Melis kk
■
BEHAVIORAL SCIENCE
Prevalence of Bruxism Awareness in a
Sardinian Population
Marcello Melis, D.M.D., R.Pharm.; Youssef S. Abou-Atme, D.D.S., M.S.
ABSTRACT: 1014 subjects on the island of Sardinia (Italy) were interviewed regarding the habit ofclenching and grinding their teeth. They had to specify if this activity occurred during the day, during thenight, or both. Other information recorded was their age, gender, marital status, and occupation. Overallprevalence of bruxism was 27.2% (276 subjects). No association was found between bruxism and age,
gender and job. Even differentiating diurnal, nocturnal, diurnal and nocturnal bruxism, associations were
000$05.00/0, THE JOURNAL OF
non-significant. Marital status seems to make some difference: divorced people reported higher para-
CRANIOMANDIBULAR
functional activity compared to widows and widowers who reported the least. Although awareness of
PRACTICE,Copyright 2003
bruxism is not a precise measure of parafunction, based on the results we cannot support the role of
by CHROMA, Inc.
stress on bruxism etiology.
Manuscript receivedJuly 8, 2002; revisedmanuscript receivedOctober 20, 2002; acceptedJanuary 28, 2003
Address for reprint requests:Dr. Marcello MelisVia Grosseto, 109125 - Cagliari,Italy
Dr. Marcello Melis received his degree
Bruxism is defined by the American Academy of
Orofacial Pain as a diurnal or nocturnal parafunc-
in pharmacy from the University of
tional activity including clenching, bracing,
Cagliari (Italy) in 1990, and a D.M.D.
gnashing, and grinding of the teeth.1 It is difficult to
degree from the dental school of the same
report the prevalence of this habit in the general popula-
university in 1998. From 1998 to 2000, hewas a resident at the Gelb Orofacial Pain
tion, because there are no gold standard methods to mea-
Center at Tufts University, Boston,
sure it. As shown in a review study performed by Seligman,
Massachusetts, U.S.A. Currently, Dr.
et al.,2 the prevalence depends on the way it is measured.
Melis practices in Cagliari in the field oftemporomandibular disorders and orofa-
Awareness of bruxism is low, about 15%, even though it
cial pain and has been involved in several
varies from one study to another;2-7 however, prevalence
international research activities focusing
increases to 50% if we clinically evaluate the subjects
on temporomandibular disorders andorofacial pain, occlusion, and muscle
interpreting dental attrition. If we interpret attrition eval-
uating study casts, it goes up to 91.5%, and finally usingnocturnal electromyographic (EMG) recordings we find
Dr. Youssef S. Abou-Atme received his
bruxism in 100% of the population2! This illustrates how
D.D.S. degree from the Université Saint
difficult is to detect parafunctional activity in the popula-
Joseph (Lebanon) in 1994. After finishing
tion. In fact, awareness is unquestionably a measure with
a residency in craniomandibular disor-ders from the Université de Nantes
low reliability, yet dental attrition (evaluated either clini-
(France) in 1996, he joined the Gelb Pain
cally or using dental casts) is not a sign of current brux-
Center at Tufts University (Boston, MA)
ism, but a cumulative record of tooth wear from both
were he completed a Fellowship in tem-poromandibular disorders (TMD) and
functional and parafunctional activity. In addition to that,
orofacial pain (1998) and received a
the amount of dental attrition is also related to age and
Masters Degree in oral biology. He
occlusal features of the subjects8,9 and is a sign of grind-
worked as a clinical and research associ-ate at the Gelb Center during the acade-
ing rather than clenching of the teeth. Also, EMG record-
mic year 1998-99. Dr. Abou-Atme's
ings are not completely reliable, because they detect not
practice in Lebanon is limited to TMD
only bruxism but also other nocturnal oral muscle activi-
and orofacial pain. He is also an activepain researcher at the Université Saint
ties such as myoclonus, somniloquy, and tics.8,10
The etiology of bruxism is also uncertain, but the
hypotheses fall into three major categories11:
BRUXISM IN A SARDINIAN POPULATION
MELIS AND ABOU-ATME
1. Local/mechanical factors
and masticatory muscles,47-51 even though not all the
2. Systemic/neurological factors
structures are affected in the same patient, but usually one
3. Psychological factors
gives up protecting the others.52
These categories are not mutually exclusive, and one or
Treatment is based on protecting the masticatory
the other can be true in different situations, even in the
system using occlusal appliances53-58 which avoid the
same subject.
damage to the teeth, periodontium, temporomandibular
Within the first category great importance has been
joints, and the masticatory muscles, and trying to reduce
given to occlusal factors with an attempt at interpreting
bruxism using stress management,59 biofeedback modali-
bruxism as an automatic reaction of the body to occlusal
ties,57,59,60 and, when needed, medications.59,61,62 Lately,
interferences with the purpose of eliminating them by
injections of botulinum toxin have been tried with some
grinding. Even though there are some data suggesting
that occlusion affects muscle activity leading to parafunc-
The purpose of this study was to detect the prevalence
tions,12-15 most of the studies seem to deny this correla-
of bruxism awareness in a specimen group drawn from
tion.16 In fact, occlusal adjustment failed to reduce
the population of the island of Sardinia (Italy), differenti-
masseter EMG nocturnal recordings in patients seeking
ating diurnal bruxism from nocturnal bruxism, and ana-
treatment for bruxism,17,18 and the placement of experi-
lyzing correlations between bruxism and other factors:
mental occlusal discrepancies did not cause an increase in
age, gender, marital status, and occupation.
nocturnal parafunctional activity.19
The choice was made because these factors, especially
Among the systemic and neurological factors, we can
marital status and occupation may influence the psychol-
report several medications that have been shown to elicit
ogy of the individual, affecting in turn parafunctional
bruxism, such as amphetamines,3 L-dopa,3,20 fenflu-
ramine,3,2l phenothiazine,3 other neuroleptics,22 selective
Additionally, diurnal and nocturnal bruxism which
serotonin reuptake inhibitors (SSRls),23-27 and all anti-
could be two separate issues and the result of different
psychotic agents which frequently cause dyskinesias:
factors, and might respond to different treatments.3,4,64,65
fluphenazine, haloperidol, loxapine, molindone, per-
This is why the authors chose to evaluate these two man-
phenazine, pimozide, thiothixene, trifluoperazine.28 Also
ifestations of bruxism separately.
recreational drugs (heroin, cocaine, ecstasy, marijuana,"crack", LSD, methadone) have been reported to increase
Materials and Methods
bruxism as well as other parafunctional oral activities.29
Some neurological pathologies may be associated with
One thousand fourteen (1014) Sardinian (citizens of
parafunctional oral activity. These are all disorders that
the island of Sardinia, Italy, population 1,423,808
are characterized by involuntary movements such as
[regional electoral lists 11/1999]) adult subjects were
dyskinesias,30 Parkinson's disease,30 and other extrapyra-
interviewed on their habit of clenching or grinding their
midal disorders.31,32
teeth during the day and/or during the night, on their age,
A lot has been written on psychological factors that are
gender, marital status, and occupation.
supposed to trigger bruxism. Stress seems to be the most
The following questions were in the questionnaire:
significant and the most frequently mentioned in the liter-
1. Do you have the habit of clenching, grinding your
ature. In some studies by Rugh, et al.,12,33 EMG nocturnal
teeth, sliding them between each other or keeping
monitoring showed a strong association between stressful
them tight together?
events (exams, family, and job problems) and muscle
And in case of a positive answer:
activity, and other studies had similar results.34 On the
2. During the day, during the night, or both?
other hand, other studies obtained different results.6,35,36
These questions were followed by information on age,
Type-A behavior has been related to bruxism evalu-
gender, marital status, and occupation. No effort was
ated by occlusal wear, especially if associated with higher
made to verify the data or to distinguish symptomatic
stress levels,38 other personality traits,39 and anxiety.37,40,41
from asymptomatic people. Several inves-tigators in dif-
But again, another study by Harness, et al.42 denied any
ferent social and occupational areas, but without stan-
association between bruxism and psychological distur-
dardized randomization, recruited the subjects.
bance as measured by the Minnesota multiphasic person-ality inventory (MMPI), agreeing with other studies.43
The effects of bruxism are indeed directed towards all
the structures of the stomatognathic system, including
In this study, we looked at different groups with differ-
teeth,44,46 periodontium,45 temporomandibular joints,47,48
ent characteristics. RxC table (contingency table) was
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
APRIL 2003, VOL. 21, NO. 2
MELIS AND ABOU-ATME
BRUXISM IN A SARDINIAN POPULATION
used to calculate the chi-square statistics to investigate
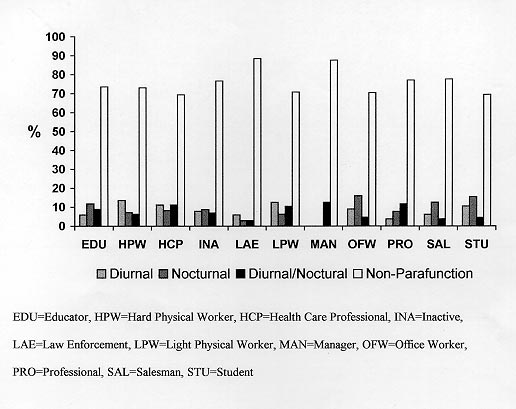
professional, inactive, law enforcement, light physical
the null hypothesis of no association between the row and
worker, manager, office worker, professional, salesper-
column variables.66 Statistical significance was accepted
son, and student. Statistical analysis did not show signif-
for p<0.05. For significant associations, Index of differ-
icant association between overall parafunction and job
ence (I dif.) was calculated in order to judge and classify
categories (chi-square =10.39, P>0.05). When analyzed
association factors.
regarding daily activity of parafunction: nocturnal, diur-nal, nocturnal/diurnal or nonparafunction, there was no
significant association with any job (chi-square = 37.37,
P>0.05), as shown in
Table 3,
Figure 3.
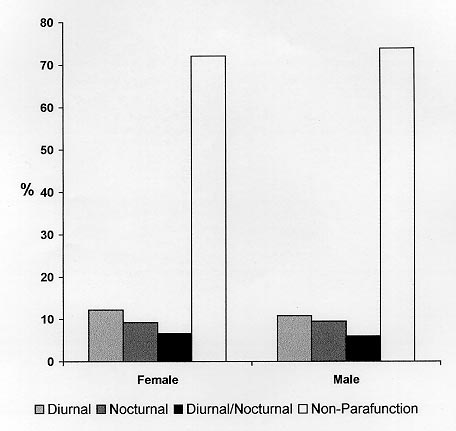
Gender: 1014 subjects answered the questionnaire,
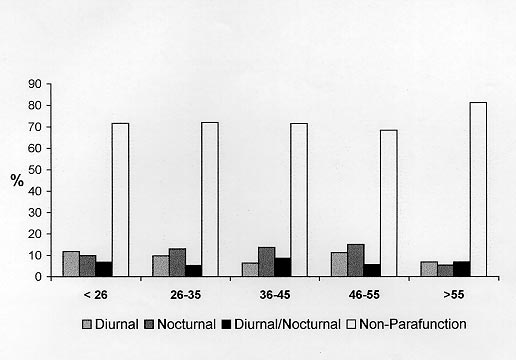
Age: As mentioned earlier, the mean age was 37.23
542 being females, and 472 males (53.5% F, 46.5% M;
years (SD 14.38, range 18-84). Subjects were grouped in
mean age 37.23 years, SD 14.38, range 18-84). 276 sub-
five age categories. Statistical analysis showed no signif-
jects (27.2%) reported bruxism. The data showed no sig-
icant association between overall parafunction and differ-
nificant difference between males and females regarding
ent age categories (chi-square = 6.65, P>0.05). When
parafunctional activity (chi-square = 0.4, p>0.05).
analyzed regarding daily activity of parafunction: noctur-
Diurnal/Nocturnal Bruxism: Even differentiating
nal, diurnal, diurnal/nocturnal or nonparafunction and
between diurnal and nocturnal parafunction data analysis
age categories (
Table 4 and
Figure 4), no significant
did not show significant gender difference between para-
associations were found (chi-square = 15.59, P>0.05).
function (either diurnal or nocturnal or diurnal/nocturnal)and nonparafunction groups (chi-square = 0.75, P>0.05).
Table 1 and
Figure 1 show gender distribution of para-
function.
Based on our results, 276 subjects reported some para-
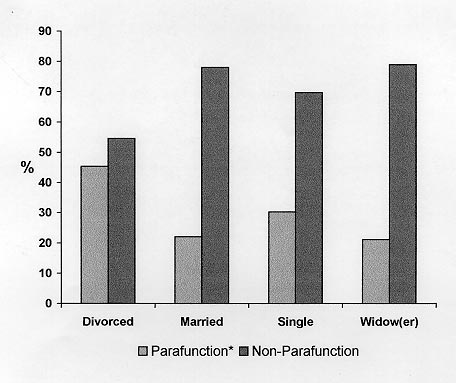
Marital Status: Out of 1014 subjects, 577 were single,
functional habit, which is 27.2% of the population we
396 married, 22 divorced, and 19 widows/widowers
examined. Even though the data found in the literature
(
Table 2,
Figure 2). Overall parafunctional activity
are not consistent and vary significantly probably due to
between these four marital status groups showed signifi-
the different populations surveyed and to different ways
cant difference (chi-square = 12.38, P<0.01). Based on
of evaluating bruxism, awareness seems to range from six
the Index of difference (I dif.=( E-O )/O) and following a
to 23%.2,8 Since the range is so wide, we can consider the
decreasing order, associations between parafunction and
percentage we obtained not so different, but we cannot
marital status were as follows: Divorced (0.40), Widow(er)
exclude some peculiarity due to differences in the exam-
(0.29), Married (0.24) and Single (0.10). Even though
ined population and probably to the way the questions on
very close to being statistically significant, marital status
the questionnaire were formulated. We also did not take
failed to show any significant association (chi-square =
into account the effect on bruxism of medications or neu-
16.8, P>0.05) related to nocturnal, diurnal, diurnal/noc-
rological diseases, because this information was not
turnal and nonparafunction groups.
included in the questionnaire. In addition to that, subjects
Occupation: Subjects were grouped in eleven job
in this study were selected and interviewed casually,
categories: educator, hard physical worker, health care
without any standardized randomization, leading to some
Gender Distribution of Diurnal and Nocturnal Parafunctional Activity
Parafunction and gender showed no significant association (chi-square = 0.75, P>0.05, df=3)
APRIL 2003, VOL. 21, NO. 2
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
BRUXISM IN A SARDINIAN POPULATION
MELIS AND ABOU-ATME
Figure 1
Gender distribution of diurnal and nocturnal
parafunctional activity (%).
involuntary selection bias, possibly altering the results of
found gender differences between diurnal and nocturnal
the survey. However, the number of the subjects (1014)
clenching and grinding behavior, with more men report-
should be high enough to help reduce this bias.
ing diurnal bruxism and more women reporting nocturnal
Comparing male to female subjects we could not
bruxism. Even though our results show a slightly higher
detect any significant difference in parafunctional habits.
number of females reporting nocturnal parafunction, this
This result agrees with Glaros, et al.'s4 study were overall
trend did not reach statistical significance, and no differ-
parafunctions where equal in men and women, but they
ences were found regarding diurnal and diurnal/nocturnal
Marital Status Distribution Between Parafunction and Nonparafunction
*Parafunction and marital status showed significant association (chi-square=12.38, P<0.01, df=3)
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
APRIL 2003, VOL. 21, NO. 2
MELIS AND ABOU-ATME
BRUXISM IN A SARDINIAN POPULATION
Figure 2
Marital distribution between parafunction and
nonparafunction (%).
bruxism. Another study2 reports higher bruxism scores in
Among the four Marital Status groups, the Divorced
males than in females, but the method they used to mea-
group showed the highest parafunctional activity, while
sure it was based on study cast evaluation and cannot be
Married and Widow(er) showed the least. Considering
a measure of awareness. That is why we cannot compare
that the Divorced group included only 22 people, and
the results.
Widow(er) 19, this small number compared to the othertwo groups (396 Married, 577 Single) might have given
Detailed Parafunctional Distribution Per Job
Hard physical worker
Health care professional
Light physical worker
Parafunctional and jobs showed no significant association (chi-square=37.37, P>0.05, df=30)
APRIL 2003, VOL. 21, NO. 2
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
BRUXISM IN A SARDINIAN POPULATION
MELIS AND ABOU-ATME
Figure 3
Detailed parafunctional distribution
per job (%).
us unreliable results. Conversely, divorced subjects could
high competition (professional, salesperson, student) to
lead a more stressful life, which may, in turn, elicit para-
show higher bruxism, but we did not detect this differ-
function. But here we must say that our overall results did
ence, even though students and health care professionals
not suggest a strong link between stress and bruxism.
seem to report more parafunctional activity.
In fact, different job categories did not seem to be asso-
If we consider that job is probably one of the most
ciated with different parafunctional activity, neither
common sources of stress, we may conclude that, in light
assessing it as a whole nor separately as diurnal and/or
of the results of this study, stress has no role in causing
nocturnal parafunctional activity. We could have expected
bruxism, agreeing with other previous studies.36,38,43,44
categories including jobs that share high responsibility
One limitation of this study is that we measured brux-
(health care professional, law enforcement, manager) or
ism prevalence asking the subjects if they "clench or
Detailed Parafunctional Age Distribution
Parafunction and age categories showed no significant association (chi-square = 15.59, P>0.05, df=12)
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
APRIL 2003, VOL. 21, NO. 2
MELIS AND ABOU-ATME
BRUXISM IN A SARDINIAN POPULATION
Figure 4
Detailed parafunctional age (years)
distribution (%).
grind their teeth" and bruxism awareness does not coin-
cide with actual bruxing activity; we could have subjectswho have such a parafunctional habit in spite of them
The authors would like to acknowledge Dr. Simona
being unaware of it. This limitation probably led to some
Foddis, Dr. Alessandro Piras, and Paolo Putzolu for their
bias and might have hidden a possible link between the
great help collecting the data.
variables we examined. Furthermore, we arbitrarilygrouped the jobs into categories within which subcate-
gories might not be uniformly stressful.
Observing the effect of age on parafunctions, our
Okeson JP (ed): Orofacial pain: guidelines for assessment, diagnosis, and
management. Chicago: Quintessence, 1996: 230 pages.
results agree with Seligman, et al.'s2 study, where no
Seligman DA, Pullinger AG, Solberg WK: The prevalence of dental attrition
association was found between bruxism and age. The
and its association with factors of age, gender, occlusion, and TMJ symp-tomatology. J Dent Res 1988; 67(10):1323-1333.
results of our study did not change after we divided the
Rugh JD, Ohrbach R: Occlusal parafunction. In: Mohl ND, Zarb GA,
overall bruxism into diurnal, nocturnal, and diurnal/noc-
Carlsson GE, eds. A textbook of occlusion. Chicago: Quintessence,1998:249-261.
turnal, confirming no association with age.
Glaros A: Incidence of diurnal and nocturnal bruxism. J Prosthet Dent 1981;
Gross AJ, Rivera-Morales WC, Gale EN: A prevalence study of symptoms
associated with TM disorders. J Craniomandib Disord Facial Oral Pain1988; 2:191-195.
Goulet JP, Lund JP, Montplaisir JY, Lavigne GJ: Daily clenching, nocturnal
All the data we collected seem to show that bruxism is
bruxism, and stress and their association with TMD symptoms [abstract].
not associated with gender, age, and work, but it is asso-
J Orofacial Pain 1993; 7:120.
Lavigne GJ, Montplaisir JY: Restless legs syndrome and sleep bruxism:
ciated to different marital statuses. The results do not
prevalence and association among Canadians. Sleep 1994; 17:739-743.
allow us to draw conclusions on the role of stress in elic-
Lobezoo F, Lavigne GJ: Do bruxism and temporomandibular disorders have
a cause-and-effect relationship? J Orofac Pain 1997; 11(1):15-23.
iting bruxism. In fact, even though some correlation
Seligman DA, Pullinger AG: The degree to which dental attrition in modern
might be assumed based on the differences between
society is a function of age and of canine contact. J Orofac Pain 1995;9:266-275.
different marital statuses, the data from different job cat-
Velly-Miguel AM, Montplaisir J, Rompré PH, Lund JP, Lavigne GJ:
egories do not support this hypothesis.
Bruxism and other orofacial movements during sleep. J CraniomandibDisord Facial Oral Pain 1992; 6:71-81.
From another point of view, what might be of impor-
Glaros AG, Rao SM. Bruxism: a critical review. Psychological reports. 1977;
tance is that stress is a personal experience, felt differ-
Okeson JP: Etiology of functional disturbances in the masticatory system. In:
ently by different individuals, and probably different
Okeson JP, ed. Management of temporomandibular disorders and occlu-
ways of coping with stress lead to bruxism rather than
sion. 4th ed. St. Louis: Mosby Year Book, 1998;149-179.
Leung AK, Robson WL: Bruxism: how to stop tooth grinding and clenching.
stress itself.
Postgrad Med 1991; 89:523-546.
APRIL 2003, VOL. 21, NO. 2
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
BRUXISM IN A SARDINIAN POPULATION
MELIS AND ABOU-ATME
Meklas JF: Bruxism: diagnosis and treatment. J Acad Gen Dent 1971; 19:31-
disturbance and bruxism in the facial pain population. J Craniomandib
Pract 1992; 10(1):70-74.
Ramfjord SP, Ash MM: Occlusion. 2nd ed. Philadelphia: WB Saunders,
Rao SM, Glaros AG: Electromyographic correlates of experimentally
induced stress in diurnal bruxists and normals. J Dent Res 1979; 58(9):
Lobezoo F, Naeije M: Bruxism is mainly regulated centrally, not peripher-
ally. J Oral Rehab 2001; 28(12):1085-1091.
Xhonga FA: Bruxism and its effect on the teeth. J Oral Rehabil 1977;
Bailey JR, Rugh JD: Effect of occlusal adjustment on bruxism as monitored
by nocturnal EMG recordings [Abstract]. J Dent Res 1980; 59:317.
Pavone BW: Bruxism and its effect on the natural teeth. J Prosthet Dent
Kardachi BJ, Bailey JO, Jr, Ash MM, Jr: A comparison of biofeedback and
occlusal adjustments on bruxism. J Periodontol 1978; 19:376.
Kleinberg I: Bruxism: etiology, clinical signs and symptoms. Aust Prosth J
Rugh JD, Barghi N, Drago CJ: Experimental occlusal discrepancies and noc-
1994; 8:9-17.
turnal bruxism. J Prosthet Dent 1984; 51(4):548-553.
Molina OF, dos Santos J, Nelson SJ, Nowlin T: A clinical study of specific
Magee KR: Bruxism related to levodopa therapy. JAMA 1970; 214(1):147.
signs and symptoms of CMD in bruxers classified by the degree of sever-
Brandon S: Unusual effect of fenfluramine. Br Med J 1969; 4:557-558.
ity. J Craniomandib Pract 1999; 17(4):268-279.
Amir I, Hermesh H, Gavish A: Bruxism secondary to antipsychotic drug
Glaros AG, Forbes M, Shanker J, Glass EG: Effect of parafunctional clench-
exposure: a positive response to propranolol. Clin Neuropharma 1997;
ing on temporomandibular disorder pain and proprioceptive awareness. J
Craniomandib Pract 2000; 18(3):198-204.
Ellison JM, Stanziani P: SSRI-associated nocturnal bruxism in four patients.
Travell JG, Simons DG: Myofascial pain and dysfunction. The trigger point
J Clin Psych 1993; 54:432-434.
manual. Baltimore: Williams & Wilkins, 1983; 223-224, 239-240, 252,
Romanelli F, Adler DA, Bungay KM: Possible paroxetine-induced bruxism.
264-270, 276-280.
Ann Pharmacother 1996; 30:1246-1248.
Glaros AG, Tabacchi KN, Glass EG: Effect of parafunctional activity on
Gerber PE, Lynd LD: Selective serotonin-reuptake inhibitor-induced move-
TMD pain. J Orofac Pain 1998; 12(2):145-152.
ment disorders. Ann Pharmacother 1998; 32:692-698.
Arima T, Svensson P, Arendt-Nielsen L: Experimental grinding in healthy
Bostwick JM, Jaffee MS: Buspirone as an antidote to SSRI-induced bruxism
subjects: a model for postexercise jaw muscle soreness? J Orofac Pain
in four cases. J Clin Psych 1999; 60(12):857-860.
Lobezoo F, van Denderen JA, Verheij JGC, Naeije M: Reports of SSRI asso-
Mehta NR, Forgione AG, Maloney G, Greene R: Different effects of noctu-
ciated bruxism in the family physician's office. J Orofac Pain 2001;
mal parafunction on the masticatory system: the weak link theory. J
Craniomandib Pract 2000; 18(4):280-285.
Lacy CF, Armstrong LL, Goldman MP, Lance LL: Drug information hand-
Solberg WK, Clark GT, Rugh JD: Nocturnal electromyographic evaluation of
book. 7th ed. Hudson: Lexi-Comp Inc. 1999; 1305.
bruxism patients undergoing a short term splint therapy. J Oral Rehabil
Winocur E, Gavish A, Volfin G, Halachmi M, Gazit E: Oral motor parafunc-
1975; 2(3):215-223.
tions among heavy drug addicts and their effects on signs and symptoms of
Okeson JP: The effects of hard and soft occlusal splints on nocturnal bruxism.
temporomandibular disorders. J Orofac Pain 2001; 15(1):56-63.
JADA 1987; 114(6):788-791.
Watts MW, Tan EK, Jankovic J: Bruxism and cranial-cervical dystonia: is
Messing SG: Splint therapy. In: Kaplan AS, Assael LA (eds). Temporo-
there a relationship. J Craniomandib Pract 1999; 17(3): 196-201.
mandibular disorders: diagnosis and treatment. Philadelphia: W.B.
Tan EK, Jankovic J, Ondo W: Bruxism in Huntington's disease. Movement
Saunders Company, 1991:395-454.
Disorders 2000; 15(1):171-173.
Okeson JP: General considerations in the treatment of temporomandibular
Louis ED, Tampone E: Bruxism in Huntington's disease. Movement
disorders. In: Okeson JP, ed. Management of temporomandibular disor-
Disorders 2001; 16(4):785-786.
ders and occlusion. 4th ed. St. Louis: Mosby Year Book, 1998:355-389
Rugh JD, Solberg WK: Psychological implications in temporomandibular
Okeson JP: Treatment of masticatory muscle disorders. In: Okeson JP, ed.
pain and dysfunction. In: Zarb GA, Carlsson GE, eds. Temporomandibular
Management of temporomandibular disorders and occlusion. 4th ed. St.
joint function and dysfunction. Copenhagen: Munksgaard, 1979; 255.
Louis: Mosby Year Book, 1998:391-411.
Hicks RA, Conti PA: Nocturnal bruxism and self reports of stress related
Pertes RA: Occlusal appliance therapy. In: Pertes RA, Gross SG, eds. Clinical
symptoms. Perceptual & Motor Skills 1991; 72:1182.
management of temporomandibular disorders and orofacial pain. Chicago:
Westrup DA, Keller SR, Nellis TA, Hicks RA: Arousability and bruxism in
Quintessence Publishing Co. Inc, 1995:197-209.
male and female college students. Perceptual & Motor Skills 1992; 75(3 Pt
Hathaway KM: Behavioral and psychological management. In: Pertes RA,
Gross SG, eds. Clinical management of temporomandibular disorders and
Pierce CJ, Chrisman K, Bennet ME, Close JM: Stress, anticipatory stress, and
orofacial pain. Chicago: Quintessence Publishing Co. Inc. 1995:245-252.
psychologic measures related to sleep bruxism. J Orofac Pain 1995;
Cannistraci AJ, Friedrich MA: A multidimensional approach to bruxism and
TMD. NYS Dent J 1987:31-34.
Major M, Rompré PH, Guitard F, Tenbokum L, O'Connor K, Nielsen T,
Raigrodski AJ, Christensen LV, Mohamed SE, Gardiner DM: The effect of
Lavigne GJ: A controlled daytime challenge of motor performance and vig-
four-week administration of amitriptyline on sleep bruxism. A double-
ilance in sleep bruxers. J Dent Res 1999; 78:1754-1762.
blind crossover clinical study. J Craniomandib Pract 2001; 19(1):21-25.
Pingitore G, Chrobak V, Petrie J: The social and psychologic factors of brux-
Melis M: Dr. Melis comments on Raigrodski, et al.'s article in the January
ism. J Prosthet Dent 1991; 65(3):443-446.
2001 issue of CRANIO [Letter to the Editor]. J Craniomandib Pract
Fischer WF, O'Toole ET: Personality characteristics of chronic bruxers.
Behav Med 1993; 19(2):82-86.
Tan EK, Jankowic J: Treating severe bruxism with botulinum toxin. JADA
Kampe T, Edman G, Hannerz H: Ten-year follow-up study of personality
2000; 131 :211-216.
traits in adults with intact and restored dentitions. J Oral Rehabil 1996;
Ramfjord SP: Bruxism, a clinical and electromyographic study. JADA 1961;
da Silva AM, Oakley DA, Hemmings KW, Newman HN, Watkins S:
Rugh JD, Harlan J: Nocturnal bruxism and temporomandibular disorders.
Psychosocial factors and tooth wear with a significant component of attri-
Advances in Neurology 1988;49:329-341.
tion. Eur J Prosth & Rest Dent 1997; 5(2):51-55.
Weintraub JA, Douglass CW, Gillings DB: Biostats, data analysis for dental
Harness DM, Peltier B: Comparison of MMPI scores with self-report of sleep
health care professionals. 2nd ed. Boston: CAVCO, Inc. 1985:145-151.
THE JOURNAL OF CRANIOMANDIBULAR PRACTICE
APRIL 2003, VOL. 21, NO. 2
Source: http://www.marcello-melis.it/pdf/new/Prevalence%20of%20bruxism%20awareness%20in%20a%20Sardinian%20population.pdf
U.S. Postage Twin Cities, MN 200 University Ave. E. Permit No. 5388 St. Paul, MN 55101 Angela Sinner, D.O. Pediatric Rehabilitation A Pediatric Perspective focuses on specialized topics in pediatrics, orthopedics, neurology, neurosurgery and rehabilitation A Range of Treatment Options
Colloque Supméca 2015 - Les Assemblages Mécaniques Développement d'un assemblage bimétallique hétérogène pour l'ultravide 1Sominex SAS, Recherche et Développement, 13, rue de la résistance, 14400 Bayeux, France Résumé. Sominex, PME manufacturière œuvrant dans le secteur de la recherche scientifique, cherche à se développer en innovant dans des produits et des procédés de fabrication permettant de répondre aux exigences de ses clients, notamment dans le domaine des accélérateurs de particules pour lequel le savoir-faire de l'entreprise est déjà bien reconnu. Dans ce cadre Sominex a développé une bride bimétallique constituée d'un anneau extérieur en acier inoxydable et d'un cœur en alliage d'aluminium. Ces deux matériaux, non miscible par soudage par voie liquide, sont assemblé conjointement de manière mécanique et par soudure par procédé de friction malaxage entre les deux matériaux. La liaison mécanique permettant d'assurer les caractéristiques mécaniques de l'assemblage et la soudure par friction malaxage son étanchéité. Ce procédé de soudage, développé de manière récente, permet dans ce cas, de générer des couches d'intermétalliques à l'interface des deux matériaux. Ces couches sont de suffisamment faible épaisseur (de 1 à 6 micromètres) pour ne pas fragiliser la liaison outre mesure, et leur grande compacité permet d'obtenir une étanchéité parfaite.

