Klab.smpp.northwestern.edu
12690 • The Journal of Neuroscience, September 17, 2014 • 34(38):12690 –12700
Serotonin Affects Movement Gain Control in the Spinal Cord
Kunlin Wei,1
Joshua I. Glaser,2,3,4,5
Linna Deng,1
Christopher K. Thompson,5,6
Ian H. Stevenson,2,3,4,5
Qining Wang,1
Thomas George Hornby,2,3,4,5,6
Charles J. Heckman,2,3,4,5
and Konrad P. Kording2,3,4,5
1Department of Psychology, Peking University, Beijing, China 100871, Departments of 2Physical Medicine and Rehabilitation, 3Physiology, and 4Applied
Mathematics, Northwestern University, Chicago, Illinois 60611, 5Rehabilitation Institute of Chicago, Chicago, Illinois 60611, and 6Department of
Kinesiology and Nutrition, University of Illinois at Chicago, Chicago, Illinois 60607
A fundamental challenge for the nervous system is to encode signals spanning many orders of magnitude with neurons of limited
bandwidth. To meet this challenge, perceptual systems use gain control. However, whether the motor system uses an analogous mecha-
nism is essentially unknown. Neuromodulators, such as serotonin, are prime candidates for gain control signals during force production.
Serotonergic neurons project diffusely to motor pools, and, therefore, force production by one muscle should change the gain of others.
Here we present behavioral and pharmaceutical evidence that serotonin modulates the input– output gain of motoneurons in humans. By
selectively changing the efficacy of serotonin with drugs, we systematically modulated the amplitude of spinal reflexes. More importantly,
force production in different limbs interacts systematically, as predicted by a spinal gain control mechanism. Psychophysics and phar-
macology suggest that the motor system adopts gain control mechanisms, and serotonin is a primary driver for their implementation in
force production.
Key words: efficient control; gain control; neuromodulation; pharmacology; serotonin; spinal cord
by motoneurons in the ventral horn of the spinal cord, whose
A central question in neuroscience is how neurons, with limited
axons connect directly to muscle fibers Previous
bandwidth, can encode signals that vary over multiple orders of
physiological studies and modeling work suggested that neuro-
magnitude. Gain control mechanisms, which are present in vir-
modulatory gain control is necessary for force production,
tually all sensory systems, effectively solve this problem
because even the "maximal effort" (maximum current in mo-
toneurons) would scarcely produce 40% of maximal force with-
However, our motor sys-
out neuromodulatory input
tem faces an analogous problem
. A potent neuromodulatory drive to these motoneu-
rons comes from the brainstem via axons projecting mono-
The forces we produce vary from fractions of a Newton, e.g.,
synaptically onto motoneurons and releasing either serotonin
when we put a contact lens into our eye, to nearly 5000 N, the
(5-HT) or norepinephrine (NE;
world record in bench pressing. Because the forces we produce
Both of these neuromodulators facilitate
vary over multiple orders of magnitude but motor commands
voltage-sensitive changes on spinal motoneurons, resulting in
from the brain to spinal cord are transmitted by noisy neurons
greatly increased input– output excitability, i.e., gain
with limited bandwidth, a gain system would reduce noise in
motor output. However, it is not currently known how, and even
5-HT is more likely to be involved in gain control, because
if, the spinal cord uses such a gain control mechanism to main-
5-HT projection to the spinal cord increases its activity with in-
tain accuracy over such a large range of forces.
creasing motor output whereas the NE sys-
If the motor system uses a gain control mechanism, how could
tem covaries with state of arousal This
it do so? All motor output from the trunk and limbs is generated
evidence leads to the hypothesis that 5-HT in the spinal cordplays a significant role in a motor output gain control system
Received May 7, 2014; revised July 6, 2014; accepted Aug. 4, 2014.
Author contributions: K.W., J.I.G., L.D., C.K.T., I.H.S., Q.W., T.G.H., C.J.H., and K.P.K. designed research; K.W.,
Here, we first aim to establish that 5-HT alters gain in the
J.I.G., L.D., C.K.T., I.H.S., Q.W., T.G.H., and C.J.H. performed research; K.W., J.I.G., L.D., C.K.T., I.H.S., T.G.H., C.J.H., and
spinal cord. If this is true, drugs that augment/suppress 5-HT
K.P.K. analyzed data; K.W., J.I.G., L.D., C.K.T., I.H.S., Q.W., T.G.H., C.J.H., and K.P.K. wrote the paper.
should also enhance/inhibit spinal reflex, which is heavily influ-
The study was supported by National Natural Science Foundation of China Grants 31371020, 31328010,
enced by excitability of spinal motoneurons. Second, we aim to
61005082, J1103602, and 61020106005, Beijing Nova Program Grant Z141101001814001, National High Technol-ogy Research and Development Program of China 863 Program Grant 2012AA011602, and National Institutes of
show that this spinal gain mechanism is present during force
Health Grants R01NS063399, P01NS044393, and R01NS034382. We thank Dr. Hongxiao Jia.
production. If this is true, because of the diffuse projection of
The authors declare no competing financial interests.
5-HT into the spinal cord, intense contraction of one muscle
Correspondence should be addressed to Kunlin Wei, Department of Psychology, Peking University, Beijing, China
group (which requires high gain) should degrade the precision at
which a subsequent low-force motor task can be achieved with
Copyright 2014 the authors 0270-6474/14/3412690-11$15.00/0
other muscles. Third, we aim to show that 5-HT affects force






Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
J. Neurosci., September 17, 2014 • 34(38):12690 –12700 • 12691
nary trials for the experimenter to adjust the
vibration head and for subjects to get ac-
quainted with experimental procedures.
Experiment 2 measured the tendon reflex
response as a function of drug intake in the
lower extremity of individuals with reduced
descending drive. Seven subjects with chronic(⬎1 year) spinal cord injury participated in
two sessions separated by at least 5 d: (1) one
session with 20 mg of escitalopram intake; and(2) one with 8 mg of cyproheptadine intake
(administrated double-blinded). The order of
the two sessions was randomized among sub-
jects. In each session, data collection occurred
before drug intake and 5 h after drug intake.
Subjects were seated in the adjustable height
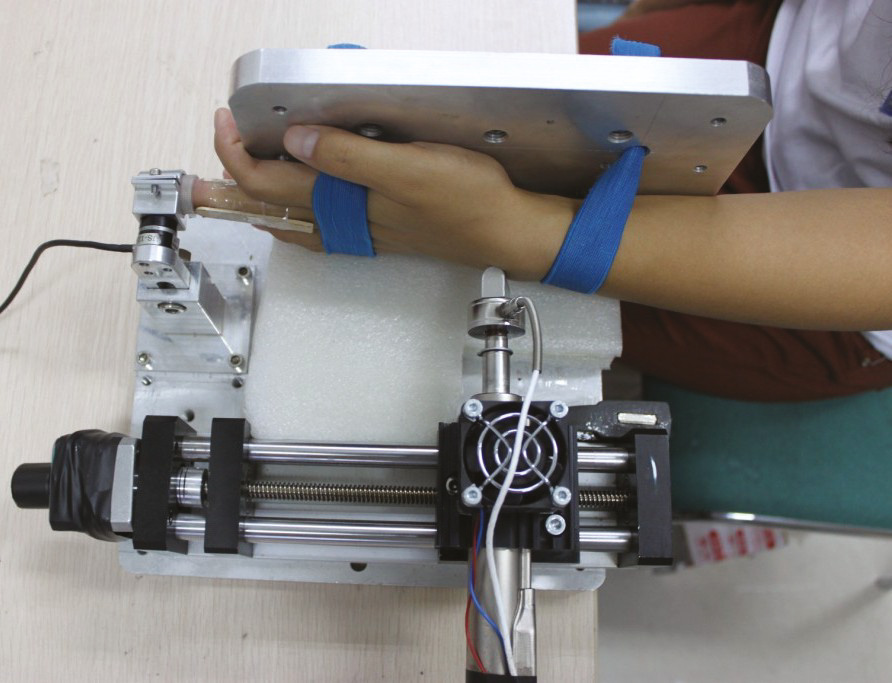
Figure 1.
Experimental setup in Experiment 1 and its data. a, Hardware setup for wrist tendon vibration. The reflexive response
chair of the testing apparatus (System 3; Biodex
is a wrist extension measured by a force transducer fitted on the middle finger. b, Results from Experiment 1. The average reflexive
Medical Systems) with the hips flexed to 45°
forces measured at the middle finger are plotted as a function of time in which time 0 is defined as 2 s before the vibration starts.
and the knee positioned at either 90°. Knee ex-
The data from the escitalopram and the placebo control condition are plotted separately. Error bars denote mean ⫾ SEM across
tension (KE) torques and surface electromyo-
n ⫽ 9 subjects. The force rate during ramp-up and the force level during the last 2 s of vibration were significantly larger in the
graphic (EMG) data were collected on all
escitalopram condition than in the control condition ( p ⬍ 0.01 and 0.05, respectively).
subjects on the more impaired limb as deter-mined during clinical evaluation, with the
production through this spinal gain mechanism. If this is true,
same limb being tested during all sessions. The distal shank of the tested
drugs that augment 5-HT should increase variability in precision
limb was secured to the dynamometer arm, which was coupled to a 6
tasks, whereas those that block its effects should decrease variabil-
degree of freedom load cell (theta; resolution, 0.025 Nm; ATI) used to
ity. Our experiments test these predictions in human subjects.
assess KE torques. Surface EMG was recorded using active bipolar elec-trodes (Delsys) applied over the vastus lateralis (VL), vastus medialis
Materials and Methods
(VM), and rectus femoris (RF). A 2-cm-wide convex rubber head was
Experiment details. Experiment 1 measured tendon vibration reflexes
aligned to the patellar tendon. The head was affixed to a load cell
elicited on the left wrist as a function of drug intake. Subjects (n ⫽ 9)
(resolution, 0.15 N; Omegadyne), which in turn was attached in series
participated in two sessions on 2 consecutive days; (1) one session with
to the end of the neodymium slider of a linear motor (model P01-
escitalopram intake; and (2) one with placebo (administrated double-
23x160H-HP; LinMot). A position control strategy was used to alter
blinded). The order of the two sessions was randomized among subjects,
forces delivered to the tendon; forces were varied by moving the initial
with four subjects taking the drug in the first session and the other five
position of the tapper relative to the tendon using a constant 30 mm
taking the drug in the second session. The data collection started 5 h after
stroke. Reflex threshold was identified as the minimum distance neces-
drug intake when the serum level of escitalopram reached its peak. Sitting
sary to elicit EMG responses of at least one KE muscle. The force applied
before a desk, subjects put the tip of their left middle fingers snugly into
to the tendon was controlled by delivering taps at 11 different positions
a metal ring, which was firmly mounted on the desk top ). Each
ranging from the starting position of reflex threshold (i.e., 0 mm) and
subject's middle finger was also splinted, by two wooden sticks on the
moving progressively closer to the tendon in randomly ordered 1 mm
lateral sides that were bundled by medical tape, to minimize the move-
steps such that responses from 11 different starting positions were as-
ments between phalangeal joints. The metal ring was fixed onto a force
sessed. The minimum rest between tendon reflexes was 20 s, and re-
transducer (resolution, 0.014 N; model Nano 17; ATI) so the reflexive
sponses were elicited two to three times at each position in a blocked
force could be measured. The left arm straightened out and was sup-
ported on the table; the left palm faced rightward and rested against a
Experiments 3–5 and the control experiments used similar paradigms.
metal surface. A 2-cm-wide, concave-shaped metal head pointed to and
Subjects were seated in front of a table. In separate sessions of Experiment
pressed against the left wrist to apply a vibrating stimulus. The head was
3, they either produced a leftward force against a strain gauge (resolution,
screwed on one side of a force transducer (resolution, 0.28 N; model
0.056 N; model Gamma; ATI) fixed on the table top with the right index
Sensotec 31; Honeywell); the other side of the force transducer was
finger or the right palm or lifted the tips of their feet up against a wooden
screwed onto a linear motor (model PS01-23x80; LinMot). The data
fixture placed directly above the feet. When using the finger or the palm
collection was organized as trials. For each trial, the initial position of the
to push against the strain gauge, the subject's right forearm was inserted
vibration head was adjusted so that the contact force between the head
into a customizable polyvinyl chloride tube to prevent arm movement.
and the wrist, measured from the attached force transducer, was above 4
When using two feet, two Nintendo Wii Fit force sensors (resolution,
N. Subjects sat idle with eyes closed after hearing a computer speaker-
0.39 N) were placed above the two feet to measure the upward force. The
generated beep. After a random period of 2– 4 s, the linear motor started
target force levels (low, medium, and high) were set at 5, 35, and 65%,
to apply 100 Hz sinusoidal movements vertically to the wrist with a
respectively, of MVC for each of the three effectors (finger, palm, and leg)
peak-to-peak displacement of 0.6 mm. The vibration lasted 8 s, and the
and were represented as a horizontal line on a computer screen placed in
data collection continued for another 10 s, until a beep signaled the end
front of the subject. The power forces produced by these effectors were
of the trial. Subjects were instructed to remain relaxed through each trial.
measured and displayed in real time as a moving cursor on the screen.
The contact force between the vibration head and the wrist was con-
The vertical displacement of the cursor was controlled by the force mag-
stantly monitored throughout the experiment; if it dropped below 4 N,
nitude, and the horizontal displacement was driven by elapsed time. Each
the experimenter would adjust the initial position of the head manually
trial was randomly assigned a target force level, and the subject was
before the next trial started. This ensured that all trials had the same
required to ramp up the power force in the first second and to maintain
initial contact force. The tendon vibration elicited a wrist extension,
it precisely at the target level. At 3 s, a monophonic beep signaled the
which in turn generated a pushing force onto the force transducer at-
subject to press the left index finger downward on a strain gauge (reso-
tached to the finger ring. We also measured the maximum voluntary
lution, 0.0035 N; model Nano 17; ATI). This precision force needed to
contraction (MVC) of this finger extension before the vibration trials
reach its target level (5% MVC, constant across all sessions) in 1 s and be
started. A total of 32 vibration trials were collected: eight trials per block
maintained there until the 14th second when the trial end. The target
with an interblock rest period of 3 min. The first 12 trials were prelimi-
level was marked as a red horizontal line on the computer screen. At 5.8 s,
12692 • J. Neurosci., September 17, 2014 • 34(38):12690 –12700
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
a stereophonic tone signaled subjects to stop producing the power force.
from a nonpublic registry housed within the Rehabilitation Institute of
As the power force ceased at approximately the 6th second, the two forces
Chicago. They were seven males with chronic (⬎1 year) spinal lesions
were simultaneously applied for ⬃2 s. The subjects were instructed to
above the T10 neurological level. Injuries were incomplete, and all sub-
disengage the power force by gently releasing the right index finger, the
jects demonstrated residual volitional KE strength in the tested limb as
right palm, or two feet from the force sensors, minimizing its impact on
determined by the lower extremity motor score
the precision force production. To minimize mechanical coupling be-
Exclusion criteria included medical history of multiple CNS le-
tween the two forces, the power force was applied in the lateral (finger
sions, known reaction to study medications, and diagnosis of lower limb
and palm) or upward (leg) direction, whereas the precision force was
peripheral nerve injury or orthopedic injury that may limit maximal
always applied downward. A monetary reward, in reverse proportion to
effort during KE contractions.
the variance of the precision force, was shown on the top-left corner of
All procedures of Experiment 1 and Experiments 3–5 and control
the computer screen after each trial to encourage good performance.
experiments were approved by the ethics committee of Peking Univer-
Experiment 3 consisted of three separate sessions, one for each effector
sity. All procedures of Experiments 2 and 3 were approved by the Insti-
used to produce the power force. The sequence of sessions was random-
tutional Review Board of Northwestern University. All experiments were
ized among seven subjects. For each session, we first calibrated the force
performed in accordance with the Declaration of Helsinki.
sensors by asking subjects to place their left index finger on the strain
Data analysis. For Experiment 1, the force elicited by the tendon vi-
gauge and their feet below the foot fixture. The forces collected were
bration reflex was measured at 1000 Hz. It was low-pass filtered at 5 Hz by
averaged for zeroing the readings of the sensors. Then, MVCs of effectors
a fifth-order Butterworth filter to remove the measurement noise and the
for the power force and for the precision force were collected twice with
vibration force transmitted from the wrist to the finger. The force data
a mandatory 90 s rest between. The larger force among the two readings
were then normalized by dividing by individuals' MVCs. To derive the
was taken as the MVC for the session. Before formal data collection,
average force curve, all trials were aligned at 2 s before the vibration (time
subjects practiced the task on the apparatus for six trials. Trials in one
0). We were particularly interested in the speed of force development
session were further partitioned into four blocks of 12 trials each with a
immediately after the initiation of the vibration. This force rate was
90 s rest between sessions. The resting time between trials was 10 s. MVCs
quantified by fitting a linear slope to the force data between the second
were measured again in the middle (immediately after the second ses-
and fourth seconds. We also calculated the average force level achieved
sion) and after the experiment (immediately after the fourth session).
during the last 2 s of the vibration. Thirteen trials (3.6% of total trials)
Experiments 4 and 5 only used the right palm as the effector for the
were excluded from analyses because visual inspection revealed that sub-
power force. Both experiments had different sets of eight subjects, and
jects occasionally failed to follow the instruction, e.g., moving their fin-
they were measured in two sessions on 2 successive days: (1) one with
gers before the vibration.
drug intake; and (2) the other with placebo intake (administered double-
For Experiment 2, the force delivered to the tendon and resulting
blind). The two sessions were performed at the same time during the day
torque and EMG responses were collected at 1000 Hz. The force signal
for each subject. To minimize the learning effect, the order of the two
was filtered at 220 Hz, the torque signal was low-pass filtered at 200 Hz,
sessions was randomized among subjects, with four subjects taking the
and the EMG signals were bandpass filtered at 20 – 450 Hz before digiti-
drug on the first day and the other four taking it on the second day. In
zation. The peak tap force for each tap was found offline and defined as
Experiment 4, data collection started 2 h after oral intake of cyprohepta-
tap onset. The peak-to-peak amplitude of the tendon reflex was calcu-
dine or the placebo, because serum level of cyproheptadine usually
lated for each muscle. To assess the gain of the reflex response, the reflex
reaches its peak level in 2 h. For the same reason, data collection for
amplitudes at the 11 different tap conditions were plotted against tap
Experiment 5 was started 5 h after paroxetine intake. Both experi-
force to construct a reflex response curve for each muscle. The gain of the
ments used the same protocol as Experiment 3 with minor changes:
tendon reflex was calculated as the linear slope of this reflex response
subjects practiced for 30 trials before formal data collection to mini-
curves for each muscle. One subject was excluded from the analysis in the
mize the learning effect, and the number of trials within each block
cyproheptadine group because tendon reflexes were unable to be elicited
increased to 15.
both before and after medication. To facilitate cross-muscle comparison,
Control Experiments A and B had the identical protocol as Experi-
we calculated the percentage change in both the amplitude and gain
ment 3 with some modifications. Only the palm was used to produce the
measurements for each muscle. They were calculated as the difference
power force. Control Experiment A reversed the order of the precision
between the post-medication and pre-medication values divided by pre-
force and the power force: the precision force reached its target level in
medication values and expressed as a percentage. We tested whether the
the first second and maintained there until the trial end at the 16th
percentage change across muscles in reflex amplitude and gain are dif-
second. The power force was ramped up between the second and the
ferent from 0, after either escitalopram or cyproheptadine administra-
third seconds and then dropped at the eighth second. The duration of the
tion. Given the sample size and a lack of data normality, Wilcoxon's
power force thus remained 5 s to facilitate comparisons between experi-
signed-rank tests were used.
ments. Compared with Experiment 3, Control Experiment B switched
For Experiments 3–5 and Control Experiments A and B, the precision
the roles of two hands: the dominant hand produced the precision force,
force was sampled at 200 Hz and the power force at 75 Hz. The precision
and the nondominant hand produced the power force. Eight subjects
force was bandpass filtered between 2 and 30 Hz with a fifth-order But-
participated in Control Experiment A, and a different set of seven sub-
terworth filter to remove slow transients and high-frequency, nonphysi-
jects participated in Control Experiment B. The same seven subjects then
ological measurement noise. The resulting data were aligned to the time
performed Control Experiment C in which only the precision force was
when the power force dropped to 50% of its target value. The SD was
produced with the right finger for 18 trials.
calculated over each second before and after this time. SDs obtained were
In Experiment 1, MVCs for the left middle finger extension were
then normalized by dividing by the target force magnitude
7.65 ⫾ 0.54 and 7.40 ⫾ 0.65 N with escitalopram intake and without,
Thus, force variance is essentially
respectively. In Experiment 3, MVCs were 3.98 ⫾ 1.23 (mean ⫾ SD),
quantified by the coefficient of variation (CV). This measure takes indi-
10.86 ⫾ 3.30, 23.35 ⫾ 6.87, and 48.66 ⫾ 13.63 N for the left finger, right
vidual differences in the target force into account and facilitates the com-
finger, right palm, and the average of both legs, respectively. In Experi-
parison across participants. The mean over trials of each condition was
ment 4, MVCs for the left finger were 4.50 ⫾ 0.88 and 4.61 ⫾ 0.67 N with
reported. The criteria for eliminating trials included the following: (1)
cyproheptadine intake and without, respectively. MVCs for the right
failure to start the precision force or to stop the power force within a 2 s
palm were 31.19 ⫾ 5.50 and 31.37 ⫾ 6.89 N, respectively. In Experiment
window of the required time; (2) failure to stabilize the precision force
5, MVCs for the left finger were 4.78 ⫾ 0.63 and 5.06 ⫾ 0.29 N with
during the 1 s before the power force stopped; and (3) failure to keep the
paroxetine intake and without, respectively. MVCs for the right palm
precision force within 4 SDs of the target force during the stationary part
were 41.12 ⫾ 6.73 and 40.71 ⫾ 5.95 N, respectively. All subjects partici-
of the trial after the power force ceased. In total, 6.7, 4.0, and 3.5% of all
pated in experiments after providing informed consent. Subjects with
trials were eliminated for additional analysis in the three experiments,
motor incomplete spinal cord injury in Experiment 2 were recruited
respectively. The number of eliminated trials did not differ between three
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
J. Neurosci., September 17, 2014 • 34(38):12690 –12700 • 12693
force conditions (one-way ANOVA with p ⫽ 0.94, 0.50, and 0.76, respec-
59.6% (35.3–73.1) and decreased the gain of the tendon reflex by
tively). Data were examined for normality before being submitted to
70.1% (51.5– 80.3; p ⫽ 0.0002 and p ⫽ 0.0005, respectively; n ⫽
parametrical statistical analyses. The comparisons between force condi-
6). These data support modification of the gain of tendon tap
tions (and between effectors) were conducted by one-sided paired t tests.
reflex by the serotonergic system.
The comparisons between drug and force conditions were conducted bytwo-way (2 drug conditions ⫻ 3 force levels) repeated-measures ANOVAs.
Why would a gain control mechanism be useful?
The comparisons between force conditions in terms of variance changesinduced by drugs were conducted by one-sided paired t tests.
Would the use of two distinct transmission channels (descendingdrives and gain) allow for more efficient transmission? We want
to highlight the advantage of gain control with a simple example.
Evidence from spinal reflexes
Let us say we have a transmission system (e.g., motoneurons to
To establish that 5-HT serves as a gain control signal on the spinal
muscles) that can only transmit a maximal number of spikes
motoneuron in humans, we examined the reflex response of ten-
during a relevant interval and that we can only produce forces
don vibration among healthy subjects under the influence of esci-
that are proportional to the number of spikes. Let us say that our
talopram (Experiment 1; ). Previous studies in animal
system can produce a maximum of 10 spikes, and there is one
preparations have established that 5-HT strongly potentiates spi-
situation (A) in which we need forces between 0 and 1 N and
another situation (B) in which we need forces between 0 and 10 N
Escitalopram is a selective 5-HT reuptake inhibitor that can am-
). In this example, if we have a system with a fixed gain,
plify the levels of 5-HT. The tendon vibration primarily activates
then we must use a gain of 1 N/spike because a lower gain would
muscle spindle Ia afferents that monosynaptically project to spi-
not support the maximal forces needed in Situation B. However,
nal motoneurons and is thus a spinally mediated response
this means that, in Situation A, we will only be able to produce
Thus, it allows us to experimentally ask how 5-HT
integer-valued forces, resulting in errors up to 0.5 N. Without a
affects spinal excitability.
gain factor, the need to be able to produce high forces necessitates
To establish the methods we are using, we find that subjects
high errors for small forces.
produced similar MVCs with and without the drug ( p ⫽ 0.57,
If we can instead use a context-dependent gain, then we could
paired t test). With tendon vibration, subjects immediately devel-
use a gain of 0.1 N/spike in Situation A and 1 N/spike in Situation
oped an extension force until reaching its plateau ). The
B. In this case, we will make maximal errors in Situation A of 0.05
force dropped gradually after the vibration was turned off. All
N, leading to a significant reduction in noise while leaving the
subjects reported after the experiment that their hand appeared
errors in Situation B unaffected. Thus, in a limited bandwidth
to be moved passively, indicating that the tendon vibration reflex
transmission system such as the brain, a gain system can result in
had been successfully elicited
more efficient transmission.
We found that the rate of force development, driven by con-
stant tendon vibration stimuli, was significantly higher with esci-
Model of force production with gain control
talopram intake than without ( p ⬍ 0.01, paired t test). The
To be able to experimentally test the results of gain control, we
average force rates were 1.35 ⫾ 0.39 and 2.2 ⫾ 0.45% of MVC per
need to specify a model of how gain control affects force output.
second for the placebo and escitalopram conditions, respectively.
With a gain control mechanism, muscular force is jointly deter-
The achieved force was also significantly higher as evaluated during
mined by descending neural commands and gain signals. In a
the last 2 s of vibration (p ⬍ 0.05, paired t test). The average forces
simple model, a desired force F is the result of the descending
were 4.4 ⫾ 0.76 and 6.8 ⫾ 1.1% of MVC for the placebo and escita-
drive multiplied by a spinal output gain: F ⫽ gain ⫻ drive. The
lopram conditions, respectively. Hence, the enhanced efficacy of
drive needed to produce a given force thus depends on the output
5-HT leads to larger responses of tendon vibration reflex and thus
gain: a high descending drive at low gain can yield the same
supports 5-HT altering the gain of spinal motoneurons.
average force as a low descending drive at high gain ).
To further establish the role of 5-HT and also show that de-
However, these situations may differ in terms of their variability.
scending drive is unlikely to contribute to these findings, we ex-
Uncontrolled variability (noise) in force production is not solely
amined magnitude and gain of tendon tap reflex responses in
defined by the descending drive but can be influenced by gain
individuals with reduced descending drive attributable to partial
control at the motor output stage in the spinal cord.
spinal injury (Experiment 2). The tap evokes a brief activation of
Assuming that the pool of neurons transmitting the drive has
the same muscle spindle Ia afferents stimulated by tendon vibra-
Poisson-like behavior, as is typical for neurons in both sensory
tion Whereas the long duration of the tendon
and motor systems the variance in the
vibration reflex could potentially evoke non-spinal pathways, the
drive is proportional to the mean drive: 2
tendon reflex elicited by brief taps is unequivocally spinal, mediated
characterizes the Poisson-like behavior (the Fano factor;
by monosynaptic EPSPs in motoneurons We sys-
For a fixed gain, the SD in the force output relative to
tematically varied the amplitude of the tap, allowing direct measure-
the target force F will depend on the gain:
ment of reflex gain across a wide input– output range
Acute administration of serotonergic agents did indeed modify
gain 冑␣ ⫽ drive.
both the amplitude and gain of the patellar tendon reflex responseacross the quadriceps muscles After administration of esci-
In our model, we find that the lower the gain, the lower the noise.
talopram, the amplitude of the tendon reflex is increased by a me-
Thus, we can quantify gain control during force production by ex-
dian of 36.3% (range: 18.0 –129.4) across all muscles; likewise, the
amining variability because force variability depends on the gain.
gain of the tendon reflex is increased by 196.1% (45.3– 656.0), withboth metrics being significantly greater than 0 (p ⬍ 0.0001 and p ⫽
Behavioral evidence from across-effector tasks
0.0001, respectively; n ⫽ 7). The opposite effects were observed in
Our behavioral experiments were designed based on evidence of
response to a 5-HT antagonist. Here, acute administration of
a diffuse serotonergic system. Studies in animal preparations
cyproheptadine decreased the amplitude of the tendon reflex by
have established that the brainstem–spinal neuromodulatory sys-
12694 • J. Neurosci., September 17, 2014 • 34(38):12690 –12700
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
Post Escitalopram
Pre Cyproheptadine
Post Cyproheptadine
Figure 2.
Results of Experiment 2 with individuals with chronic spinal cord injury (SCI). a, Tap forces and elicited EMG responses for quadriceps tendon reflexes in a typical subject with and without
escitalopram intake. Muscles include VL, VM, and RF. b, Similar exemplary trials in the same subject as in a with administration of cyproheptadine. c, The peak-to-peak amplitude of the reflex
response for RF is plotted against tap force, and the reflex gain is calculated as the slope of the linear regression of the linear portion of the reflex curve (filled circles). Data are from the same typical
subject before and after escitalopram intake. d, Similar plot as in c from the same subject before and after cyproheptadine intake. e, Across all subjects, escitalopram intake produces an increase in
amplitude of the tendon reflex, producing a median 56% increase in the RF, 20% increase in the VL, and 36% increase in the VM, whereas after cyproheptadine intake, the amplitude of the tendon
reflex is decreased by 61, 48, and 59% in the RF, VL, and VM, respectively. f, The gain of the reflex was likewise modified by serotonergic agents. After escitalopram intake, the gain of the response
was increased by 196, 283, and 116%, and after cyproheptadine intake, the gain of the response was decreased by 75, 70, and 65% in the RF, VL, and VM, respectively.
tem is highly diffuse in its projection from the brainstem to the
expect force production in one effector to alter the gain of the corti-
cospinal pathway and thus alter force production in a separate effec-
Similarly, studies in humans have sug-
tor. Furthermore, this gain effect should last for a short period of
gested that the excitability of the corticospinal pathway can be
time after the original effector stops its force production.
enhanced with large concurrent force production in a separate
In Experiments 3–5, we used a psychophysical task requiring
effector This suggests that gain control
two successive isometric muscular contractions using separate
mechanisms and neuromodulatory signals in particular affect the
effectors; we call the first the power force and the second the
overall excitability of motor output throughout a limb or even
precision force. In Experiment 3, the power force is produced in
across the whole body. Furthermore, gain control also changes
three separate conditions by the right index finger, the right palm,
relatively slowly and affects many neurons at the same time
or the two feet, and the intensity of the force is varied ). In
it is diffuse in space and time.
Experiments 4 and 5, the power force is produced by the right
Therefore, if there is a spinal gain control mechanism, we would
palm only, but subjects are required to take the drugs that selec-
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
J. Neurosci., September 17, 2014 • 34(38):12690 –12700 • 12695
level. This is, in general, not the case
). We calculated the cross-correlation
between two forces when they are simul-
taneously on, 0.5 s before the completion
of the power force. It is indistinguishable
among three force levels, suggesting that
the dependency of variance on power
force levels is unlikely to be caused by me-
chanical coupling.
We performed three control experi-
ments to rule out other possible con-
Muscle force (normalized)
Synaptic input (nA of current)
founding factors. The involved transients
may affect the cognitive burden. In Con-trol Experiment A, we thus reversed the
Figure 3.
Model of gain control. a, A hypothetical scenario with context-dependent gain control. To encode both 10 and 1 N
order of two forces, and the systematic ef-
target forces with only 10 spikes (B), the best resolution for the 1 N force is 0.5 N, with a gain of 1 N/spike, which is the lowest gainthat make the 10 N force production possible. Allowing a context-dependent gain of 0.1 N/spike (A), the resolution can be 0.05 N
fects of the power force onto the precision
for the 1 N force while leaving the solution for the 10 N force unaffected. b, Muscle force plotted as a function of synaptic input and
force are essentially unchanged , at
gain according to our model. Depending on the gain, a fixed variance in synaptic inputs translates to different levels of variance in
approximately time 0 and onward). The
muscle force (variances shown as Gaussian distributions).
critical comparison is for the time afterthe power force is dropped. In addition,
tively suppress or enhance the efficacy of 5-HT (see Materials and
we observed that the variance of the precision force does not
Methods). This allows determining the serotonergic influence on
differ when subjects are expecting different levels of power forces
gain control.
(at ⫺7 s). This suggests there is no priming effect from upcoming
For each trial, subjects ramp up the power force and stabilize it
power forces.
for a fixed duration and subsequently produce a precision force
Second, the precision force is always performed by the left,
with the left index finger ). The power force is then
nondominant hand, and thus handedness might affect the vari-
switched off while the precision force remains until the end of the
ance results. In Control Experiment B, the hands of the two forces
trial. How the previous power force modulates the variance of
are switched so that the dominant hand performed the precision
the precision force is the focus of our analyses. We expected that
force and the nondominant hand performed the power force.
the effects of the intense activation of the descending serotonergic
The noise level in the precision force still follows a similar pattern
system would gradually decline after the end of the power force
as in Experiment 3 ).
for two reasons: (1) the activity of the descending system itself
Third, primary results are about variance changes in the pre-
would likely decline relatively slowly; and (2) there is a slow decay
cision force after the power force exits; what is the natural fluc-
of the persistent inward current in motoneurons
tuation in variance with the precision force only? In Control
We focus on the precision
Experiment C, the same set of subjects from Control Experiment
force variation after the power force is released rather than when
B was tested to produce the precision force only. The resulting
the two forces are held concurrently to minimize the effect of
noise level is indistinguishable from that in the low force condi-
divided attention. With these experiments, we can analyze how
tion in the dual-force paradigm ), suggesting that natural
gain changes in the spinal cord induced by the power force
fluctuations in the precision force cannot account for the en-
affect the production of a precision force (recall from the
hanced noise level associated with power forces. The similarity
above equation that a larger gain will lead to a larger variation
between the dual-force task (Control Experiment B) and the
in force production).
single-force task (Control Experiment C) also suggests that our
We find that power forces affect noise levels in the concurrent
findings are not a result of divided attention.
precision task (Experiment 3; –e). More importantly, asexpected by our gain control hypothesis, this effect is significant
Pharmacological evidence from across-effector tasks
after the drop of power forces, and it decays toward baseline
To establish a role for 5-HT in the observed cross-limb interac-
within ⬃2 s. The intensity of the power force has a strong effect
tions, we directly and selectively manipulated 5-HT activity with
on noise levels.
drugs and examined performance in the same dual force produc-
This intensity effect is observed no matter which effector is
tion task as in Experiment 3. After oral intake of cyproheptadine
used for power force production: the contralateral finger, hand,
(Experiment 4), a selective 5-HT receptor antagonist, the excit-
or the legs. The palm appears to produce the strongest effect.
atory effect of 5-HT is reduced
When comparing the CV during the first second for different
and the precision
effectors in the high force condition, we found a significant dif-
force is expected to exhibit less variance ). This variance
ference between the finger and the palm ( p ⬍ 0.05). This might
reduction should also be more pronounced when the magnitude
be expected if assuming an approximate somatotopy in the ra-
of the power force, and thus 5-HT levels, increase ).
phe–spinal projections in which the arm muscles (primarily in-
We found that subjects show improved precision after cypro-
volved for the palm as the effector) has more projections. Thus,
heptadine intake and thus performed better after the drop; the
we use the palm to elicit gain changes for all our subsequent
opposite would be expected from potential side effects, such as
analyses and additional experiments (Experiments 4 and 5).
drowsiness, of the drug. In agreement with our hypothesis, there
If mechanical coupling was underlying the differential effect
was a greater improvement after larger power forces. After oral
of the power force on the precision force variance, we would
intake of paroxetine (Experiment 5), which is a selective 5-HT
expect that the cross-correlation between two forces should be
reuptake inhibitor capable of enhancing the excitatory effect of
significantly different from zero and scaled by the power force
5-HT, the opposite effect is observed ,d): the variance in
12696 • J. Neurosci., September 17, 2014 • 34(38):12690 –12700
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
Experiment 1: palm
d Experiment 1: finger
Precision force (N)
e Experiment 1: leg
g Control Experiment 1
h Control Experiment 2 & 3
ficient of V .010
-6.5 -5.5 -4.5 -3.5 -2.5 -1.5 -0.5 0.5 1.5
Figure 4.
Results from Experiment 3 and Control Experiments A-C. a, Experimental setup for Experiments 3–5 and the control experiments. The lines on the screen represent the force instructions
for the precision force (red) and the power force (blue). b, Force signals from a typical subject during the medium power force task. Subjects were instructed to produce a precision force with their
left index finger (mean shown in blue) while first holding and afterward removing the power force. The green trace depicts a typical power force recording, dropping to half of its amplitude at time
0. Gray shading denotes SDs across trials. c– e, Variance (CV) of the precision force during each second before and after switching off the power force produced by the palm (c), the finger (d), and the
leg (e). The moment when the power force drops to its half amplitude is defined as time 0. On the time axis, 0.5 s means that the variance is calculated over the first second after time 0 (between 0
and 1 s). Significant differences have been found between power force intensity levels within the ⫺1, 1, and 2 s (not marked in graph) for all effectors. f, Cross-correlation of the power force and the
precision force is plotted as a function of time lag for three force levels separately. g, Results from Control Experiment A, presented in the same format as in c. The dashed lines represent the force
instructions for the precision force (red) and the power force (blue), which are now in the reverse order as a. Significant differences have been found between power force intensity levels within the
⫺1, 1, and 2 s (not marked in graph). There is no difference found within ⫺7 s. h, Results from Control Experiments B and C, presented in the same format as in c. Significant differences have been
found between power force intensity levels within the ⫺1, 1, and 2 s (not marked in graph). *p ⬍ 0.05, **p ⬍ 0.01, ***p ⬍ 0.001.
precision force production increases in all conditions, and this
out a contribution to gain control from the cortex or other
increase is significantly larger with larger power force.
components of the movement system but do provide strong
We also found that, throughout the entire period, subjects had
evidence that spinal motoneurons are strongly involved. We have
lower variance on cyproheptadine and higher variance on parox-
also shown that this gain mechanism is present during force pro-
etine. Two-way repeated-measures ANOVAs (2 drug condi-
duction and can manifest itself as across-effector interactions
tions ⫻ 3 force levels), conducted for each experiment separately,
reveal significant main effects of the drugs at different times dur-
Gain control can refer to any phenomenon in which the in-
ing a trial (separate tests for the ⫺1, 1, 2, and 6 s; seven of eight
put– output relationship gets modulated, and hence there are
tests are significant with p ⬍ 0.05 or p ⬍ 0.005, and the last test
diverse uses of the concept in movement science. In many closed-
comes out marginally significant with p ⫽ 0.071). These results
loop situations (e.g., reflexes or perception–action loop), gain is
indicate that the reduction and increase in variance induced by
used to refer to the effect of feedback on future movement or
drugs are significant during the whole trial, before and after the
power force is dropped. Therefore, 5-HT also seems to have a
reliable baseline influence on resulting variance.
sense, any increasing force can be viewed as a result of changing
To rule out the possibility of central or peripheral fatigue, we
gain of the muscle as increasingly more motor units get recruited
compared the maximum voluntary force before, in the middle of,
and after data collection in these dual-task experiments. In Ex-
the present study, the gain of force control refers to the slope of
periment 3, MVCs of all effectors do not change significantly
input– output function between synaptic inputs (descending
(one-way ANOVA on timing, p ⫽ 0.588, 0.919, 0.723, and 0.868
drives and afferent signals) and the resulting motor output (force
for the right finger, palm, leg, and left finger, respectively). For the
or EMG; ). This is a definition similar to what has been
two drug experiments (Experiments 4 and 5), we performed a 2
used widely in the perceptual literature
(drug) ⫻ 3 (timing) repeated-measures ANOVA on MVCs of the
gain is one of two channels rele-
finger and the palm. Neither the main effects nor the interactionis significant, indicating that fatigue does not contribute to the
vant to information transmission.
observed effects and that MVCs are not affected by cyprohepta-
Note that we here specifically refer to the gain control in the
dine or paroxetine intake.
spinal cord. In cortical neurons, synaptic noise can markedlydecrease gain in response to input Spinal
motoneurons work in a different synaptic processing regimen,
Here, we have proposed that gain control in the spinal cord is
having long spike afterhyperpolarizations and relatively regular
computationally desirable for producing a wide range of mus-
spiking outputs (CVs of firing in motoneurons in humans during
cular forces and established behavioral and pharmacological
voluntary contractions rarely exceed 0.2;
paradigms to examine its effects and causes. Using reflex as-
Instead, gain control occurs via neuromodulatory inputs,
sessments, we provided strong evidence that the gain effect of
such as 5-HT, that increase persistent inward currents to amplify
5-HT is based on spinal mechanisms. These results do not rule
incoming synaptic current.
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
J. Neurosci., September 17, 2014 • 34(38):12690 –12700 • 12697
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
Increase in CV .002
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
-1.5 -0.5 0.5 1.5 2.5 3.5 4.5 5.5
Figure 5.
Results from Experiments 4 and 5. a, Variance in the precision force plotted as a function of time, with or without cyproheptadine intake. The data from different power force conditions
are plotted separately. b, Variance reduction (within the 1st second) induced by cyproheptadine intake is plotted as a function of the power force. c, Variance in the precision force as a function of
time, with or without paroxetine intake. d, Variance increase (within the 1st second) induced by paroxetine intake is plotted as a function of the power force. Error bars denote mean ⫾ SEM across
n ⫽ 8 subjects. *p ⬍ 0.05.
Previous studies provide significant neurophysiological evi-
in gain is negligible and it is ignored in our simple model (see
dence supporting a role for 5-HT in the excitability of motor
equation in Results).
Although the neuromodulatory gain control is advantageous
havior of the brainstem–spinal neuromodulatory system is state
in terms of offering precise control over a large range with limited
dependent: quiescent in the sleeping state and tonically active in
bandwidth, the obvious disadvantage for this strategy is the un-
the waking state In addition, it appears likely
necessary coupling between effectors. This unspecific control can
that the 5-HT projection to the cord increases its activity with
be negated by reciprocal inhibition mediated by spindle Ia affer-
increasing motor output
ents and Ia interneurons
Thus, the brainstem–spinal cord neuromodulatory system
Dendritic persistent inward current, which is the main
could adaptively match the gain of motoneurons to the demands
mechanism of serotonergic control of motoneuron gain, is highly
of both precise and intense motor behaviors. This kind of gain
sensitive to this inhibition
control is particularly useful in cases in which communication
Thus, the nervous system can still offer specific control
channels are narrow. The descending pyramidal tract, for in-
with a diffusive neuromodulation background if the descending
stance, contains ⬍106 axons which is relatively
motor commands are coupled to both brainstem monoaminer-
narrow given that there are both a large number of cortical motor
gic nuclei and to reciprocal inhibitory interneurons in the spinal
neurons and a large number of involved muscles and fibers.
Adaptive gain control can support generating large motor output
Our findings from spinal reflexes provided direct support for
without sacrificing precision for small motor output.
a spinal locus for the 5-HT effect. In Experiment 1, we demon-
It might be asked whether the introduction of a gain would
strated that the response of the tendon vibration reflex can be
also introduce noise, which might undo the advantage of using
amplified by selectively manipulating 5-HT efficacy. We consider
gain control. However, if the gain changes slowly, then the trans-
a descending contribution unlikely to account for the gain effect
mission of the gain can have a large time constant. Because SEs of
we observed in Experiment 1 for two reasons. First, the subject
firing rate estimates scale linearly with the inverse square root of
was instructed to relax during the whole duration of a trial. The
integration time, long integration time constants translate into
vibration was applied at a random time in each trial to minimize
small variance for slowly changing gains. Thus, the effect of noise
anticipation. These measures prevented voluntary intervention
12698 • J. Neurosci., September 17, 2014 • 34(38):12690 –12700
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
of reflexive responses. In fact, the difference in reflexive response
ing the MVC, muscle fibers are maximally recruited, and thus the
between 5-HT drug conditions is evidenced immediately after
force output will not increase further even when the 5-HT effi-
application of vibration ), suggesting that the gain effect is
cacy is amplified. Conversely, the MVC is still unaffected when
not mediated by feedback.
the 5-HT efficacy is reduced by a selective 5-HT reuptake inhib-
Second, previous studies on tendon vibration reflex in ani-
itor. We postulate in this case that other neuromodulators help in
mals and humans established that this type of reflex is essentially
amplifying the gain when large force production is demanded, as
monosynaptic. In animal preparations, the tendon vibration re-
revealed by single-cell studies
flex is well established as being attributable to the monosynaptic
Thus, this result is consistent with the notion that other
connections of Ia afferents onto motoneurons
neuromodulators might also play a role in gain control. For in-
In humans, vibration must be applied via the skin and thus acti-
stance, animal studies typically found that both 5-HT and NE
vates additional afferents but the
have an amplification effect. Here we focus on 5-HT because NE
overall form of the reflex is identical to that in the animal. The
is closely related to arousal, making 5-HT a more likely candidate
tendon vibration reflexes studied here behaved just as in animal
for generic neuromodulatory gain control. Moreover, the 5-HT
preparations, including the tendency for a slow increase and then
projection to the spinal cord increases its activity with increasing
decrease that is a hallmark of the short-term plastic behavior
motor output Finally, 5-HT alone can pro-
exhibited by the voltage-sensitive Ca channels that generate per-
duce an equally strong amplification effect as both 5-HT and NE
sistent inward currents
combined, as shown in an animal preparation study
However, an unconscious contribution in human subjects,
although unlikely, is still possible. This possibility was one reason
There are many previously described changes in excitability of
that prompted us to conduct Experiment 2 with tendon tap re-
the human motor system. An intensive volitional contraction will
flex, which is much too brief to be affected by changes in descend-
result in reflex potentiation in both the contracting
ing drives. We applied tendon taps to the knee instead of the wrist
because of the complexity of the wrist tendon structure. Experi-
ment 2 further demonstrates the spinal loci of gain control of
muscles, as well as an enhancement
motor output; both the magnitude and the gain of the short-
of corticospinal tract excitability
latency (⬍50 ms) tendon reflex is either amplified or suppressed
with differing 5-HT medications in individuals with reduced cor-
The proposed mechanisms underlying this remote altera-
tical drive.
tion in the excitability of the motor system range from decreased
Although the effect of 5-HT that we discovered in Experi-
presynaptic inhibition of Ia terminals to widespread increases in
ments 3–5 could in principle also be outside of the spinal cord,
previous physiological work
We cannot completely exclude potential contributions from
these mechanisms; however, the systematic patterns elicited by
makes it very likely that the action is in the spinal
pharmacologically manipulating the efficacy of 5-HT on both
cord. For example, our administration of drugs might affect the
volitional and reflexive pathways provide firm support for both
cortical control of force. However, for a single dose, their effects
the neuromodulatory and spinal origins of our findings. More-
are most potent on the spinal cord, because previous studies re-
over, our current findings are fully consistent with these previous
vealed that a moderate to high dose of 5-HT in an animal prepa-
investigations, and the widespread actions of 5-HT on the gain
ration can increase motoneuron throughput gain by as much as
control of spinal neurons may be an unaccounted for mechanism
that would aid in unifying these previous interpretations. It is
dition, motoneurons are densely covered in synaptic boutons
now clear that future studies on remote effects should take neu-
containing 5-HT, which provide direct, monosynaptic connec-
romodulatory gain control in the spinal cord into consideration.
tions from the brainstem
Targeting the serotonergic system has been shown recently to
In fact, the number of 5-HT synapses is larger than the
be a promising strategy to improve function and reduce spasticity
number of synapses from muscle spindle Ia afferents mediating
after spinal cord injury
the tendon tap and vibration reflexes
In terms of behavior, it is important to realize that, when
Hence, although we cannot exclude cortical effect for cross-limb
multiple effectors are involved in movement, their noise levels are
interaction, previous findings and our results on spinal reflexes
not independent from one another, because gain control makes
support the role of 5-HT on the spinal level.
them dependent. Gain control in the spinal cord promises to be
A possible cortical mechanism is that the variance increase in
important topic for research in rehabilitation and motor control.
our psychophysical experiments results from divided attentionsuch that a higher power force is associated with a greater atten-
tional effect. However, there are two results arguing against this
Alvarez FJ, Pearson JC, Harrington D, Dewey D, Torbeck L, Fyffe RE (1998)
interpretation. First, we observe differing variance with pharma-
Distribution of 5-hydroxytryptamine-immunoreactive boutons onalpha-motoneurons in the lumbar spinal cord of adult cats. J Comp Neu-
ceutical interventions long after the power force is stopped. This
rol 393:69 – 83.
cannot be explained by attention because there is no more dual
Aston-Jones G, Chen S, Zhu Y, Oshinsky ML (2001) A neural circuit for
task. Second, tendon reflexes, which are spinally mediated, were
circadian regulation of arousal. Nat Neurosci 4:732–738.
clearly modified by the changes in 5-HT levels in the direction
consistent with the gain changes that we postulate altered force
Barbeau H, Rossignol S (1990) The effects of serotonergic drugs on the lo-
variances. Thus, these pieces of evidence suggest that divided
comotor pattern and on cutaneous reflexes of the adult chronic spinal cat.
Brain Res 514:55– 67.
attention cannot explain the observed variance increase in force
Boroojerdi B, Battaglia F, Muellbacher W, Cohen LG (2000) Voluntary
teeth clenching facilitates human motor system excitability. Clin Neuro-
It is noteworthy that our experiments involving pharmaceu-
physiol 111:988 –993.
tical intervention of 5-HT efficacy did not change the MVC. Dur-
Bowker RM, Westlund KN, Sullivan MC, Coulter JD (1982) Organization
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
J. Neurosci., September 17, 2014 • 34(38):12690 –12700 • 12699
of descending serotonergic projections to the spinal cord. In: Descending
Hounsgaard J, Hultborn H, Jespersen B, Kiehn O (1988) Bistability of
pathways to the spinal cord. Progress in Brain Res (Kuypers HGJM, Mar-
alpha-motoneurones in the decerebrate cat and in the acute spinal cat
tin GF, eds), pp 239 –265. Amsterdam: Elsevier.
after intravenous 5-hydroxytryptophan. J Physiol 405:345–367.
Brooke JD, Cheng J, Collins DF, McIlroy WE, Misiaszek JE, Staines WR
Hultborn H, Denton ME, Wienecke J, Nielsen JB (2003) Variable amplifi-
(1997) Sensori-sensory afferent conditioning with leg movement: gain
cation of synaptic input to cat spinal motoneurones by dendritic persis-
control in spinal reflex and ascending paths. Prog Neurobiol 51:393– 421.
tent inward current. J Physiol 552:945–952.
Hultborn H, Brownstone RB, Toth TI, Gossard JP (2004) Key mechanisms
Bui TV, Grande G, Rose PK (2008) Multiple modes of amplification of syn-
for setting the input-output gain across the motoneuron pool. Prog Brain
aptic inhibition to motoneurons by persistent inward currents. J Neuro-
Res 143:77–95.
physiol 99:571–582.
Hyngstrom AS, Johnson MD, Miller JF, Heckman CJ (2007) Intrinsic elec-
Carlton L, Newell K (1993) Force variability and characteristics of force
trical properties of spinal motoneurons vary with joint angle. Nat Neuro-
production. In: Force variability, pp 15–36. Champaign, IL: Human
sci 10:363–369.
Jacobs BL, Fornal CA (1993) 5-HT and motor control: a hypothesis. Trends
Carp JS, Rymer WZ (1986) Enhancement by serotonin of tonic vibration
Neurosci 16:346 –352.
and stretch reflexes in the decerebrate cat. Exp Brain Res 62:111–122.
Jacobs BL, Martín-Cora FJ, Fornal CA (2002) Activity of medullary se-
rotonergic neurons in freely moving animals. Brain Res Brain Res Rev
Chance FS, Abbott LF, Reyes AD (2002) Gain modulation from background
synaptic input. Neuron 35:773–782.
Jones KE, Hamilton AFC, Wolpert DM (2002) Sources of signal-dependent
Churchland MM, Yu BM, Cunningham JP, Sugrue LP, Cohen MR, Corrado
noise during isometric force production. J Neurophysiol 88:1533–1544.
GS, Newsome WT, Clark AM, Hosseini P, Scott BB, Bradley DC, Smith
MA, Kohn A, Movshon JA, Armstrong KM, Moore T, Chang SW, Snyder
Kawakita H, Kameyama O, Ogawa R, Hayes KC, Wolfe DL, Allatt RD (1991)
LH, Lisberger SG, Priebe NJ, et al. (2010) Stimulus onset quenches neu-
Reinforcement of motor evoked potentials by remote muscle contraction.
ral variability: a widespread cortical phenomenon. Nat Neurosci 13:369 –
J Electromyogr Kinesiol 1:96 –106.
Kawato M (1999) Internal models for motor control and trajectory plan-
Cushing S, Bui T, Rose PK (2005) Effect of nonlinear summation of synaptic
ning. Curr Opin Neurobiol 9:718 –727.
currents on the input– output properties of spinal motoneurons. J Neu-
Kernell D (2006) The motoneurone and its muscle fibres. Oxford:
rophysiol 94:3465–3478.
Dayan P, Huys QJM (2009) Serotonin in affective control. Annu Rev Neu-
Kuo JJ, Lee RH, Johnson MD, Heckman HM, Heckman CJ (2003) Active
rosci 32:95–126.
dendritic integration of inhibitory synaptic inputs in vivo. J Neurophysiol
Delwaide PJ, Toulouse P (1981) Facilitation of monosynaptic reflexes by
voluntary contraction of muscle in remote parts of the body. Mechanisms
Kuypers HG (1981) Anatomy of the descending pathways. In: The nervous
involved in the Jendrassik Manoeuvre. Brain 104:701–709.
system, Handbook of physiology (Brooks V, ed). Baltimore: Williams and
Devanne H, Lavoie BA, Capaday C (1997) Input-output properties and gain
Lee RH, Heckman CJ (2000) Adjustable amplification of synaptic input in
changes in the human corticospinal pathway. Exp Brain Res 114:329 –338.
the dendrites of spinal motoneurons in vivo. J Neurosci 20:6734 – 6740.
Dowman R, Wolpaw JR (1988) Jendrassik maneuver facilitates soleus
Mante V, Frazor RA, Bonin V, Geisler WS, Carandini M (2005) Indepen-
H-reflex without change in average soleus motoneuron pool membrane
dence of luminance and contrast in natural scenes and in the early visual
potential. Exp Neurol 101:288 –302.
system. Nat Neurosci 8:1690 –1697.
Enoka RM, Hutton RS, Eldred E (1980) Changes in excitability of tendon
Marino RJ, Graves DE (2004) Metric properties of the ASIA motor score:
tap and Hoffmann reflexes following voluntary contractions. Electroen-
subscales improve correlation with functional activities. Arch Phys Med
cephalogr Clin Neurophysiol 48:664 – 672.
Rehabil 85:1804 –1810.
Evinger C, Manning KA (1988) A model system for motor learning: adap-
Matthews PB (1972) Mammalian muscle receptors and their central ac-
tive gain control of the blink reflex. Exp Brain Res 70:527–538.
tions. London: Arnold.
Fallon JB, Macefield VG (2007) Vibration sensitivity of human muscle spin-
Miles GB, Hartley R, Todd AJ, Brownstone RM (2007) Spinal cholinergic
dles and Golgi tendon organs. Muscle Nerve 36:21–29.
interneurons regulate the excitability of motoneurons during locomo-
Fetz EE, Perlmutter SI, Prut Y (2000) Functions of mammalian spinal in-
tion. Proc Natl Acad Sci U S A 104:2448 –2453.
terneurons during movement. Curr Opin Neurobiol 10:699 –707.
Miyahara T, Hagiya N, Ohyama T, Nakamura Y (1996) Modulation of hu-
man soleus H reflex in association with voluntary clenching of the teeth.
Fullerton GS, Cattell JM (1892) On the perception of small differences. Uni-
J Neurophysiol 76:2033–2041.
versity of Pennsylvania Philosophical Series 2. Philadelphia: University of
Montague SJ, Fenrich KK, Mayer-Macaulay C, Maratta R, Neuber-Hess MS,
Rose PK (2013) Nonuniform distribution of contacts from noradrener-
Gregory JE, Mark RF, Morgan DL, Patak A, Polus B, Proske U (1990) Effects
gic and serotonergic boutons on the dendrites of cat splenius motoneu-
of muscle history on the stretch reflex in cat and man. J Physiol 424:93–
rons. J Comp Neurol 521:638 – 656.
Murray KC, Nakae A, Stephens MJ, Rank M, D'Amico J, Harvey PJ, Li X,
Harvey PJ, Li X, Li Y, Bennett DJ (2006) 5-HT2 receptor activation facili-
Harris RLW, Ballou EW, Anelli R, Heckman CJ, Mashimo T, Vavrek R,
tates a persistent sodium current and repetitive firing in spinal motoneu-
Sanelli L, Gorassini MA, Bennett DJ, Fouad K (2010) Recovery of mo-
rons of rats with and without chronic spinal cord injury. J Neurophysiol
toneuron and locomotor function after spinal cord injury depends on
96:1158 –1170.
constitutive activity in 5-HT2C receptors. Nat Med 16:694 –700.
Heckman C, Enoka RM (2012) Motor unit. Comp Physiol 2:2629 –2686.
Naito E, Roland PE, Ehrsson HH (2002) I feel my hand moving: a new role
Heckman CJ, Lee RH, Brownstone RM (2003) Hyperexcitable dendrites in
of the primary motor cortex in somatic perception of limb movement.
motoneurons and their neuromodulatory control during motor behav-
Neuron 36:979 –988.
ior. Trends Neurosci 26:688 – 695.
Newell KM, Carlton LG (1988) Force variability in isometric responses.
Heckman CJ, Hyngstrom AS, Johnson MD (2008) Active properties of mo-
J Exp Psychol Hum Percept Perform 14:37– 44.
toneurone dendrites: diffuse descending neuromodulation, focused local
Pe´re´on Y, Genet R, Guihe´neuc P (1995) Facilitation of motor evoked poten-
inhibition. J Physiol 586:1225–1231.
tials: timing of Jendrassik maneuver effects. Muscle Nerve 18:1427–1432.
Henneman E, Mendell L (1981) Functional organization of motoneuron
pool and its inputs. Handbook of physiology: the nervous system motor
Peterka RJ (2002) Sensorimotor integration in human postural control.
control, pp 423–507. Bethesda, MD: American Physiological Society.
J Neurophysiol 88:1097–1118.
Holstege JC, Kuypers HG (1987) Brainstem projections to spinal motoneu-
Power KE, McCrea DA, Fedirchuk B (2010) Intraspinally mediated state-
rons: an update. Neuroscience 23:809 – 821.
dependent enhancement of motoneurone excitability during fictive
12700 • J. Neurosci., September 17, 2014 • 34(38):12690 –12700
Wei et al. • 5-HT and Movement Gain Control in Spinal Cord
scratch in the adult decerebrate cat. J Physiol 588:2839 –2857.
Stedman A, Davey NJ, Ellaway PH (1998) Facilitation of human first dorsal
interosseous muscle responses to transcranial magnetic stimulation dur-
Powers RK, Binder MD (2001) Input-output functions of mammalian mo-
ing voluntary contraction of the contralateral homonymous muscle.
toneurons. Rev Physiol Biochem Pharmacol 143:137–263.
Muscle Nerve 21:1033–1039.
Prochazka A (1989) Sensorimotor gain control: a basic strategy of motor
Tazoe T, Sakamoto M, Nakajima T, Endoh T, Shiozawa S, Komiyama T
systems? Prog Neurobiol 33:281–307.
(2009) Remote facilitation of supraspinal motor excitability depends on
Robinson DA (1976) Adaptive gain control of vestibuloocular reflex by the
the level of effort. Eur J Neurosci 30:1297–1305.
cerebellum. J Neurophysiol 39:954 –969.
Teich MC, Heneghan C, Lowen SB, Ozaki T, Kaplan E (1997) Fractal char-
Schmidt RA, Zelaznik H, Hawkins B, Frank JS, Quinn Jr JT (1979) Motor-
acter of the neural spike train in the visual system of the cat. J Opt Soc Am
output variability: a theory for the accuracy of rapid motor acts. Psychol
A Opt Image Sci Vis 14:529 –546.
Wainberg M, Barbeau H, Gauthier S (1990) The effects of cyproheptadine
Schwartz O, Simoncelli EP (2001) Natural signal statistics and sensory gain
on locomotion and on spasticity in patients with spinal cord injuries.
control. Nat Neurosci 4:819 – 825.
J Neurol Neurosurg Psychiatry 53:754 –763.
Smirnakis SM, Berry MJ, Warland DK, Bialek W, Meister M (1997) Adap-
Zehr EP, Stein RB (1999) Interaction of the Jendrassik maneuver with seg-
tation of retinal processing to image contrast and spatial scale. Nature
mental presynaptic inhibition. Exp Brain Res 124:474 – 480.
Stam J (2000) Jendrassik's maneuver. Neurological eponyms, p 143. Ox-
Zhao HB, Santos-Sacchi J (1999) Auditory collusion and a coupled couple
ford, UK: Oxford UP.
of outer hair cells. Nature 399:359 –362.
Source: http://klab.smpp.northwestern.edu/wiki/images/8/81/Serotonin_gain_control.pdf
Human Reproduction Vol.19, No.10 pp. 2395–2400, 2004 Advance Access publication August 19, 2004 An increase in the absolute count of CD56dimCD161CD691NK cells in the peripheral blood is associated with a poorerIVF treatment and pregnancy outcome M.Y.Thum1,2,3,4, S.Bhaskaran2, H.I.Abdalla1, B.Ford2, N.Sumar2, H.Shehata3and A.S.Bansal2 1Lister Fertility Clinic, Lister Hospital, Chelsea Bridge Road, London SW1W 8RH, 2Immunology Department and 3Women HealthDepartment, Epsom and St Helier University Hospitals NHS Trust, Surrey, UK
The dysplastic nevus: From historical perspective to management in the modern era Part II. Molecular aspects and clinical management Keith Duffy, MD,a and Douglas Grossman, MD, PhDa,b Salt Lake City, Utah The following is a journal-based CME activity presented by the American Academy of Date of release: July 2012 Dermatology and is made up of four phases: Expiration date: July 2015

