Med 1990;88:337– 43.
ablation registry. Pacing Clin Electrophysiol 2000;23:1020 – 8.
32. Buxton AE, Marchlinski FE, Doherty JU, et al. Hazards of intravenous
56. Clague JR, Dagres N, Kottkamp H, et al. Targeting the slow pathway for
verapamil for sustained ventricular tachycardia. Am J Cardiol 1987;59:
atrioventricular nodal re-entrant tachycardia: initial results and
long-term follow-up in 379 consecutive patients. Eur Heart J 2001;
33. Ghuran A, Nolan J. Recreational drug misuse: issues for the cardiologist.
57. Calkins H, Yong P, Miller JM, et al., for the Atakr Multicenter Inves-
34. Steinherz L, Yalahom J. Cardiac toxicity. In: DeVita VT, Hellman S,
tigators Group. Catheter ablation of accessory pathways, atrioventricular
Rosenberg SA, editors. Cancer Principles and Practice of Oncology.
nodal re-entrant tachycardia, and the atrioventricular junction: final
Philadelphia, PA: Lippincott Williams and Wilkins, 2001:2904 –21.
results of a prospective, multicenter clinical trial. Circulation 1999;99:
35. Olgin J, Zipes D. Specific arrhythmias: diagnosis and treatment. In:
Braunwald E, Zipes D, editors. Heart Disease: A Textbook of Cardio-
58. Akhtar M, Jazayeri MR, Sra J, et al. Atrioventricular nodal re-entry:
vascular Medicine. Libby P. Philadelphia, PA: Saunders, 2001:815– 89.
clinical, electrophysiological, and therapeutic considerations. Circu-
36. Asnis GM, Hameedi FA, Goddard AW, et al. Fluvoxamine in the
treatment of panic disorder: a multi-center, double-blind, placebo-
59. Mauritson DR, Winniford MD, Walker WS, et al. Oral verapamil for
controlled study in outpatients. Psychiatry Res 2001;103:1–14.
paroxysmal supraventricular tachycardia: a long-term, double-blind ran-
37. Stein DJ, Stein MB, Goodwin W, et al. The selective serotonin reuptake
domized trial. Ann Intern Med 1982;96:409 –12.
inhibitor paroxetine is effective in more generalized and in less gener-
60. Winniford MD, Fulton KL, Hillis LD. Long-term therapy of paroxysmal
alized social anxiety disorder. Psychopharmacology (Berl) 2001;158:
supraventricular tachycardia: a randomized, double-blind comparison of
digoxin, propranolol and verapamil. Am J Cardiol 1984;54:1138 –9.
38. van der Linden GJ, Stein DJ, van Balkom AJ. The efficacy of the
61. Anderson JL, Platt ML, Guarnieri T, et al., for the Flecainide Supraven-
selective serotonin reuptake inhibitors for social anxiety disorder (social
tricular Tachycardia Study Group. Flecainide acetate for paroxysmal
phobia): a meta-analysis of randomized controlled trials. Int Clin Psy-
supraventricular tachyarrhythmias. Am J Cardiol 1994;74:578 – 84.
chopharmacol 2000;15 Suppl 2:S15–23.
62. Pritchett EL, McCarthy EA, Wilkinson WE. Propafenone treatment of
39. Schomig A, Kastrati A, Dirschinger J, et al. for the Stent versus Throm-
symptomatic paroxysmal supraventricular arrhythmias: a randomized,
bolysis for Occluded Coronary Arteries in Patients with Acute Myo-
placebo-controlled, crossover trial in patients tolerating oral therapy.
cardial Infarction Study Investigators. Coronary stenting plus platelet
Ann Intern Med 1991;114:539 – 44.
glycoprotein IIb/IIIa blockade compared with tissue plasminogen acti-
63. Wanless RS, Anderson K, Joy M, et al. Multicenter comparative study
vator in acute myocardial infarction. N Engl J Med 2000;343:385–91.
of the efficacy and safety of sotalol in the prophylactic treatment of
40. The Metoprolol in Dilated Cardiomyopathy (MDC) Trial Study Group.
patients with paroxysmal supraventricular tachyarrhythmias. Am Heart J
3-year follow-up of patients randomised in the metoprolol in dilated
1997;133:441– 6.
cardiomyopathy trial. Lancet 1998;351:1180 –1.
64. Henthorn RW, Waldo AL, Anderson JL, et al., for the Flecainide
41. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised
Supraventricular Tachycardia Study Group. Flecainide acetate prevents
trial. Lancet 1999;353:9 –13.
recurrence of symptomatic paroxysmal supraventricular tachycardia.
Circulation 1991;83:119 –25.
42. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system.
65. UK Propafenone PSVT Study Group. A randomized, placebo-controlled
N Engl J Med 2001;344:501–9.
trial of propafenone in the prophylaxis of paroxysmal supraventricular
43. Cossu SF, Steinberg JS. Supraventricular tachyarrhythmias involving
tachycardia and paroxysmal atrial fibrillation. Circulation 1995;92:
the sinus node: clinical and electrophysiologic characteristics. Prog
Cardiovasc Dis 1998;41:51– 63.
66. Gambhir DS, Bhargava M, Nair M, et al. Comparison of electrophysi-
44. Sato T, Mitamura H, Murata M, et al. Electrophysiologic findings of a
ologic effects and efficacy of single-dose intravenous and long-term oral
patient with inappropriate sinus tachycardia cured by selective radiofre-
amiodarone therapy in patients with AV nodal re-entrant tachycardia.
quency catheter ablation. J Electrocardiol 2000;33:381– 6.
Indian Heart J 1996;48:133–7.
45. Mischke K, Stellbrink C, Hanrath P. Evidence of sinoatrial block as a
67. Bogun F, Knight B, Weiss R, et al. Slow pathway ablation in patients
curative mechanism in radiofrequency current ablation of inappropriate
with documented but noninducible paroxysmal supraventricular
sinus tachycardia. J Cardiovasc Electrophysiol 2001;12:264 –7.
tachycardia. J Am Coll Cardiol 1996;28:1000 – 4.
46. Man KC, Knight B, Tse HF, et al. Radiofrequency catheter ablation of
68. Hamdan MH, Dorostkar P, Scheinman M. Junctional tachycardia and
inappropriate sinus tachycardia guided by activation mapping. J Am
junctional rhythm. In: Zipes D, Jalife J, editors. Cardiac Electrophys-
Coll Cardiol 2000;35:451–7.
iology: From Cell to Bedside. Philadelphia, PA: WB Saunders, 2000:
47. Lee RJ, Kalman JM, Fitzpatrick AP, et al. Radiofrequency catheter
modification of the sinus node for "inappropriate" sinus tachycardia.
69. Kuck KH, Kunze KP, Schluter M, et al. Encainide versus flecainide for
Circulation 1995;92:2919 –28.
chronic atrial and junctional ectopic tachycardia. Am J Cardiol 1988;
48. Yee R, Guiraudon GM, Gardner MJ, et al. Refractory paroxysmal sinus
62:37L– 44L.
tachycardia: management by subtotal right atrial exclusion. J Am Coll
70. Paul T, Reimer A, Janousek J, et al. Efficacy and safety of propafenone
Cardiol 1984;3:400 – 4.
in congenital junctional ectopic tachycardia. J Am Coll Cardiol 1992;
49. Esmailzadeh B, Bernat R, Winkler K, et al. Surgical excision of the
20:911– 4.
sinus node in a patient with inappropriate sinus tachycardia. J Thorac
71. Maragnes P, Fournier A, Davignon A. Usefulness of oral sotalol for the
Cardiovasc Surg 1997;114:861– 4.
treatment of junctional ectopic tachycardia. Int J Cardiol 1992;35:165–7.
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
72. Fidell J, Do-Ngoc D, Attuel P, et al. L'amiodarone dans le traitement des
94. Cockrell JL, Scheinman MM, Titus C, et al. Safety and efficacy of oral
troubles du rythme cardiaque de l'enfant. Arch Mal Coeur Vaiss 1973;
flecainide therapy in patients with atrioventricular re-entrant
2:198 –204.
tachycardia. Ann Intern Med 1991;114:189 –94.
73. Villain E, Vetter VL, Garcia JM, et al. Evolving concepts in the man-
95. Hoff PI, Tronstad A, Oie B, et al. Electrophysiologic and clinical effects
agement of congenital junctional ectopic tachycardia: a multicenter
of flecainide for recurrent paroxysmal supraventricular tachycardia.
study. Circulation 1990;81:1544 –9.
Am J Cardiol 1988;62:585–9.
74. Ehlert FA, Goldberger JJ, Deal BJ, et al. Successful radiofrequency
96. Wiseman MN, Elstob JE, Camm AJ, et al. A study of the use of
energy ablation of automatic junctional tachycardia preserving normal
flecainide acetate in the long-term management of cardiac arrhythmias.
atrioventricular nodal conduction. Pacing Clin Electrophysiol 1993;16:
Pacing Clin Electrophysiol 1990;13:767–75.
97. Benditt DG, Dunnigan A, Buetikofer J, et al. Flecainide acetate for
75. Hamdan M, Van Hare GF, Fisher W, et al. Selective catheter ablation of
long-term prevention of paroxysmal supraventricular tachyarrhythmias.
the tachycardia focus in patients with nonre-entrant junctional
tachycardia. Am J Cardiol 1996;78:1292–7.
98. Pritchett EL, DaTorre SD, Platt ML, et al., for the Flecainide Supraven-
76. Scheinman MM, Gonzalez RP, Cooper MW, et al. Clinical and electro-
tricular Tachycardia Study Group. Flecainide acetate treatment of par-
physiologic features and role of catheter ablation techniques in adult
oxysmal supraventricular tachycardia and paroxysmal atrial fibrillation:
patients with automatic atrioventricular junctional tachycardia. Am J
dose-response studies. J Am Coll Cardiol 1991;17:297–303.
99. Manolis AS, Estes NA, III. Reversal of electrophysiologic effects of
77. Castellanos A, Sung RJ, Myerburg RJ. His bundle electrocardiography
flecainide on the accessory pathway by isoproterenol in the Wolff-
in digitalis-induced "atrioventricular junctional" Wenckebach periods
Parkinson-White syndrome. Am J Cardiol 1989;64:194 – 8.
with irregular H-H intervals. Am J Cardiol 1979;43:653– 6.
100. Kunze KP, Schluter M, Kuck KH. Sotalol in patients with Wolff-
78. Storstein O, Hansteen V, Hatle L, et al. Studies on digitalis: XIII: a
Parkinson-White syndrome. Circulation 1987;75:1050 –7.
prospective study of 649 patients on maintenance treatment with
101. Mason JW. Amiodarone. N Engl J Med 1987;316:455– 66.
digitoxin. Am Heart J 1977;93:434 – 43.
102. Rosenbaum MB, Chiale PA, Ryba D, et al. Control of tachyarrhythmias
79. Fisch C. Myocardial infarction: accelerated junctional rhythm. J Indiana
associated with Wolff-Parkinson-White syndrome by amiodarone
State Med Assoc 1970;63:350.
hydrochloride. Am J Cardiol 1974;34:215–23.
80. Breslow MJ, Evers AS, Lebowitz P. Successful treatment of accelerated
103. Wellens HJ, Lie KI, Bar FW, et al. Effect of amiodarone in the Wolff-
junctional rhythm with propranolol: possible role of sympathetic stim-
Parkinson-White syndrome. Am J Cardiol 1976;38:189 –94.
ulation in the genesis of this rhythm disturbance. Anesthesiology 1985;
104. Kappenberger LJ, Fromer MA, Steinbrunn W, et al. Efficacy of amiod-
62:180 –2.
arone in the Wolff-Parkinson-White syndrome with rapid ventricular
81. Dagres N, Clague JR, Lottkamp H, et al. Impact of radiofrequency
response via accessory pathway during atrial fibrillation. Am J Cardiol
catheter ablation of accessory pathways on the frequency of atrial
1984;54:330 –5.
fibrillation during long-term follow-up; high recurrence rate of atrial
105. Lai WT, Voon WC, Yen HW, et al. Comparison of the electrophysi-
fibrillation in patients older than 50 years of age. Eur Heart J 2001;22:
ologic effects of oral sustained-release and intravenous verapamil in
patients with paroxysmal supraventricular tachycardia. Am J Cardiol
82. Gollob MH, Green MS, Tang AS, et al. Identification of a gene
1993;71:405– 8.
responsible for familial Wolff-Parkinson-White syndrome. N Engl
106. Calkins H, Sousa J, el Atassi R, et al. Diagnosis and cure of the
J Med 2001;344:1823–31.
Wolff-Parkinson-White syndrome or paroxysmal supraventricular
83. Priori SG, Aliot E, Blomstrom-Lundqvist C, et al. Task force on sudden
tachycardias during a single electrophysiologic test. N Engl J Med
cardiac death of the European Society of Cardiology. Eur Heart J
1991;324:1612– 8.
2001;22:1374 – 450.
107. Kuck KH, Schluter M, Geiger M, et al. Radiofrequency current catheter
84. Pappone C, Santinelli V, Rosanio S, et al. Usefulness of invasive
ablation of accessory atrioventricular pathways. Lancet 1991;337:
electrophysiologic testing to stratify the risk of arrhythmic events in
asymptomatic patients with Wolff-Parkinson-White pattern: results from
108. Calkins H, Langberg J, Sousa J, et al. Radiofrequency catheter ablation
a large prospective long-term follow-up study. J Am Coll Cardiol 2003;
of accessory atrioventricular connections in 250 patients: abbreviated
41:239 – 44.
therapeutic approach to Wolff-Parkinson-White syndrome. Circulation
85. Jackman WM, Wang XZ, Friday KJ, et al. Catheter ablation of
1992;85:1337– 46.
accessory atrioventricular pathways (Wolff-Parkinson-White syndrome)by radiofrequency current. N Engl J Med 1991;324:1605–11.
109. Lesh MD, Van Hare GF, Scheinman MM, et al. Comparison of the
86. Manolis AS, Katsaros C, Cokkinos DV. Electrophysiological and elec-
retrograde and transseptal methods for ablation of left free wall
tropharmacologic studies in pre-excitation syndromes: results with
accessory pathways. J Am Coll Cardiol 1993;22:542–9.
propafenone therapy and isoproterenol infusion testing. Eur Heart J
110. Scheinman MM. NASPE survey on catheter ablation. Pacing Clin Elec-
1992;13:1489 –95.
trophysiol 1995;18:1474 – 8.
87. Zipes DP, DiMarco JP, Gillette PC, et al. Guidelines for clinical intra-
111. Hindricks G, for the Multicentre European Radiofrequency Survey
cardiac electrophysiological and catheter ablation procedures: a report of
(MERFS) investigators of the Working Group on Arrhythmias of the
the American College of Cardiology/American Heart Association Task
European Society of Cardiology. The Multicentre European Radiofre-
Force on Practice Guidelines (Committee on Clinical Intracardiac Elec-
quency Survey (MERFS): complications of radiofrequency catheter
trophysiologic and Catheter Ablation Procedures), developed in collab-
ablation of arrhythmias. Eur Heart J 1993;14:1644 –53.
oration with the North American Society of Pacing and Electrophys-
112. Yeh SJ, Lin FC, Chou YY, et al. Termination of paroxysmal supraven-
iology. J Am Coll Cardiol 1995;26:555–73.
tricular tachycardia with a single oral dose of diltiazem and propranolol.
88. Janousek J, Paul T, Reimer A, et al. Usefulness of propafenone for
Circulation 1985;71:104 –9.
supraventricular arrhythmias in infants and children. Am J Cardiol
113. Saoudi N, Cosio F, Waldo A, et al. A classification of atrial flutter and
1993;72:294 –300.
regular atrial tachycardia according to electrophysiological mechanisms
89. Musto B, D'Onofrio A, Cavallaro C, et al. Electrophysiological effects
and anatomical bases; a statement from a joint expert group from The
and clinical efficacy of propafenone in children with recurrent par-
Working Group of Arrhythmias of the European Society of Cardiology
oxysmal supraventricular tachycardia. Circulation 1988;78:863–9.
and the North American Society of Pacing and Electrophysiology. Eur
90. Vignati G, Mauri L, Figini A. The use of propafenone in the treatment
Heart J 2001;22:1162– 82.
of tachyarrhythmias in children. Eur Heart J 1993;14:546 –50.
114. Steinbeck G, Hoffmann E. ‘True' atrial tachycardia. Eur Heart J 1998;19
91. Vassiliadis I, Papoutsakis P, Kallikazaros I, et al. Propafenone in the
Suppl E:E10 –9.
prevention of nonventricular arrhythmias associated with the Wolff-
115. Poutiainen AM, Koistinen MJ, Airaksinen KE, et al. Prevalence and
Parkinson-White syndrome. Int J Cardiol 1990;27:63–70.
natural course of ectopic atrial tachycardia. Eur Heart J 1999;20:
92. Helmy I, Scheinman MM, Herre JM, et al. Electrophysiologic effects of
isoproterenol in patients with atrioventricular re-entrant tachycardia
116. Wren C. Incessant tachycardias. Eur Heart J 1998;19 Suppl E:E32–59.
treated with flecainide. J Am Coll Cardiol 1990;16:1649 –55.
117. Lee SH, Tai CT, Lin WS, et al. Predicting the arrhythmogenic foci of
93. Kim SS, Lal R, Ruffy R. Treatment of paroxysmal re-entrant supraven-
atrial fibrillation before atrial transseptal procedure: implication for
tricular tachycardia with flecainide acetate. Am J Cardiol 1986;58:80 –5.
catheter ablation. J Cardiovasc Electrophysiol 2000;11:750 –7.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
118. SippensGroenewegen A, Peeters HA, Jessurun ER, et al. Body surface
143. Pool PE, Quart BD. Treatment of ectopic atrial arrhythmias and pre-
mapping during pacing at multiple sites in the human atrium: P-wave
mature atrial complexes in adults with encainide. Am J Cardiol 1988;
morphology of ectopic right atrial activation. Circulation 1998;97:
144. Cheng J, Scheinman MM. Acceleration of typical atrial flutter due to
119. Kalman JM, Olgin JE, Karch MR, et al. "Cristal tachycardias": origin of
double-wave re-entry induced by programmed electrical stimulation.
right atrial tachycardias from the crista terminalis identified by intra-
Circulation 1998;97:1589 –96.
cardiac echocardiography. J Am Coll Cardiol 1998;31:451–9.
145. Cheng J, Cabeen WR Jr., Scheinman MM. Right atrial flutter due to
120. Tada H, Nogami A, Naito S, et al. Simple electrocardiographic criteria
lower loop re-entry: mechanism and anatomic substrates. Circulation
for identifying the site of origin of focal right atrial tachycardia. Pacing
1999;99:1700 –5.
Clin Electrophysiol 1998;21:2431–9.
146. Yang Y, Cheng J, Bochoeyer A, et al. Atypical right atrial flutter
121. Hoffmann E, Reithmann C, Nimmermann P, et al. Clinical experience
patterns. Circulation 2001;103:3092– 8.
with electroanatomic mapping of ectopic atrial tachycardia. Pacing Clin
147. Friedman PA, Luria D, Fenton AM, et al. Global right atrial mapping of
Electrophysiol 2002;25:49 –56.
human atrial flutter: the presence of posteromedial (sinus venosa region)
122. Lai LP, Lin JL, Chen TF, et al. Clinical, electrophysiological character-
functional block and double potentials: a study in biplane fluoroscopy
istics, and radiofrequency catheter ablation of atrial tachycardia near the
and intracardiac echocardiography. Circulation 2000;101:1568 –77.
apex of Koch's triangle. Pacing Clin Electrophysiol 1998;21:367–74.
148. Li W, Somerville J. Atrial flutter in grown-up congenital heart (GUCH)
123. Markowitz SM, Stein KM, Mittal S, et al. Differential effects of aden-
patients: clinical characteristics of affected population. Int J Cardiol
osine on focal and macrore-entrant atrial tachycardia. J Cardiovasc
2000;75:129 –37.
Electrophysiol 1999;10:489 –502.
149. Puley G, Siu S, Connelly M, et al. Arrhythmia and survival in patients
124. Hsieh MH, Chen SA. Catheter ablation of focal AT. In: Zipes DP,
⬎18 years of age after the mustard procedure for complete transposition
Haissaguerre M, editors. Catheter Ablation of Arrhythmias. Armonk,
of the great arteries. Am J Cardiol 1999;83:1080 – 4.
NY: Futura Publishing Co., Inc., 2002:185–204.
150. Volgman AS, Carberry PA, Stambler B, et al. Conversion efficacy and
125. Chen SA, Tai CT, Chiang CE, et al. Focal atrial tachycardia: reanalysis
safety of intravenous ibutilide compared with intravenous procainamide
of the clinical and electrophysiologic characteristics and prediction of
in patients with atrial flutter or fibrillation. J Am Coll Cardiol 1998;31:
successful radiofrequency ablation. J Cardiovasc Electrophysiol 1998;
9:355– 65.
151. Vos MA, Golitsyn SR, Stangl K, et al., for the Ibutilide/Sotalol Com-
126. Schmitt C, Zrenner B, Schneider M, et al. Clinical experience with a
parator Study Group. Superiority of ibutilide (a new class III agent) over
novel multielectrode basket catheter in right atrial tachycardias. Circu-
DL-sotalol in converting atrial flutter and atrial fibrillation. Heart 1998;79:568 –75.
lation 1999;99:2414 –22.
152. Doni F, Manfredi M, Piemonti C, et al. New onset atrial flutter termi-
127. Natale A, Breeding L, Tomassoni G, et al. Ablation of right and left
nation by overdrive transoesophageal pacing: effects of different pro-
ectopic atrial tachycardias using a three-dimensional nonfluoroscopic
tocols of stimulation. Europace 2000;2:292– 6.
mapping system. Am J Cardiol 1998;82:989 –92.
153. Rostas L, Antal K, Putorek Z. Transesophageal pacemaker therapy in
128. Weiss C, Willems S, Cappato R, et al. High frequency current ablation
atrial flutter after procainamide pretreatment. Am J Ther 1999;6:
of ectopic atrial tachycardia: different mapping strategies for local-
ization of right- and left-sided origin. Herz 1998;23:269 –79.
154. Singh S, Zoble RG, Yellen L, et al. Efficacy and safety of oral dofetilide
129. Anguera I, Brugada J, Roba M, et al. Outcomes after radiofrequency
in converting to and maintaining sinus rhythm in patients with chronic
catheter ablation of atrial tachycardia. Am J Cardiol 2001;87:886 –90.
atrial fibrillation or atrial flutter: the symptomatic atrial fibrillation
130. Engelstein ED, Lippman N, Stein KM, et al. Mechanism-specific effects
investigative research on dofetilide (SAFIRE-D) study. Circulation
of adenosine on atrial tachycardia. Circulation 1994;89:2645–54.
131. Harrison DA, Siu SC, Hussain F, et al. Sustained atrial arrhythmias in
155. Pedersen OD, Bagger H, Keller N, et al. Efficacy of dofetilide in the
adults late after repair of tetralogy of fallot. Am J Cardiol 2001;87:
treatment of atrial fibrillation-flutter in patients with reduced left ven-
tricular function: a Danish investigations of arrhythmia and mortality on
132. Stock JP. Beta adrenergic blocking drugs in the clinical management of
dofetilide (diamond) substudy. Circulation 2001;104:292– 6.
cardiac arrhythmias. Am J Cardiol 1966;18:444 –9.
156. Benditt DG, Williams JH, Jin J, et al., for the d,l-Sotalol Atrial Fibril-
133. Kunze KP, Kuck KH, Schluter M, et a;. Effect of encainide and fle-
lation/Flutter Study Group. Maintenance of sinus rhythm with oral
cainide on chronic ectopic atrial tachycardia. J Am Coll Cardiol 1986;
d,l-sotalol therapy in patients with symptomatic atrial fibrillation and/or
7:1121– 6.
atrial flutter. Am J Cardiol 1999;84:270 –7.
134. Berns E, Rinkenberger RL, Jeang MK, et al. Efficacy and safety of
157. Dunn MI. Thrombolism with atrial flutter. Am J Cardiol 1998;82:638.
flecainide acetate for atrial tachycardia or fibrillation. Am J Cardiol
158. Seidl K, Hauer B, Schwick NG, et al. Risk of thromboembolic events in
1987;59:1337– 41.
patients with atrial flutter. Am J Cardiol 1998;82:580 –3.
135. Coumel P, Leclercq JF, Assayag P. European experience with the
159. Weiss R, Marcovitz P, Knight BP, et al. Acute changes in spontaneous
antiarrhythmic efficacy of propafenone for supraventricular and ventric-
echo contrast and atrial function after cardioversion of persistent atrial
ular arrhythmias. Am J Cardiol 1984;54:60D– 6D.
flutter. Am J Cardiol 1998;82:1052–5.
136. Lesh MD, Kalman JM, Olgin JE. New approaches to treatment of atrial
160. Sparks PB, Jayaprakash S, Vohra JK, et al. Left atrial "stunning"
flutter and tachycardia. J Cardiovasc Electrophysiol 1996;7:368 – 81.
following radiofrequency catheter ablation of chronic atrial flutter. J Am
137. Beaufort-Krol GC, Bink-Boelkens MT. Sotalol for atrial tachycardias
Coll Cardiol 1998;32:468 –75.
after surgery for congenital heart disease. Pacing Clin Electrophysiol
161. Lip GY, Kamath S. Thromboprophylaxis for atrial flutter. Eur Heart J
2001;22:984 –7.
138. Carrasco HA, Vicuna AV, Molina C, et al. Effect of low oral doses of
162. Willems S, Weiss C, Ventura R, et al. Catheter ablation of atrial flutter
disopyramide and amiodarone on ventricular and atrial arrhythmias of
guided by electroanatomic mapping (CARTO): a randomized com-
chagasic patients with advanced myocardial damage. Int J Cardiol 1985;
parison to the conventional approach. J Cardiovasc Electrophysiol 2000;
139. Kopelman HA, Horowitz LN. Efficacy and toxicity of amiodarone for
163. Kottkamp H, Hugl B, Krauss B, et al. Electromagnetic versus fluoro-
the treatment of supraventricular tachyarrhythmias. Prog Cardiovasc Dis
scopic mapping of the inferior isthmus for ablation of typical atrial
1989;31:355– 66.
flutter: a prospective randomized study. Circulation 2000;102:2082– 6.
140. Prager NA, Cox JL, Lindsay BD, et al. Long-term effectiveness of
164. Natale A, Newby KH, Pisano E, et al. Prospective randomized com-
surgical treatment of ectopic atrial tachycardia. J Am Coll Cardiol
parison of antiarrhythmic therapy versus first-line radiofrequency
ablation in patients with atrial flutter. J Am Coll Cardiol 2000;35:
141. Chen SA, Chiang CE, Yang CJ, et al. Sustained atrial tachycardia in
1898 –904.
adult patients: electrophysiological characteristics, pharmacologic
165. Schumacher B, Jung W, Lewalter T, et al. Radiofrequency ablation of
response, possible mechanisms, and effects of radiofrequency ablation.
atrial flutter due to administration of class IC antiarrhythmic drugs for
atrial fibrillation. Am J Cardiol 1999;83:710 –3.
142. Creamer JE, Nathan AW, Camm AJ. Successful treatment of atrial
166. Tai CT, Chiang CE, Lee SH, et al. Persistent atrial flutter in patients
tachycardias with flecainide acetate. Br Heart J 1985;53:164 – 6.
treated for atrial fibrillation with amiodarone and propafenone: electro-
Blomström-Lundqvist et al.
JACC Vol. 42, No. 8, 2003
ACC/AHA/ESC Guidelines for Management of SVA
October 15, 2003:1493–531
physiologic characteristics, radiofrequency catheter ablation, and risk
191. Kingma JH, Suttorp MJ. Acute pharmacologic conversion of atrial
prediction. J Cardiovasc Electrophysiol 1999;10:1180 –7.
fibrillation and flutter: the role of flecainide, propafenone, and verap-
167. Nabar A, Rodriguez LM, Timmermans C, et al. Radiofrequency ablation
amil. Am J Cardiol 1992;70:56A– 60A.
of "class IC atrial flutter" in patients with resistant atrial fibrillation.
192. Stambler BS, Wood MA, Ellenbogen KA, et al., for the Ibutilide Repeat
Am J Cardiol 1999;83:785–7.
Dose Study Investigators. Efficacy and safety of repeated intravenous
168. Reithmann C, Hoffmann E, Spitzlberger G, et al. Catheter ablation of
doses of ibutilide for rapid conversion of atrial flutter or fibrillation.
atrial flutter due to amiodarone therapy for paroxysmal atrial fibrillation.
Eur Heart J 2000;21:565–72.
193. Ellenbogen KA, Stambler BS, Wood MA, et al. Efficacy of intravenous
169. Huang DT, Monahan KM, Zimetbaum P, et al. Hybrid pharmacologic
ibutilide for rapid termination of atrial fibrillation and atrial flutter: a
and ablative therapy: a novel and effective approach for the management
dose-response study. J Am Coll Cardiol 1996;28:130 – 6.
of atrial fibrillation. J Cardiovasc Electrophysiol 1998;9:462–9.
194. Sung RJ, Tan HL, Karagounis L, et al., for the Sotalol Multicenter Study
170. VanderLugt JT, Mattioni T, Denker S, et al. Efficacy and safety of
Group. Intravenous sotalol for the termination of supraventricular
ibutilide fumarate for the conversion of atrial arrhythmias after cardiac
tachycardia and atrial fibrillation and flutter: a multicenter, randomized,
surgery. Circulation 1999;100:369 –75.
double-blind, placebo-controlled study. Am Heart J 1995;129:739 – 48.
171. Delle KG, Geppert A, Neunteufl T, et al. Amiodarone versus diltiazem
195. Hou ZY, Chang MS, Chen CY, et al. Acute treatment of recent-onset
for rate control in critically ill patients with atrial tachyarrhythmias. Crit
atrial fibrillation and flutter with a tailored dosing regimen of intrave-
Care Med 2001;29:1149 –53.
nous amiodarone: a randomized, digoxin-controlled study. Eur Heart J
172. Nakagawa H, Shah N, Matsudaira K, et al. Characterization of re-entrant
1995;16:521– 8.
circuit in macrore-entrant right atrial tachycardia after surgical repair of
196. Schreck DM, Rivera AR, Tricarico VJ. Emergency management of atrial
congenital heart disease: isolated channels between scars allow "focal"
fibrillation and flutter: intravenous diltiazem versus intravenous digoxin.
ablation. Circulation 2001;103:699 –709.
Ann Emerg Med 1997;29:135– 40.
173. Shah D, Jais P, Takahashi A, et al. Dual-loop intra-atrial re-entry in
197. Platia EV, Michelson EL, Porterfield JK, et al. Esmolol versus verap-
humans. Circulation 2000;101:631–9.
amil in the acute treatment of atrial fibrillation or atrial flutter. Am J
174. Triedman JK, Alexander ME, Berul CI, et al. Electroanatomic mapping
of entrained and exit zones in patients with repaired congenital heart
198. Goldenberg IF, Lewis WR, Dias VC, et al. Intravenous diltiazem for the
disease and intra-atrial re-entrant tachycardia. Circulation 2001;103:
treatment of patients with atrial fibrillation or flutter and moderate to
severe congestive heart failure. Am J Cardiol 1994;74:884 –9.
175. Triedman JK, Saul JP, Weindling SN, et al. Radiofrequency ablation of
199. Chen SA, Chiang CE, Wu TJ, et al. Radiofrequency catheter ablation of
intra-atrial re-entrant tachycardia after surgical palliation of congenital
common atrial flutter: comparison of electrophysiologically guided focal
heart disease. Circulation 1995;91:707–14.
ablation technique and linear ablation technique. J Am Coll Cardiol
176. Akar JG, Kok LC, Haines DE, et al. Coexistence of type I atrial flutter
1996;27:860 – 8.
and intra-atrial re-entrant tachycardia in patients with surgically cor-
200. Naccarelli GV, Dorian P, Hohnloser SH, et al, for the Flecainide Mul-
rected congenital heart disease. J Am Coll Cardiol 2001;38:377– 84.
ticenter Atrial Fibrillation Study Group. Prospective comparison of
177. Chan DP, Van Hare GF, Mackall JA, et al. Importance of atrial flutter
flecainide versus quinidine for the treatment of paroxysmal atrial fibril-
isthmus in postoperative intra-atrial re-entrant tachycardia. Circulation
lation/flutter. Am J Cardiol 1996;77:53A–9A.
201. Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC guidelines for
178. Delacretaz E, Ganz LI, Soejima K, et al. Multi atrial macro-re-entry
the management of patients with atrial fibrillation: a report of the
circuits in adults with repaired congenital heart disease: entrainment
American College of Cardiology/American Heart Association Task
mapping combined with three-dimensional electroanatomic mapping.
Force on Practice Guidelines and the European Society of Cardiology
J Am Coll Cardiol 2001;37:1665–76.
Committee for Practice Guidelines and Policy Conferences (Committee
179. Duru F, Hindricks G, Kottkamp H. Atypical left atrial flutter after
to Develop Guidelines for the Management of Patients With Atrial
intraoperative radiofrequency ablation of chronic atrial fibrillation: suc-
Fibrillation), developed in collaboration with the North American
cessful ablation using three-dimensional electroanatomic mapping.
Society of Pacing and Electrophysiology. Eur Heart J 2001;22:
J Cardiovasc Electrophysiol 2001;12:602–5.
180. Thomas SP, Nunn GR, Nicholson IA, et al. Mechanism, localization and
202. Joglar JA, Page RL. Treatment of cardiac arrhythmias during pregnancy:
cure of atrial arrhythmias occurring after a new intraoperative endo-
safety considerations. Drug Saf 1999;20:85–94.
cardial radiofrequency ablation procedure for atrial fibrillation. J AmColl Cardiol 2000;35:442–50.
203. Damilakis J, Theocharopoulos N, Perisinakis K, et al. Conceptus
181. Hebe J, Hansen P, Ouyang F, et al. Radiofrequency catheter ablation of
radiation dose and risk from cardiac catheter ablation procedures. Cir-
tachycardia in patients with congenital heart disease. Pediatr Cardiol
204. Lydakis C, Lip GY, Beevers M, et al. Atenolol and fetal growth in
182. Kall JG, Rubenstein DS, Kopp DE, et al. Atypical atrial flutter origi-
pregnancies complicated by hypertension. Am J Hypertens 1999;12:
nating in the right atrial free wall. Circulation 2000;101:270 –9.
183. Molenschot M, Ramanna H, Hoorntje T, et al. Catheter ablation of
205. Simpson JM, Sharland GK. Fetal tachycardias: management and
incisional atrial tachycardia using a novel mapping system: LocaLisa.
outcome of 127 consecutive cases. Heart 1998;79:576 – 81.
Pacing Clin Electrophysiol 2001;24:1616 –22.
206. Bartalena L, Bogazzi F, Braverman LE, et al. Effects of amiodarone
184. Jais P, Shah DC, Haissaguerre M, et al. Mapping and ablation of left
administration during pregnancy on neonatal thyroid function and sub-
atrial flutters. Circulation 2000;101:2928 –34.
sequent neurodevelopment. J Endocrinol Invest 2001;24:116 –30.
185. Tai CT, Lin YK, Chen SA. Atypical atrial flutter involving the isthmus
207. Gatzoulis MA, Freeman MA, Siu SC, et al. Atrial arrhythmia after
between the right pulmonary veins and fossa ovalis. Pacing Clin Elec-
surgical closure of atrial septal defects in adults. N Engl J Med 1999;
trophysiol 2001;24:384 –7.
340:839 – 46.
186. Tucker KJ, Wilson C. A comparison of transoesophageal atrial pacing
208. Attie F, Rosas M, Granados N, et al. Surgical treatment for secundum
and direct current cardioversion for the termination of atrial flutter: a
atrial septal defects in patients ⬎40 years old: a randomized clinical
prospective, randomised clinical trial. Br Heart J 1993;69:530 –5.
trial. J Am Coll Cardiol 2001;38:2035– 42.
187. Doni F, Della BP, Kheir A, et al. Atrial flutter termination by overdrive
209. Donti A, Bonvicini M, Placci A, et al. Surgical treatment of secundum
transesophageal pacing and the facilitating effect of oral propafenone.
atrial septal defect in patients older than 50 years. Ital Heart J 2001;2:
Am J Cardiol 1995;76:1243– 6.
188. Doni F, Staffiere E, Manfredi M, et al. Type II atrial flutter interruption
210. Triedman JK, Alexander ME, Love BA, et al. Influence of patient
with transesophageal pacing: use of propafenone and possible change of
factors and ablative technologies on outcomes of radiofrequency
the substrate. Pacing Clin Electrophysiol 1996;19:1958 – 61.
ablation of intra-atrial re-entrant tachycardia in patients with congenital
189. Lown B. Electrical reversion of cardiac arrhythmias. Br Heart J 1967;
heart disease. J Am Coll Cardiol 2002;39:1827–35.
29:469 – 89.
211. Gatzoulis MA, Walters J, McLaughlin PR, et al. Late arrhythmia in
190. Suttorp MJ, Kingma JH, Jessurun ER, et al. The value of class IC
adults with the mustard procedure for transposition of great arteries: a
antiarrhythmic drugs for acute conversion of paroxysmal atrial fibril-
surrogate marker for right ventricular dysfunction? Heart 2000;84:
lation or flutter to sinus rhythm. J Am Coll Cardiol 1990;16:1722–7.
JACC Vol. 42, No. 8, 2003
Blomström-Lundqvist et al.
October 15, 2003:1493–531
ACC/AHA/ESC Guidelines for Management of SVA
212. Sarkar D, Bull C, Yates R, et al. Comparison of long-term outcomes of
of multiple macrore-entrant circuits using fluoroscopically based three-
atrial repair of simple transposition with implications for a late arterial
dimensional endocardial mapping. J Cardiovasc Electrophysiol 1997;8:
switch strategy. Circulation 1999;100:II176 – 81.
213. Li W, Somerville J, Gibson DG, et al. Disturbed atrioventricular elec-
226. Misaki T, Watanabe G, Iwa T, et al. Surgical treatment of patients with
tromechanical function long after Mustard operation for transposition of
Wolff-Parkinson-White syndrome and associated Ebstein's anomaly.
great arteries: a potential contributing factor to atrial flutter. J Am Soc
J Thorac Cardiovasc Surg 1995;110:1702–7.
Echocardiogr 2001;14:1088 –93.
227. Bubien RS, Knotts-Dolson SM, Plumb VJ, et al. Effect of radiofre-
214. Gatzoulis MA, Balaji S, Webber SA, et al. Risk factors for arrhythmia
quency catheter ablation on health-related quality of life and activities of
and sudden cardiac death late after repair of tetralogy of Fallot: a
daily living in patients with recurrent arrhythmias. Circulation 1996;94:
multicentre study. Lancet 2000;356:975– 81.
215. Therrien J, Siu SC, Harris L, et al. Impact of pulmonary valve
228. Lau CP, Tai YT, Lee PW. The effects of radiofrequency ablation versus
replacement on arrhythmia propensity late after repair of tetralogy of
medical therapy on the quality-of-life and exercise capacity in patients
Fallot. Circulation 2001;103:2489 –94.
with accessory pathway-mediated supraventricular tachycardia: a
216. Natterson PD, et al. Electrophysiologic abnormalities: unoperated
treatment comparison study. Pacing Clin Electrophysiol 1995;18:
occurrence and postoperative residua and sequelae. In: Perloff J, ChildJS, eds. Congenital heart disease in adults. Philadelphia, PA: WB
Saunders, 1998:316 –39.
229. Bathina MN, Mickelsen S, Brooks C, et al. Radiofrequency catheter
217. Hebe J. Ebstein's anomaly in adults arrhythmias: diagnosis and thera-
ablation versus medical therapy for initial treatment of supraventricular
peutic approach. Thorac Cardiovasc Surg 2000;48:214 –9.
tachycardia and its impact on quality of life and healthcare costs. Am J
218. Ho SY, Goltz D, McCarthy K, et al. The atrioventricular junctions in
Cardiol 1998;82:589 –93.
Ebstein malformation. Heart 2000;83:444 –9.
230. Cheng CH, Sanders GD, Hlatky MA, et al. Cost-effectiveness of radio-
219. Attie F, Rosas M, Rijlaarsdam M, et al. The adult patient with Ebstein
frequency ablation for supraventricular tachycardia. Ann Intern Med
anomaly: outcome in 72 unoperated patients. Medicine (Baltimore)
2000;133:864 –76.
231. Goldberg AS, Bathina MN, Mickelsen S, et al. Long-term outcomes on
220. Huang CJ, Chiu IS, Lin FY, et al. Role of electrophysiological studies
quality-of-life and health care costs in patients with supraventricular
and arrhythmia intervention in repairing Ebstein's anomaly. Thorac
tachycardia (radiofrequency catheter ablation versus medical therapy).
Cardiovasc Surg 2000;48:347–50.
Am J Cardiol 2002;89:1120 –3.
221. Reich JD, Auld D, Hulse E, et al., for the Pediatric Electrophysiology
232. Anselme F, Saoudi N, Poty H, et al. Radiofrequency catheter ablation of
Society. The Pediatric Radiofrequency Ablation Registry's experience
common atrial flutter: significance of palpitations and quality-of-life
with Ebstein's anomaly. J Cardiovasc Electrophysiol 1998;9:1370 –7.
evaluation in patients with proven isthmus block. Circulation 1999;99:
222. Gatzoulis MA, Munk MD, Williams WG, et al. Definitive palliation
with cavopulmonary or aortopulmonary shunts for adults with single
233. Lee SH, Tai CT, Yu WC, et al. Effects of radiofrequency catheter
ventricle physiology. Heart 2000;83:51–7.
ablation on quality of life in patients with atrial flutter. Am J Cardiol
223. Ghai A, Harris L, Harrison DA, et al. Outcomes of late atrial
1999;84:278 – 83.
tachyarrhythmias in adults after the Fontan operation. J Am Coll Cardiol
234. O'Callaghan PA, Meara M, Kongsgaard E, et al. Symptomatic
improvement after radiofrequency catheter ablation for typical atrial
224. Lesh MD, Van Hare GF, Epstein LM, et al. Radiofrequency catheter
ablation of atrial arrhythmias: results and mechanisms. Circulation 1994;
flutter. Heart 2001;86:167–71.
89:1074 – 89.
225. Triedman JK, Jenkins KJ, Colan SD, et al. Intra-atrial re-entrant
KEY WORDS: ACC/AHA/ESC Practice Guidelines
䡲 arrhythmia 䡲
tachycardia after palliation of congenital heart disease: characterization
tachycardia 䡲 ablation 䡲 drugs
Source: http://arrhythmology.narod.ru/guidelines/Guidelines_Management_SVA.pdf
Acoso Moral o Psicoterror Laboral y sus repercusiones en las personas y la productividad laboral. Resumen: El acoso moral o psicoterror laboral es una de las patologías que más daños producen a las personas trabajadoras así como al rendimiento de las compañías, instituciones y organizaciones, que permiten este tipo de estrategias de abuso
Giasson-Gariépy and Jutras-Aswad Addiction Science & Clinical Practice 2013, 8:22http://www.ascpjournal.org/content/8/1/22 A case of hypomania during nicotine cessationtreatment with bupropion Karine Giasson-Gariépy1,2 and Didier Jutras-Aswad1,2* Antidepressants can increase the spontaneous risk of hypomania or mania when used for treatment in affectivedisorders. When prescribed as an antidepressant, bupropion is generally considered to have a lower relative riskof inducing mood shifts. We describe the case of a 67-year-old man known for dysthymic disorder in remission onquetiapine and venlafaxine who experienced a first lifetime episode of hypomania with the introduction of bupropionSR for smoking cessation. To the best of our knowledge, this is the first case report of bupropion-induced mood shiftwhen used specifically for nicotine cessation in a nonbipolar patient. This case highlights the need for clinicians whoprescribe bupropion for smoking cessation to perform regular and systematic mood follow-ups during treatment.These follow-ups could even be more important when bupropion is selected to quit smoking in a patient alreadytaking an antidepressant.

