Pri.rn.dk
Seventh Report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure
Aram V. Chobanian, George L. Bakris, Henry R. Black, William C. Cushman, Lee A.
Green, Joseph L. Izzo, Jr, Daniel W. Jones, Barry J. Materson, Suzanne Oparil,
Jackson T. Wright, Jr, Edward J. Roccella and the National High Blood Pressure
Education Program Coordinating Committee
2003;42;1206-1252; originally published online Dec 1, 2003;
DOI: 10.1161/01.HYP.0000107251.49515.c2
Hypertension is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
Copyright 2003 American Heart Association. All rights reserved. Print ISSN: 0194-911X. Online
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
Subscriptions: Information about subscribing to Hypertension is online at
Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of WoltersKluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax:410-528-8550. E-mail:
Reprints: Information about reprints can be found online at
JNC 7 – COMPLETE VERSION
SEVENTH REPORT OF THE JOINT NATIONAL
COMMITTEE ON PREVENTION, DETECTION,
EVALUATION, AND TREATMENT OF HIGH
Aram V. Chobanian, George L. Bakris, Henry R. Black, William C. Cushman, Lee A. Green,
Joseph L. Izzo, Jr, Daniel W. Jones, Barry J. Materson, Suzanne Oparil, Jackson T. Wright, Jr,
Edward J. Roccella, and the National High Blood Pressure Education Program Coordinating Committee
Abstract—The National High Blood Pressure Education Program presents the complete Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Like its predecessors,
the purpose is to provide an evidence-based approach to the prevention and management of hypertension. The key
messages of this report are these: in those older than age 50, systolic blood pressure (BP) of greater than 140 mm Hg
is a more important cardiovascular disease (CVD) risk factor than diastolic BP; beginning at 115/75 mm Hg, CVD risk
doubles for each increment of 20/10 mm Hg; those who are normotensive at 55 years of age will have a 90% lifetime
risk of developing hypertension; prehypertensive individuals (systolic BP 120 –139 mm Hg or diastolic BP 80 – 89
mm Hg) require health-promoting lifestyle modifications to prevent the progressive rise in blood pressure and CVD; for
uncomplicated hypertension, thiazide diuretic should be used in drug treatment for most, either alone or combined with
drugs from other classes; this report delineates specific high-risk conditions that are compelling indications for the use
of other antihypertensive drug classes (angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers,
beta-blockers, calcium channel blockers); two or more antihypertensive medications will be required to achieve goal BP
(⬍140/90 mm Hg, or ⬍130/80 mm Hg) for patients with diabetes and chronic kidney disease; for patients whose BP
is more than 20 mm Hg above the systolic BP goal or more than 10 mm Hg above the diastolic BP goal, initiation of therapy
using two agents, one of which usually will be a thiazide diuretic, should be considered; regardless of therapy or care,
hypertension will be controlled only if patients are motivated to stay on their treatment plan. Positive experiences, trust in the
clinician, and empathy improve patient motivation and satisfaction. This report serves as a guide, and the committee continues
to recognize that the responsible physician's judgment remains paramount.
(Hypertension. 2003;42:1206 –1252.)
For more than 3 decades, the National Heart, Lung, and hypertension may be as much as 1 billion individuals, and
Blood Institute (NHLBI) has administered the National
approximately 7.1 million deaths per year may be attributable
High Blood Pressure Education Program (NHBPEP) Coordi-
to hypertension.3 The World Health Organization reports that
nating Committee, a coalition of 39 major professional,
suboptimal BP (⬎115 mm Hg SBP) is responsible for 62% of
public, and voluntary organizations and 7 federal agencies.
cerebrovascular disease and 49% of ischemic heart disease,
One important function is to issue guidelines and advisories
with little variation by sex. In addition, suboptimal blood
designed to increase awareness, prevention, treatment, and
pressure is the number one attributable risk for death through-
control of hypertension (high blood pressure).
Data from the National Health and Nutrition Examination
Considerable success has been achieved in the past in
Survey (NHANES) have indicated that 50 million or more
meeting the goals of the program. The awareness of hyper-
Americans have high blood pressure (BP) warranting some
tension has improved from a level of 51% of Americans in the
form of treatment.1,2 Worldwide prevalence estimates for
period 1976 to 1980 to 70% in 1999 to 2000 (Table 1). The
Received November 5, 2003; revision accepted November 6, 2003.
From Boston University School of Medicine (A.V.C.), Boston, Mass; Rush University Medical Center (G.L.B., H.R.B.), Chicago, Ill; Veterans Affairs
Medical Center (W.C.C.), Memphis, Tenn; University of Michigan (L.A.G.), Ann Arbor, Mich; State University of New York at Buffalo School ofMedicine (J.L.I. Jr.), Buffalo, NY; University of Mississippi Medical Center (D.W.J.), Jackson, Miss; University of Miami (B.J.M.), Miami, Fla;University of Alabama at Birmingham (S.O.), Birmingham, Ala; Case Western Reserve University (J.T.W. Jr.), Cleveland, Ohio; National Heart, Lung,and Blood Institute (E.J.R.), Bethesda, Md.
The executive committee, writing teams, and reviewers served as volunteers without remuneration.
Members of the National High Blood Pressure Education Program Coordinating Committee are listed in the Appendix.
Correspondence to Edward J. Roccella, PhD, Coordinator, National High Blood Pressure Education Program, National Heart, Lung, and Blood
Institute, National Institutes of Health, Building 31, Room 4A10, 31 Center Drive MSC 2480, Bethesda, MD 20892. E-mail
[email protected]
2003 American Heart Association, Inc.
Hypertension is available at http://www.hypertensionaha.org

Chobanian et al
JNC 7 – COMPLETE REPORT
Trends in Awareness, Treatment, and Control of
High Blood Pressure 1976 –2000
National Health and Nutrition Examination Survey, %
Percentage of adults aged 18 to 74 years with systolic blood pressure (SBP)
of 140 mm Hg or greater, diastolic blood pressure (DBP) of 90 mm Hg orgreater, or taking antihypertensive medication.
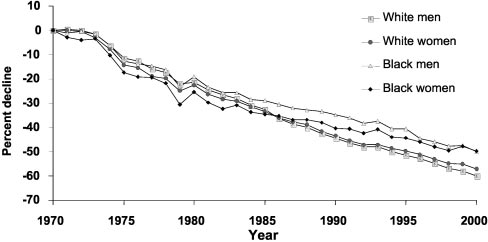
Figure 2. Percentage decline in age-adjusted mortality rates for
*SBP below 140 mm Hg and DBP below 90 mm Hg and on antihypertensive
stroke by gender and race: United States, 1970 to 2000.
Source: Prepared by T. Thom, National Heart, Lung, and BloodInstitute from Vital Statistics of the United States, National Cen-ter for Health Statistics. Death rates are age-adjusted to the
percentage of patients with hypertension receiving treatment
2000 US census population.
has increased from 31% to 59% in the same period, and thepercentage of persons with high BP controlled to below
Furthermore, the rates of decline of deaths from CHD and
140/90 mm Hg has increased from 10% to 34%. Between
stroke have slowed in the past decade. In addition, the
1960 and 1991, median systolic BP (SBP) for individuals 60
prevalence and hospitalization rates of HF, wherein the
to 74 years old declined by approximately 16 mm Hg (Figure
majority of patients have hypertension before developing
1). These changes have been associated with highly favorable
heart failure, have continued to increase (Figures 5 and 6).
trends in the morbidity and mortality attributed to hyperten-
Moreover, there is an increasing trend in end-stage renal
sion. Since 1972, age-adjusted death rates from stroke and
disease (ESRD) by primary diagnosis. Hypertension is sec-
coronary heart disease (CHD) have declined by approxi-
ond only to diabetes as the most common antecedent for this
mately 60% and 50%, respectively (Figures 2 and 3). These
condition (Figure 7). Undiagnosed, untreated, and uncon-
benefits have occurred independent of gender, age, race, or
trolled hypertension clearly places a substantial strain on the
socioeconomic status. Within the last 2 decades, better
health care delivery system.
treatment of hypertension has been associated with a consid-erable reduction in the hospital case-fatality rate for heartfailure (HF) (Figure 4). This information suggests that there
have been substantial improvements.
The decision to appoint a committee for The Seventh Report of the
However, these improvements have not been extended to
Joint National Committee on Prevention, Detection, Evaluation, and
the total population. Current control rates for hypertension in
Treatment of High Blood Pressure (JNC 7) was based on 4 factors:the publication of many new hypertension observational studies and
the United States are clearly unacceptable. Approximately
clinical trials since the last report was published in 19974; the need
30% of adults are still unaware of their hypertension, more
for a new clear and concise guideline that would be useful to
than 40% of individuals with hypertension are not on treat-
clinicians; the need to simplify the classification of BP; and a clear
ment, and two thirds of hypertensive patients are not being
recognition that the JNC reports did not result in maximum benefit
controlled to BP levels less than 140/90 mm Hg (Table 1).
to the public. This JNC report is presented in 2 separate publications.
The initial "Express" version, a succinct practical guide, waspublished in the May 21, 2003, issue of the Journal of the AmericanMedical Association.5 The current, more comprehensive reportprovides a broader discussion and justification for the recommenda-tions made by the committee. As with prior JNC reports, the
Figure 3. Percentage decline in age-adjusted mortality rates for
CHD by gender and race: United States, 1970 to 2000. Source:
Figure 1. Smoothed weighted frequency distribution, median,
Prepared by T. Thom, National Heart, Lung, and Blood Institute
and 90th percentile of SBP for ages 60 to 74 years, United
from Vital Statistics of the United States, National Center for
States, 1960 to 1991. Source: Burt et al. Hypertension
Health Statistics. Death rates are age-adjusted to the 2000 US
1995;26:60 – 69. Erratum in: Hypertension 1996;27:1192.
census population.
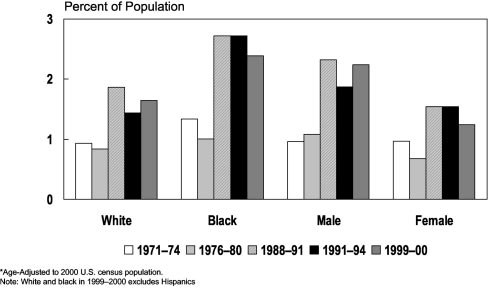
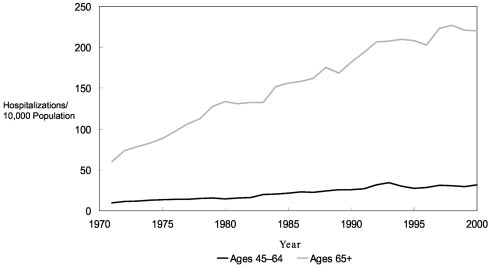
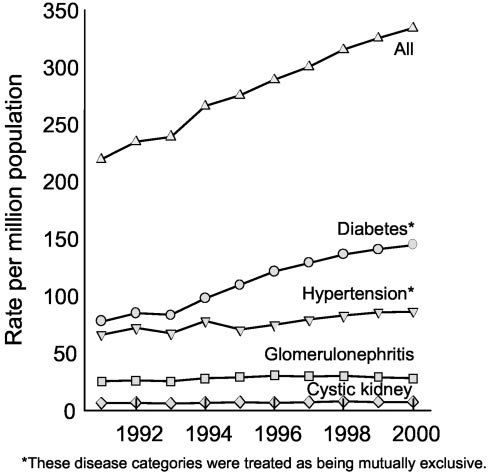
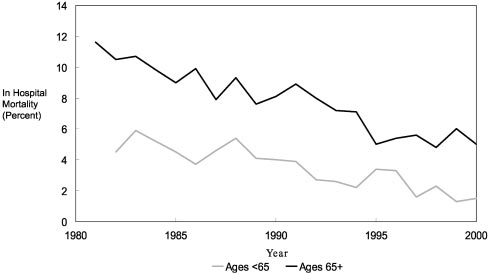
Figure 6. Hospitalization rates for congestive heart failure, ages
Figure 4. Hospital case-fatality rates for congestive heart failure,
45 to 64 and 65⫹: United States, 1971 to 2000. Source:
ages ⬍65 and 65⫹: United States, 1981 to 2000. Source:
National Heart, Lung, and Blood Institute. Morbidity and Mortal-
National Heart, Lung, and Blood Institute. Morbidity and Mortal-
ity: 2002 Chart Book on Cardiovascular, Lung, and Blood Dis-
ity: 2002 Chart Book on Cardiovascular, Lung, and Blood Dis-
ease. Chart 3–35. Accessed September 2003.
ease. Chart 3–36. Accessed September 2003.
appointed the JNC 7 chair and an Executive Committee derived from
committee recognizes that the responsible physician's judgment is
the Coordinating Committee membership. The Coordinating Com-
paramount in managing his or her patients.
mittee members served on 1 of 5 JNC 7 writing teams, which
Since the publication of the JNC 6 report, the NHBPEP Coordi-
contributed to the writing and review of the document.
nating Committee, chaired by the director of the NHLBI, has
The concepts for the new report identified by the NHBPEP
regularly reviewed and discussed studies on hypertension. To con-
Coordinating Committee membership were used to create the report
duct this task, the Coordinating Committee is divided into 4
outline. On the basis of these critical issues and concepts, the
subcommittees: Science Base; Long Range Planning; Professional,
Executive Committee developed relevant medical subject headings
Patient, and Public Education; and Program Organization. The
(MeSH) terms and keywords to further review the scientific litera-
subcommittees work together to review the hypertension scientific
ture. These MeSH terms were used to generate MEDLINE searches
literature from clinical trials, epidemiology, and behavioral science.
that focused on English-language, peer-reviewed scientific literature
In many instances, the principal investigator of the larger studies has
from January 1997 through April 2003. Various systems of grading
presented the information directly to the Coordinating Committee.
the evidence were considered, and the classification scheme used in
The committee reviews are summarized and posted on the NHLBI
JNC 6 and other NHBPEP clinical guidelines was selected.4,7–10 This
web site.6 This ongoing review process keeps the committee apprisedof the current state of the science, and the information is also used to
scheme classifies studies according to a process adapted from Last
develop program plans for future activities, such as continuing
and Abramson (see the section Scheme Used for Classification of the
During fall 2002, the NHBPEP Coordinating Committee chair
In reviewing the exceptionally large body of research literature in
solicited opinions regarding the need to update the JNC 6 report. The
hypertension, the Executive Committee focused its deliberations on
entire Coordinating Committee membership provided, in writing, adetailed rationale explaining the necessity for updating JNC 6,outlined critical issues, and provided concepts to be addressed in thenew report. Thereafter, the NHBPEP Coordinating Committee chair
Figure 5. Prevalence of CHF by race and gender, ages 25 to
74: United States, 1971 to 1974 to 1999 to 2000. Age-adjusted
to 2000 US census population. White and African American in
1999 to 2000 excludes Hispanics. Source: National Heart, Lung,
and Blood Institute. Morbidity and Mortality: 2002 Chart Book
on Cardiovascular, Lung, and Blood Disease. Accessed Sep-
Figure 7. Trends in incident rates of ESRD, by primary diagno-
sis (adjusted for age, gender, race). Disease categories were
book.htm and 1999 to 2000 unpublished data computed by M.
treated as being mutually exclusive. Source: United States
Wolz and T. Thom, National Heart, Lung, and Blood Institute.
Renal Data System. 2002. Figure 1.14. Accessed September,
Chobanian et al
JNC 7 – COMPLETE REPORT
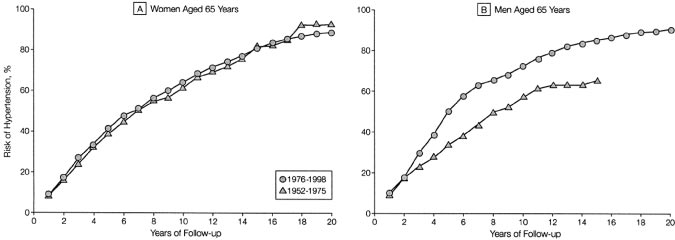
Figure 8. Residual lifetime risk of hyper-
tension in women and men aged 65
years. Cumulative incidence of hyperten-
sion in 65-year-old women and men.
Data for 65-year-old men in the 1952 to
1975 period are truncated at 15 years
since there were few participants in this
age category who were followed up
beyond this time interval. Source: JAMA
2002;287:1003–1010. Copyright 2002,
American Medical Association. All rights
reserved.
evidence pertaining to outcomes of importance to patients and with
circulated among the Coordinating Committee members for review and
effects of sufficient magnitude to warrant changes in medical
comment. The JNC 7 chair synthesized the comments, and the longer
practice ("patient oriented evidence that matters" [POEMs]).12,13
version was submitted to the journal Hypertension in November, 2003.
Patient-oriented outcomes include not only mortality but also otheroutcomes that affect patients' lives and well-being, such as sexual
Lifetime Risk of Hypertension
function, ability to maintain family and social roles, ability to work,
Hypertension is an increasingly important medical and public
and ability to carry out activities of daily living. These outcomes are
health issue. The prevalence of hypertension increases with
strongly affected by nonfatal stroke, HF, coronary heart disease, and
advancing age to the point where more than half of people
renal disease; hence, these outcomes were considered along withmortality in the committee's evidence-based deliberations. Studies of
aged 60 to 69 years old and approximately three-fourths of
physiological end points (disease-oriented evidence [DOEs]) were
those aged 70 years and older are affected.1 The age-related
used to address questions where POEMs were not available.
rise in SBP is primarily responsible for an increase in both
The Coordinating Committee began the process of developing the
incidence and prevalence of hypertension with increasing
JNC 7 Express report in December 2002, and the report was
submitted to the Journal of the American Medical Association inApril 2003. It was published in an electronic format on May 14,
Whereas the short-term absolute risk for hypertension is
2003, and in print on May 21, 2003. During this time, the Executive
conveyed effectively by incidence rates, the long-term risk is
Committee met on 6 occasions, 2 of which included meetings with
best summarized by the lifetime risk statistic, which is the
the entire Coordinating Committee. The writing teams also met by
probability of developing hypertension during the remaining
teleconference and used electronic communications to develop the
years of life (either adjusted or unadjusted for competing
report. Twenty-four drafts were created and reviewed repeatedly. At
causes of death). Framingham Heart Study investigators
its meetings, the Executive Committee used a modified nominalgroup process14 to identify and resolve issues. The NHBPEP
recently reported the lifetime risk of hypertension to be
Coordinating Committee reviewed the penultimate draft and pro-
approximately 90% for men and women who were nonhy-
vided written comments to the Executive Committee. In addition, 33
pertensive at 55 or 65 years old and survived to age 80 to 85
national hypertension leaders reviewed and commented on the
(Figure 8).16 Even after adjusting for competing mortality, the
document. The NHBPEP Coordinating Committee approved the
remaining lifetime risks of hypertension were 86 to 90% in
JNC 7 Express report. To complete the longer JNC 7 version, theExecutive Committee members met via teleconferences and in
women and 81 to 83% in men.
person and circulated sections of the larger document via e-mail. The
The impressive increase of BP to hypertensive levels with
sections were assembled and edited by the JNC 7 chair and were
age is also illustrated by data indicating that the 4-year rates
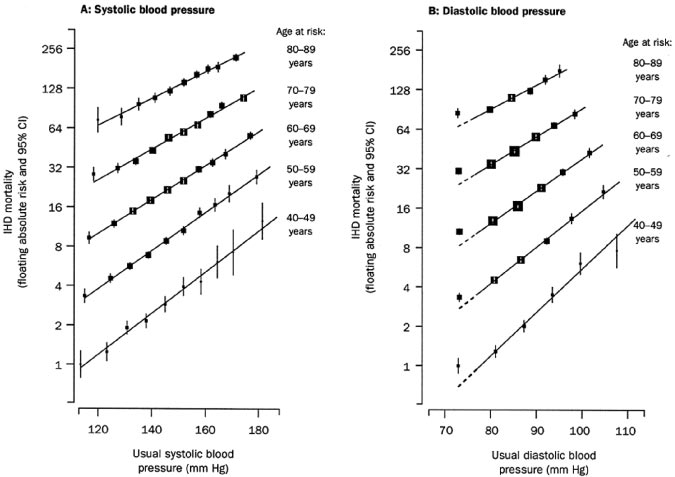
Figure 9. Ischemic heart disease (IHD)
mortality rate in each decade of age ver-
sus usual blood pressure at the start of
that decade. Source: Reprinted with per-
mission from Elsevier (The Lancet,
2002;360:1903–1913).
Figure 10. Stroke mortality rate in each
decade of age versus usual blood pres-
sure at the start of that decade. Source:
Reprinted with permission from Elsevier
(The Lancet, 2002;360:1903–1913).
of progression to hypertension are 50% for those 65 years and
In addition, longitudinal data obtained from the Framing-
older with BP in the 130 to 139/85 to 89 mm Hg range and
ham Heart Study have indicated that BP values in the 130 to
26% for those with BP in the 120 to 129/80 to 84 mm Hg
139/85 to 89 mm Hg range are associated with a more than
2-fold increase in relative risk from cardiovascular disease(CVD) compared with those with BP levels below 120/
Blood Pressure and Cardiovascular Risk
80 mm Hg (Figure 11).19
Data from observational studies involving more than 1million individuals have indicated that death from bothischemic heart disease and stroke increases progressively and
Basis for Reclassification of Blood Pressure
linearly from BP levels as low as 115 mm Hg systolic and
Because of the new data on lifetime risk of hypertension and
75 mm Hg diastolic upward (Figures 9 and 10).18 The
the impressive increase in the risk of cardiovascular compli-
increased risks are present in all age groups ranging from 40
cations associated with levels of BP previously considered to
to 89 years old. For every 20 mm Hg systolic or 10 mm Hg
be normal, the JNC 7 report has introduced a new classifica-
diastolic increase in BP, there is a doubling of mortality from
tion that includes the term "prehypertension" for those with
both ischemic heart disease and stroke.
BPs ranging from 120 to 139 mm Hg systolic and/or 80 to
Figure 11. Impact of high normal blood pressure on the risk of cardiovascular disease. Cumulative incidence of cardiovascular events
in women (A) and men (B) without hypertension, according to blood-pressure category at the baseline examination. Vertical bars indi-
cate 95% confidence intervals. Optimal BP is defined here as a systolic pressure of less than 120 mm Hg and a diastolic pressure of
less than 80 mm Hg. Normal BP is a systolic pressure of 120 to 129 mm Hg or a diastolic pressure of 80 to 84 mm Hg. High-normal
BP is a systolic pressure of 130 to 139 mm Hg or a diastolic pressure of 85 to 89 mm Hg. If the systolic and diastolic pressure read-
ings for a subject were in different categories, the higher of the two categories was used. Source: N Engl J Med 2001;345:1291–1297.
Copyright 2001, Massachusetts Medical Society. All rights reserved.
Chobanian et al
JNC 7 – COMPLETE REPORT
Figure 12. Ten-year risk for CHD by SBP and presence of other
risk factors. Source: Derived from K.M. Anderson, P.W.F. Wil-
son, P.M. Odell, W.B. Kannel. An updated coronary risk profile.
A statement for health professionals. Circulation
1991;83:356 –362.
for individuals with hypertension and no other compelling
89 mm Hg diastolic blood pressure (DBP). This new desig-
conditions is ⬍140/90 mm Hg (see the section Compelling
nation is intended to identify those individuals in whom early
Indications). The goal for individuals with prehypertension
intervention by adoption of healthy lifestyles could reduce
and no compelling indications is to lower BP to normal with
BP, decrease the rate of progression of BP to hypertensive
lifestyle changes and prevent the progressive rise in BP using
levels with age, or prevent hypertension entirely.
the recommended lifestyle modifications (See the section
Another change in classification from JNC 6 is the combining
of stage 2 and stage 3 hypertension into a single stage 2 category.
This revision reflects the fact that the approach to the manage-
Cardiovascular Disease Risk
ment of the former two groups is similar (Table 2).
The relationship between BP and risk of CVD events iscontinuous, consistent, and independent of other risk factors.
Classification of Blood Pressure
The higher the BP, the greater is the chance of heart attack,
Table 3 provides a classification of BP for adults aged 18 and
HF, stroke, and kidney diseases. The presence of each
older. The classification is based on the average of 2 or more
additional risk factor compounds the risk from hypertension,
properly measured, seated BP readings on each of 2 or more
as illustrated in Figure 12.20 The easy and rapid calculation of
office visits.
a Framingham CHD risk score using published tables21 may
Prehypertension is not a disease category. Rather it is a
assist the clinician and patient in demonstrating the benefits
designation chosen to identify individuals at high risk of
of treatment. Management of these other risk factors is
developing hypertension, so that both patients and clinicians
essential and should follow the established guidelines for
are alerted to this risk and encouraged to intervene and
controlling these coexisting problems that contribute to over-
prevent or delay the disease from developing. Individuals
all cardiovascular risk.
who are prehypertensive are not candidates for drug therapyon the basis of their level of BP and should be firmly and
Importance of Systolic Blood Pressure
unambiguously advised to practice lifestyle modification in
Impressive evidence has accumulated to warrant greater
order to reduce their risk of developing hypertension in the
attention to the importance of SBP as a major risk factor for
future (see the section Lifestyle Modifications). Moreover,individuals with prehypertension who also have diabetes orkidney disease should be considered candidates for appropri-ate drug therapy if a trial of lifestyle modification fails toreduce their BP to 130/80 mm Hg or less.
This classification does not stratify hypertensives by the
presence or absence of risk factors or target organ damage inorder to make different treatment recommendations, if eitheror both are present. JNC 7 suggests that all people withhypertension (Stages 1 and 2) be treated. The treatment goal
Classification of Blood Pressure for Adults
BP Classification
Figure 13. Changes in systolic and diastolic blood pressure with
age. SBP and DBP by age and race or ethnicity for men and
Stage 1 hypertension
women over 18 years of age in the US population. Data fromNHANES III, 1988 to 1991. Source: Burt VL et al. Hypertension
Stage 2 hypertension
Figure 14. Difference in CHD prediction between systolic and
diastolic blood pressure as a function of age. The strength of
the relationship as a function of age is indicated by an increase
in the  coefficient. Difference in  coefficients (from Cox
Figure 15. Systolic blood pressure distributions. Source: Whel-
proportional-hazards regression) between SBP and DBP is plot-
ton PK et al. JAMA 2002;288:1884.
ted as function of age, obtaining this regression line:  (SBP)⫺(DBP)⫽1.4948⫹0.0290 ⫻ age (P⫽0.008). A  coefficient level
BP with age could be prevented or diminished, much of
⬍0.0 indicates a stronger effect of DBP on CHD risk, while lev-els ⬎0.0 suggest a greater importance of systolic pressure.
hypertension, cardiovascular and renal disease, and stroke
Source: Circulation 2001;103:1247.
might be prevented. A number of important causal factors forhypertension have been identified, including excess body
CVDs. Changing patterns of BP occur with increasing age.
weight; excess dietary sodium intake; reduced physical ac-
The rise in SBP continues throughout life, in contrast to DBP,
tivity; inadequate intake of fruits, vegetables, and potassium;
which rises until approximately 50 years old, tends to level
and excess alcohol intake.10,32 The prevalence of these char-
off over the next decade, and may remain the same or fall
acteristics is high. One hundred twenty-two million Ameri-
later in life (Figure 13).1,15 Diastolic hypertension predomi-
cans are overweight or obese.33 Mean sodium intake is
nates before 50 years of age, either alone or in combination
approximately 4100 mg per day for men and 2750 mg per day
with SBP elevation. The prevalence of systolic hypertension
for women, 75% of which comes from processed foods.34,35
increases with age, and above the age of 50 years, systolic
Fewer than 20% of Americans engage in regular physical
hypertension represents the most common form of hyperten-
activity,36 and fewer than 25% consume 5 or more servings of
sion. DBP is a more potent cardiovascular risk factor than
fruits and vegetables daily.37
SBP until age 50; thereafter, SBP is more important (Figure
Because the lifetime risk of developing hypertension is
very high (Figure 8), a public health strategy that comple-
Clinical trials have demonstrated that control of isolated
ments the hypertension treatment strategy is warranted. In
systolic hypertension reduces total mortality, cardiovascular
order to prevent BP levels from rising, primary prevention
mortality, stroke, and HF events.23–25 Both observational
measures should be introduced to reduce or minimize these
studies and clinical trial data suggest that poor SBP control is
causal factors in the population, particularly in individuals
largely responsible for the unacceptably low rates of overall
with prehypertension. A population approach that decreases
BP control.26,27 In the Antihypertensive and Lipid-Lowering
the BP level in the general population by even modest
Treatment to Prevent Heart Attack Trial (ALLHAT) andControlled Onset Verapamil Investigation of Cardiovascular
amounts has the potential to substantially reduce morbidity
End Points (CONVINCE) trial, DBP control rates exceeded
and mortality or at least delay the onset of hypertension. For
90%, but SBP control rates were considerably less (60 to
example, it has been estimated that a 5 mm Hg reduction of
70%).28,29 Poor SBP control is at least in part related to
SBP in the population would result in a 14% overall reduction
physician attitudes. A survey of primary care physicians
in mortality due to stroke, a 9% reduction in mortality due to
indicated that three-fourths of them failed to initiate antihy-
CHD, and a 7% decrease in all-cause mortality (Figure
pertensive therapy in older individuals with SBP of 140 to
159 mm Hg, and most primary care physicians did not pursue
Barriers to prevention include cultural norms; insufficient
control to less than 140 mm Hg.30,31 Most physicians have
attention to health education by health care practitioners; lack
been taught that the diastolic pressure is more important than
of reimbursement for health education services; lack of
SBP and thus treat accordingly. Greater emphasis must
access to places to engage in physical activity; larger servings
clearly be placed on managing systolic hypertension. Other-
of food in restaurants; lack of availability of healthy food
wise, as the US population becomes older, the toll of
choices in many schools, worksites, and restaurants; lack of
uncontrolled SBP will cause increased rates of cardiovascular
exercise programs in schools; large amounts of sodium added
and renal diseases.
to foods by the food industry and restaurants; and the highercost of food products that are lower in sodium and calories.10
Prevention of Hypertension: Public
Overcoming the barriers will require a multipronged ap-
proach directed not only to high-risk populations but also to
The prevention and management of hypertension are major
communities, schools, worksites, and the food industry. The
public health challenges for the United States. If the rise in
recent recommendations by the American Public Health
Chobanian et al
JNC 7 – COMPLETE REPORT
Association and the NHBPEP Coordinating Committee that
Recommendations for Follow-Up Based on Initial
the food industry, including manufacturers and restaurants,
Blood Pressure Measurements for Adults Without Acute End
reduce sodium in the food supply by 50% over the next
Organ Damage
decade is the type of approach that, if implemented, would
reduce BP in the population.39,40
Follow-Up Recommended†
Recheck in 2 years
Recheck in 1 year‡
Healthy People 2010 has identified the community as asignificant partner and vital point of intervention for attaining
Stage 1 hypertension
Confirm within 2 months‡
healthy goals and outcomes.41 Partnerships with community
Stage 2 hypertension
Evaluate or refer to source of care within 1 month.
groups such as civic, philanthropic, religious, and senior
For those with higher pressures (eg,⬎180/110 mm Hg), evaluate and treat immediately
citizen organizations provide locally focused orientation to
or within 1 week depending on clinical situation
the health needs of diverse populations. The probability of
and complications.
success increases as interventional strategies more aptly
*If systolic and diastolic categories are different, follow recommendations for
address the diversity of racial, ethnic, cultural, linguistic,
shorter time follow-up (e.g., 160/86 mm Hg should be evaluated or referred to
religious, and social factors in the delivery of medical
source of care within 1 month).
services. Community service organizations can promote the
†Modify the scheduling of follow-up according to reliable information about past
prevention of hypertension by providing culturally sensitive
BP measurements, other cardiovascular risk factors, or target organ disease.
educational messages and lifestyle support services and by
‡Provide advice about lifestyle modifications (see Lifestyle Modifications
establishing cardiovascular risk factor screening and referralprograms. Community-based strategies and programs have
should be avoided for at least 30 minutes prior to measure-
been addressed in prior NHLBI publications and other doc-uments (Facts About the DASH Eating Plan,
ment. Measurement of BP in the standing position is indi-
Lowering High Blood Pressure,43 National High Blood Pres-
cated periodically, especially in those at risk for postural
sure Education Month,44 The Heart Truth: A National Aware-
hypotension, prior to necessary drug dose or adding a drug,
ness Campaign for Women About Heart Disease,45 Mobiliz-
and in those who report symptoms consistent with reduced
ing African American Communities To Address Disparities in
BP on standing. An appropriately sized cuff (cuff bladder
Cardiovascular Health: The Baltimore City Health Partner-
encircling at least 80% of the arm) should be used to ensure
ship Strategy Development Workshop Summary Report,46
accuracy. At least two measurements should be made and the
NHLBI Healthy People 2010 Gateway,47 Cardiovascular
average recorded. For manual determinations, palpated radial
Disease Enhanced Dissemination and Utilization Centers
pulse obliteration pressure should be used to estimate SBP;
[EDUCs] Awardees,48 Hearts N' Parks,49 Healthbeat Radio
the cuff should then be inflated 20 to 30 mm Hg above this
Network,50 Salud para su Corazo´n [For the Health of Your
level for the auscultatory determinations; the cuff deflation
rate for auscultatory readings should be 2 mm Hg per second.
SBP is the point at which the first of two or more Korotkoff
Calibration, Maintenance, and Use of Blood
sounds is heard (onset of phase 1), and the disappearance of
Korotkoff sound (onset of phase 5) is used to define DBP.
The potential of mercury spillage contaminating the environ-
Clinicians should provide to patients, verbally and in writing,
ment has led to the decreased use or elimination of mercury
their specific BP numbers and the BP goal of their treatment.
in sphygmomanometers as well as in thermometers52 How-
Follow-up of patients with various stages of hypertension
ever, concerns regarding the accuracy of nonmercury sphyg-
is recommended as shown in Table 4.
momanometers have created new challenges for accurate BPdetermination.53,54 When mercury sphygmomanometers are
Ambulatory Blood Pressure Monitoring
replaced, the new equipment, including all home BP mea-
Ambulatory blood pressure monitoring (ABPM) provides
surement devices, must be appropriately validated and
information about BP during daily activities and sleep.59 BP
checked regularly for accuracy.55
has a reproducible circadian profile, with higher values whileawake and mentally and physically active, much lower values
Accurate Blood Pressure Measurement in
during rest and sleep, and early morning increases for 3 or
the Office
more hours during the transition of sleep to wakefulness.60
The accurate measurement of BP is the sine qua non for
These devices use either a microphone to measure Korotkoff
successful management. The equipment, whether aneroid,
sounds or a cuff that senses arterial waves using oscillometric
mercury, or electronic, should be regularly inspected and
techniques. Twenty-four-hour BP monitoring provides mul-
validated. The operator should be trained and regularly
tiple readings during all of a patient's activities. While office
retrained in the standardized technique, and the patient must
BP values have been used in the numerous studies that have
be properly prepared and positioned.4,56,57 The auscultatory
established the risks associated with an elevated BP and the
method of BP measurement should be used.58 Persons should
benefits of lowering BP, office measurements have some
be seated quietly for at least 5 minutes in a chair (rather than
shortcomings. For example, a white-coat effect (increase in
on an examination table), with feet on the floor, and arm
BP primarily in the medical care environment) is noted in as
supported at heart level. Caffeine, exercise, and smoking
many as 20 to 35% of patients diagnosed with hypertension.61
Clinical Situations in Which Ambulatory Blood
Cardiovascular Risk Factors
Pressure Monitoring May Be Helpful
Major risk factors
Suspected white-coat hypertension in patients with hypertension and no
target organ damage
Age (older than 55 for men, 65 for women)†
Apparent drug resistance (office resistance)
Diabetes mellitus*
Hypotensive symptoms with antihypertensive medication
Elevated LDL (or total) cholesterol or low HDL cholesterol*
Episodic hypertension
Estimated GFR ⬍60 mL/min
Autonomic dysfunction
Family history of premature cardiovascular disease (men aged ⬍55 orwomen aged ⬍65)
Ambulatory BP values are usually lower than clinic read-
ings. Awake hypertensive individuals have an average BP of
Obesity* (body mass index ⱖ30 kg/m2)
⬎135/85 mm Hg and during sleep, ⬎120/75 mm Hg. The
Physical inactivity
level of BP measurement using ABPM correlates better than
Tobacco usage, particularly cigarettes
office measurements with target organ injury.15 ABPM also
Target organ damage
provides a measure of the percentage of BP readings that areelevated, the overall BP load, and the extent of BP fall during
sleep. In most people, BP drops by 10 to 20% during the night;
Left ventricular hypertrophy
those in whom such reductions are not present appear to be at
Angina/prior myocardial infarction
increased risk for cardiovascular events. In addition, it was
Prior coronary revascularization
reported recently that ABPM patients whose 24-hour BP ex-
ceeded 135/85 mm Hg were nearly twice as likely to have a
cardiovascular event as those with 24-hour mean BPs less than
Stroke or transient ischemic attack
135/85 mm Hg, irrespective of the level of the office BP.62,63
Indications for the use of ABPM are listed in Table 5.
Medicare reimbursement for ABPM is now provided to
Chronic kidney disease
assess patients with suspected white-coat hypertension.
Peripheral arterial disease
GFR indicates glomerular filtration rate.
Self-monitoring of BP at home and work is a practical
*Components of the metabolic syndrome. Reduced HDL and elevated
approach to assess differences between office and out-of-
triglycerides are components of the metabolic syndrome. Abdominal obesity is
office BP prior to consideration of ambulatory monitoring.
also a component of metabolic syndrome.
For those whose out-of-office BPs are consistently ⬍130/
†Increased risk begins at approximately 55 and 65 for men and women,
respectively. Adult Treatment Panel III used earlier age cutpoints to suggest the
80 mm Hg despite an elevated office BP and who lack
need for earlier action.
evidence of target organ disease, 24-hour monitoring or drugtherapy can be avoided.
Self-measurement or ambulatory monitoring may be par-
extremities for edema and pulses; and neurological
ticularly helpful in assessing BP in smokers. Smoking raises
BP acutely, and the level returns to baseline in about 15
Data from epidemiological studies and clinical trials have
minutes after stopping.
demonstrated that elevations in resting heart rate and reducedheart rate variability are associated with higher cardiovascu-
lar risk. In the Framingham Heart Study, an average resting
Evaluation of hypertensive patients has three objectives: (1)
heart rate of 83 beats per minute was associated with a
to assess lifestyle and identify other cardiovascular risk
substantially higher risk of death from a CV event than those
factors or concomitant disorders that may affect prognosisand guide treatment (Table 6); (2) to reveal identifiable
Identifiable Causes of Hypertension
causes of high BP (Table 7); and (3) to assess the presence or
Chronic kidney disease
absence of target organ damage and CVD.
Patient evaluation is made through medical history, phys-
Coarctation of the aorta
ical examination, routine laboratory tests, and other diagnos-
Cushing syndrome and other glucocorticoid excess states including chronic
tic procedures. The physical examination should include an
appropriate measurement of BP, with verification in the
Drug-induced or drug-related (see Table 18)
contralateral arm; examination of the optic fundi; calculation
Obstructive uropathy
of body mass index (BMI) (measurement of waist circumfer-
ence is also very useful); auscultation for carotid, abdominal,
Primary aldosteronism and other mineralocorticoid excess states
and femoral bruits; palpation of the thyroid gland; thorough
examination of the heart and lungs; examination of the
abdomen for enlarged kidneys, masses, distended urinary
Thyroid or parathyroid disease
bladder, and abnormal aortic pulsation; palpation of the lower
Chobanian et al
JNC 7 – COMPLETE REPORT
Screening Tests for Identifiable Hypertension
Chronic kidney disease
Coarctation of the aorta
Cushing syndrome and other glucocorticoid
History/dexamethasone suppression test
excess states including chronic steroid therapy
Drug-induced/related (see Table 18)
History; drug screening
24-hour urinary metanephrine and normetanephrine
Primary aldosteronism and other
24-hour urinary aldosterone level or specific
mineralocorticoid excess states
measurements of other mineralocorticoids
Doppler flow study; magnetic resonance angiography
Sleep study with O2 saturation
GFR indicates glomerular filtration rate; CT, computed tomography; TSH, thyroid stimulating hormone; PTH,
at lower heart rate levels.64 Moreover, reduced heart rate
be considered in some individuals, particularly those with
variability was also associated with an increase in CV
CVD but without other risk factor abnormalities. Results of
mortality.65 No clinical trials have prospectively evaluated the
an analysis of the Framingham Heart Study cohort demon-
impact of reducing heart rate on CV outcomes.
strated that those with an LDL value within the rangeassociated with low CV risk, who also had an elevated
Laboratory Tests and Other
HS-CRP value, had a higher CV event rate as compared with
those with low CRP and high LDL-C.73 Other studies also
Routine laboratory tests recommended before initiating ther-
have shown that elevated CRP is associated with a higher CV
apy include a 12-lead ECG; urinalysis; blood glucose and
event rate, especially in women.74 Elevations in homocys-
hematocrit; serum potassium, creatinine (or the correspond-
teine have also been described as associated with higher CV
ing estimated glomerular filtration rate [eGFR]), and calci-
risk; however, the results with this marker are not as robust as
um66; and a lipoprotein profile (after 9- to 12-hour fast) that
those with high HS-CRP.75,76
includes HDL and LDL cholesterol (HDL-C and LDL-C) andtriglycerides (TGs). Optional tests include measurement of
Identifiable Causes of Hypertension
urinary albumin excretion or albumin/creatinine ratio (ACR),
Additional diagnostic procedures may be indicated to identify
except for those with diabetes or kidney disease, for whom
causes of hypertension, particularly in patients whose (1) age,
annual measurements should be made. More extensive testing
history, physical examination, severity of hypertension, or
for identifiable causes is not indicated generally unless BP
initial laboratory findings suggest such causes; (2) BP re-
control is not achieved or the clinical and routine laboratory
sponds poorly to drug therapy; (3) BP begins to increase for
evaluation strongly suggests an identifiable secondary cause
uncertain reason after being well controlled; and (4) onset of
(ie, vascular bruits, symptoms of catecholamine excess,
hypertension is sudden. Screening tests for particular forms of
unprovoked hypokalemia). See the section Identifiable
identifiable hypertension are shown in Table 8.
Causes of Hypertension for a more thorough discussion.
Pheochromocytoma should be suspected in patients with
The presence of decreased GFR or albuminuria has prog-
labile hypertension or with paroxysms of hypertension ac-
nostic implications as well. Studies reveal a strong relation-
companied by headache, palpitations, pallor, and perspira-
ship between decreases in GFR and increases in cardiovas-
tion.77 Decreased pressure in the lower extremities or delayed
cular morbidity and mortality.67,68 Even small decreases in
or absent femoral arterial pulses may indicate aortic coarcta-
GFR increase cardiovascular risk.67 Serum creatinine may
tion; truncal obesity, glucose intolerance, and purple striae
overestimate glomerular filtration. The optimal tests to deter-
suggest Cushing syndrome. Examples of clues from the
mine GFR are debated, but calculating GFR from the recent
laboratory tests include unprovoked hypokalemia (primary
modifications of the Cockcroft and Gault equations is
aldosteronism), hypercalcemia (hyperparathyroidism), and
elevated creatinine or abnormal urinalysis (renal parenchymal
The presence of albuminuria, including microalbuminuria,
disease). Appropriate investigations should be conducted
even in the setting of normal GFR, is also associated with an
when there is a high index of suspicion of an identifiable
increase in cardiovascular risk.70–72 Urinary albumin excre-
tion should be quantitated and monitored on an annual basis
The most common parenchymal kidney diseases associated
in high-risk groups, such as those with diabetes or renal
with hypertension are chronic glomerulonephritis, polycystic
kidney disease, and hypertensive nephrosclerosis. These can
Additionally, three emerging risk factors—(1) high-
generally be distinguished by the clinical setting and addi-
sensitivity C-reactive protein (HS-CRP), a marker of inflam-
tional testing. For example, a renal ultrasound is useful in
mation; (2) homocysteine; and (3) elevated heart rate—may
diagnosing polycystic kidney disease. Renal artery stenosis
and subsequent renovascular hypertension should be sus-
drug doses, or appropriate drug combinations may result in
pected in a number of circumstances, including (1) onset of
inadequate BP control.
hypertension before 30 years of age, especially in the absenceof family history, or onset of significant hypertension after
Goals of Therapy
age 55; (2) an abdominal bruit, especially if a diastolic
The ultimate public health goal of antihypertensive therapy is
component is present; (3) accelerated hypertension; (4) hy-
to reduce cardiovascular and renal morbidity and mortality.
pertension that had been easy to control but is now resistant;
Since most persons with hypertension, especially those ⬎50
(5) recurrent flash pulmonary edema; (6) renal failure of
years old, will reach the DBP goal once the SBP goal is
uncertain etiology, especially in the absence of proteinuria or
achieved, the primary focus should be on attaining the SBP
an abnormal urine sediment; and (7) acute renal failure
goal. Treating SBP and DBP to targets that are ⬍140/
precipitated by therapy with an angiotensin-converting en-
90 mm Hg is associated with a decrease in CVD complica-tions.87 In patients with hypertension and diabetes or renal
zyme inhibitor (ACEI) or angiotensin receptor blocker (ARB)
disease, the BP goal is ⬍130/80 mm Hg.88,89
under conditions of occult bilateral renal artery stenosis ormoderate to severe volume depletion.
Benefits of Lowering Blood Pressure
In patients with suspected renovascular hypertension, non-
In clinical trials, antihypertensive therapy has been associated
invasive screening tests include the ACEI-enhanced renal
with reductions in stroke incidence averaging 35% to 40%;
scan, duplex Doppler flow studies, and magnetic resonance
myocardial infarction, 20% to 25%; and HF, ⬎50%.90 It is
angiography. While renal artery angiography remains the
estimated that in patients with stage 1 hypertension (SBP 140
gold standard for identifying the anatomy of the renal artery,
to 159 mm Hg and/or DBP 90 to 99 mm Hg) and additional
it is not recommended for diagnosis alone because of the risk
cardiovascular risk factors, achieving a sustained 12 mm Hg
associated with the procedure. At the time of intervention, an
reduction in SBP over 10 years will prevent 1 death for every
arteriogram will be performed using limited contrast to
11 patients treated. In the added presence of CVD or target
confirm the stenosis and identify the anatomy of the renal
organ damage, only 9 patients would require such BP
reduction to prevent 1 death.91
Genetics of Hypertension
The investigation of rare genetic disorders affecting BP has
Adoption of healthy lifestyles by all persons is critical for the
led to the identification of genetic abnormalities associated
prevention of high BP and is an indispensable part of the
with several rare forms of hypertension, including
management of those with hypertension.10 Weight loss of as
little as 10 lbs (4.5 kg) reduces BP and/or prevents hyperten-
hydroxylase and 17␣-hydroxylase deficiencies, Liddle syn-
sion in a large proportion of overweight persons, although the
drome, the syndrome of apparent mineralocorticoid excess,
ideal is to maintain normal body weight.92,93 BP is also
and pseudohypoaldosteronism type II.82 The individual and
benefited by adoption of the Dietary Approaches to Stop
joint contributions of these genetic mutations to BP levels in
Hypertension (DASH) eating plan,94 which is a diet rich in
the general population, however, are very small. Genetic
fruits, vegetables, and lowfat dairy products with a reduced
association studies have identified polymorphisms in several
content of dietary cholesterol as well as saturated and total fat
candidate genes (eg, angiotensinogen, ␣-adducin, - and
(modification of whole diet). It is rich in potassium and
DA-adrenergic receptors, -3 subunit of G proteins), and
calcium content.95 Dietary sodium should be reduced to no
genetic linkage studies have focused attention on several
more than 100 mmol per day (2.4 g of sodium).94–96 Everyone
genomic sites that may harbor other genes contributing to
who is able should engage in regular aerobic physical activity
primary hypertension.83–85 However, none of these various
such as brisk walking at least 30 minutes per day most days
genetic abnormalities has been shown, either alone or in joint
of the week.97,98 Alcohol intake should be limited to no more
combination, to be responsible for any applicable portion of
than 1 oz (30 mL) of ethanol, the equivalent of two drinks, per
hypertension in the general population.
day in most men and no more than 0.5 oz of ethanol (onedrink) per day in women and lighter weight persons. A drink
is 12 oz of beer, 5 oz of wine, and 1.5 oz of 80-proof liquor(Table 9).99 Lifestyle modifications reduce BP, prevent or
Blood Pressure Control Rates
delay the incidence of hypertension, enhance antihyperten-
Hypertension is the most common primary diagnosis in
sive drug efficacy, and decrease cardiovascular risk. For
America (35 million office visits as the primary diagnosis).5
example, in some individuals, a 1600 mg sodium DASH
Current control rates (SBP ⬍140 mm Hg and DBP
eating plan has BP effects similar to single drug therapy.94
⬍90 mm Hg), though improved, are still far below the
Combinations of 2 (or more) lifestyle modifications can
Healthy People goal of 50% (originally set as the year 2000
achieve even better results.100 For overall cardiovascular risk
goal and since extended to 2010; Table 1). In the majority of
reduction, patients should be strongly counseled to quit
patients, reducing SBP has been considerably more difficult
than lowering DBP. Although effective BP control can beachieved in most patients who are hypertensive, the majority
will require 2 or more antihypertensive drugs.28,29,86 Failure to
A large number of drugs are currently available for reducing
prescribe lifestyle modifications, adequate antihypertensive
BP. Tables 10 and 11 provide a list of the commonly used
Chobanian et al
JNC 7 – COMPLETE REPORT
Lifestyle Modifications To Prevent and Manage Hypertension*
Approximate SBP Reduction
Maintain normal body weight (body
5–20 mm Hg/10 kg92,93
mass index 18.5–24.9 kg/m2).
Adopt DASH eating plan
Consume a diet rich in fruits,
8–14 mm Hg94,95
vegetables, and low-fat dairyproducts with a reduced content ofsaturated and total fat.
Dietary sodium reduction
Reduce dietary sodium intake to no
2–8 mm Hg94–96
more than 100 mmol per day (2.4 gsodium or 6 g sodium chloride).
Physical activity
Engage in regular aerobic physical
activity such as brisk walking (atleast 30 minutes per day, most daysof the week).
Moderation of alcohol
Limit consumption to no more than 2
drinks (eg, 24 oz beer, 10 oz wine,or 3 oz 80-proof whiskey) per day inmost men and to no more than 1drink per day in women and lighter-weight persons.
DASH indicates Dietary Approaches to Stop Hypertension.
*For overall cardiovascular risk reduction, stop smoking.
†The effects of implementing these modifications are dose- and time-dependent and could be
greater for some individuals.
antihypertensive agents and their usual dose range and
disease (EUROPA), in which the ACEI perindopril was
frequency of administration.
added to existent therapy in patients with stable coronary
More than two-thirds of hypertensive individuals cannot
disease and without HF, also demonstrated reduction in CVD
be controlled on one drug and will require two or more
events with ACEIs.114
antihypertensive agents selected from different drug class-
Since 1998, several large trials comparing newer classes of
es.28,87,101–103 For example, in ALLHAT, 60% of those
agents, including CCBs, ACEIs, an ␣1 receptor blocker, and
whose BP was controlled to ⬍140/90 mm Hg received two
an ARB, with the older diuretics and/or BBs have been
or more agents, and only 30% overall were controlled on
completed.101,102,109,112,115–118 Most of these studies showed
one drug.28 In hypertensive patients with lower BP goals or
the newer classes were neither superior nor inferior to the
with substantially elevated BP, 3 or more antihypertensive
older ones. One exception was the Losartan Intervention for
drugs may be required.
Endpoint Reduction in Hypertension (LIFE) study, in which
Since the first VA Cooperative trial published in 1967,
CVD events were 13% lower (because of differences in
thiazide-type diuretics have been the basis of antihyperten-
stroke but not CHD rates) with the ARB losartan than with
sive therapy in the majority of placebo-controlled outcome
the BB atenolol.102 There has not been a large outcome trial
trials in which CVD events, including strokes, CHD, and HF,
completed as yet comparing an ARB with a diuretic. All of
have been reduced by BP lowering.104–108 However, there are
these trials taken together suggest broadly similar cardiovas-
also excellent clinical trial data proving that lowering BP with
cular protection from BP-lowering with ACEIs, CCBs, and
other classes of drugs, including ACEIs, ARBs, -blockers
ARBs, as with thiazide-type diuretics and BBs, although
(BBs), and calcium channel blockers (CCBs), also reduces
some specific outcomes may differ between the classes.
the complications of hypertension.90,101,102,107,109–112 Several
There do not appear to be systematic outcome differences
randomized controlled trials have demonstrated reduction in
between dihydropyridine and nondihydropyridine CCBs in
CVD with BBs, but the benefits are less consistent than with
hypertension morbidity trials. On the basis of other data,
diuretics.107,108 The European Trial on Systolic Hypertension
short-acting CCBs are not recommended in the management
in the Elderly (Syst-EUR) study showed significant reduc-
of hypertension.
tions in stroke and all CVD with the dihydropyridine CCB,nitrendipine, compared with placebo.113 The Heart Outcomes
Rationale for Recommendation of Thiazide-Type Diuretics
Prevention Evaluation (HOPE) trial, which was not restricted
as Preferred Initial Agent
to hypertensive individuals but which included a sizable
In trials comparing diuretics with other classes of antihyper-
hypertensive subgroup, showed reductions in a variety of
tensive agents, diuretics have been virtually unsurpassed in
CVD events with the ACEI ramipril compared with placebo
preventing the cardiovascular complications of hypertension.
in individuals with prior CVD or diabetes mellitus combined
In the ALLHAT study, which involved more than 40 000
with other risk factor(s).110 The European trial on reduction of
hypertensive individuals,109 there were no differences in the
cardiac events with perindopril in stable coronary artery
primary CHD outcome or mortality between the thiazide-type
TABLE 10.
Oral Antihypertensive Drugs
Usual Dose Range,
Drug (Trade Name)
Thiazide diuretics
Chlorothiazide (Diuril)
Chlorthalidone (generic)
Hydrochlorothiazide (Microzide, HydroDIURIL†)
Polythiazide (Renese)
Indapamide (Lozol†)
Metolazone (Mykrox)
Metolazone (Zaroxolyn)
Bumetanide (Bumex†)
Furosemide (Lasix†)
Torsemide (Demadex†)
Amiloride (Midamor†)
Triamterene (Dyrenium)
Aldosterone receptor blockers
Eplerenone (Inspra)
Atenolol (Tenormin†)
Betaxolol (Kerlone†)
Bisoprolol (Zebeta†)
Metoprolol extended release (Toprol XL)
Nadolol (Corgard†)
Propranolol (Inderal†)
Propranolol long-acting (Inderal LA†)
Timolol (Blocadren†)
BBs with intrinsic sympathomimetic activity
Acebutolol (Sectral†)
Penbutolol (Levatol)
Pindolol (generic)
Combined ␣-blockers and BBs
Carvedilol (Coreg)
Labetalol (Normodyne, Trandate†)
Benazepril (Lotensin†)
Captopril (Capoten†)
Enalapril (Vasotec†)
Fosinopril (Monopril)
Lisinopril (Prinivil, Zestril†)
Moexipril (Univasc)
Perindopril (Aceon)
Quinapril (Accupril)
Ramipril (Altace)
Trandolapril (Mavik)
Angiotensin II antagonists
Candesartan (Atacand)
Eprosartan (Teveten)
Irbesartan (Avapro)
Losartan (Cozaar)
Olmesartan (Benicar)
Telmisartan (Micardis)
Valsartan (Diovan)
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 10.
Oral Antihypertensive Drugs (continued)
Usual Dose Range,
Drug (Trade Name)
Diltiazem extended release (Cardizem CD,
Dilacor XR, Tiazac†)
Diltiazem extended release (Cardizem LA)
Verapamil immediate release (Calan, Isoptin†)
Verapamil long acting (Calan SR, Isoptin SR†)
Verapamil (Coer, Covera HS, Verelan PM)
Amlodipine (Norvasc)
Felodipine (Plendil)
Isradipine (Dynacirc CR)
Nicardipine sustained release (Cardene SR)
Nifedipine long-acting (Adalat CC, Procardia
Nisoldipine (Sular)
Doxazosin (Cardura)
Prazosin (Minipress†)
Terazosin (Hytrin)
Central ␣2 agonists and othercentrally acting drugs
Clonidine (Catapres†)
Clonidine patch (Catapres-TTS)
Methyldopa (Aldomet†)
Reserpine (generic)
Guanfacine (Tenex†)
Direct vasodilators
Minoxidil (Loniten†)
Source: Physicians' Desk Reference. 57th ed. Montvale, NJ: Thomson PDR; 2003.
*In some patients treated once daily, the antihypertensive effect may diminish toward the end of the dosing interval (trough effect). BP should be measured just
prior to dosing to determine if satisfactory BP control is obtained. Accordingly, an increase in dosage or frequency may need to be considered. These dosages mayvary from those listed in the Physician's Desk Reference, 57th ed.
†Available now or soon to become available in generic preparations.
diuretic chlorthalidone, the ACEI lisinopril, or the CCB
were generally the equivalent of 25 to 50 mg of hydrochlo-
amlodipine. Stroke incidence was greater with lisinopril than
rothiazide or 12.5 to 25 mg of chlorthalidone, although
chlorthalidone therapy, but these differences were present
therapy may be initiated at lower doses and titrated to these
primarily in blacks, who also had less BP lowering with
doses if tolerated. Higher doses have been shown to add
lisinopril than diuretics. The incidence of HF was greater in
little additional antihypertensive efficacy but are associ-
CCB-treated and ACEI-treated individuals compared with
ated with more hypokalemia and other adverse
those receiving the diuretic in both blacks and whites. In the
effects.119 –122
Second Australian National Blood Pressure (ANBP2) study,
Uric acid will increase in many patients receiving a
which compared the effects of an ACEI-based regimen
diuretic, but the occurrence of gout is uncommon with
against diuretics-based therapy in 6000 white hypertensive
dosages ⱕ50 mg/d of hydrochlorothiazide or ⱕ25 mg of
individuals, cardiovascular outcomes were less in the ACEI
chlorthalidone. Some reports have described an increased
group, with the favorable effect apparent only in men.112
degree of sexual dysfunction when thiazide diuretics, partic-
CVD outcome data comparing ARB with other agents are
ularly at high doses, are used. In the Treatment of Mild
Hypertension Study (TOMHS), participants randomized to
Clinical trial data indicate that diuretics are generally
chlorthalidone reported a significantly higher incidence of
well tolerated.103,109 The doses of thiazide-type diuretics
erection problems through 24 months of the study; however,
used in successful morbidity trials of low-dose diuretics
the incidence rate at 48 months was similar to placebo.123 The
TABLE 11.
Combination Drugs for Hypertension
Fixed-Dose Combination, mg*
Amlodipine-benazepril hydrochloride (2.5/10, 5/10, 5/20, 10/20)
Trandolapril-verapamil (2/180, 1/240, 2/240, 4/240)
ACEIs and diuretics
Benazepril-hydrochlorothiazide (5/6.25, 10/12.5, 20/12.5, 20/25)
Captopril-hydrochlorothiazide (25/15, 25/25, 50/15, 50/25)
Enalapril-hydrochlorothiazide (5/12.5, 10/25)
Fosinopril-hydrochlorothiazide (10/12.5, 20/12.5)
Lisinopril-hydrochlorothiazide (10/12.5, 20/12.5, 20/25)
Prinzide, Zestoretic
Moexipril-hydrochlorothiazide (7.5/12.5, 15/25)
Quinapril-hydrochlorothiazide (10/12.5, 20/12.5, 20/25)
ARBs and diuretics
Eprosartan-hydrochlorothiazide (600/12.5, 600/25)
Losartan-hydrochlorothiazide (50/12.5, 100/25)
Olmesartan medoxomil-hydrochlorothiazide (20/12.5, 40/12.5, 40/25)
Valsartan-hydrochlorothiazide (80/12.5, 160/12.5, 160/25)
BBs and diuretics
Atenolol-chlorthalidone (50/25, 100/25)
Bisoprolol-hydrochlorothiazide (2.5/6.25, 5/6.25, 10/6.25)
Metoprolol-hydrochlorothiazide (50/25, 100/25)
Nadolol-bendroflumethiazide (40/5, 80/5)
Propranolol LA-hydrochlorothiazide (40/25, 80/25)
Centrally acting drug and diuretic
Methyldopa-hydrochlorothiazide (250/15, 250/25, 500/30, 500/50)
Reserpine-chlorthalidone (0.125/25, 0.25/50)
Reserpine-chlorothiazide (0.125/250, 0.25/500)
Diuretic and diuretic
Spironolactone-hydrochlorothiazide (25/25, 50/50)
Triamterene-hydrochlorothiazide (37.5/25, 75/50)
BB indicates -blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker.
*Some drug combinations are available in multiple fixed doses. Each drug dose is reported in milligrams.
VA Cooperative study did not document a significant differ-
not shown an increase in serum cholesterol in diuretic-
ence in the occurrence of sexual dysfunction using diuretics
treated patients.124,125 In ALLHAT, serum cholesterol did
compared with other antihypertensive medications103 (see the
not increase from baseline in any group, but it was 1.6
section Erectile Dysfunction). Adverse metabolic effects
mg/dL lower in the CCB group and 2.2 mg/dL lower in the
may occur with diuretics. In ALLHAT, diabetes incidence
ACEI group than in diuretic-treated patients.109 Thiazide-
after 4 years of therapy was 11.8% with chlorthalidone
induced hypokalemia could contribute to increased ven-
therapy, 9.6% with amlodipine, and 8.1% with lisinopril.
tricular ectopy and possible sudden death, particularly with
However, those differences did not translate to fewer CV
high doses of thiazides in the absence of a potassium-
events for the ACEI or CCB groups.109 Those who were
sparing agent.121 In the Systolic Hypertension in the
already diabetic had fewer CV events in the diuretic group
Elderly Program (SHEP) trial, the positive benefits of
than with ACEI treatment. Trials longer than 1 year
diuretic therapy were not apparent when serum potassium
duration using modest doses of diuretics generally have
levels were below 3.5 mmol/L.126 However, other studies
Chobanian et al
JNC 7 – COMPLETE REPORT
have become available in generic form, their cost has beenreduced. Despite the various benefits of diuretics, they remainunderutilized.128
Achieving Blood Pressure Control in
Individual Patients
The algorithm for the treatment of hypertensive patients is
shown in Figure 16. Therapy begins with lifestyle modifica-
tion, and if the BP goal is not achieved, thiazide-type
diuretics should be used as initial therapy for most patients,
either alone or in combination with one of the other classes
(ACEIs, ARBs, BBs, CCBs) that have also been shown to
reduce one or more hypertensive complications in random-
ized controlled outcome trials. Selection of one of these other
agents as initial therapy is recommended when a diuretic
cannot be used or when a compelling indication is present
that requires the use of a specific drug, as listed in Table 12.
If the initial drug selected is not tolerated or is contraindi-
cated, then a drug from one of the other classes proven to
reduce cardiovascular events should be substituted.
Since most hypertensive patients will require 2 or more
antihypertensive medications to achieve their BP goals,addition of a second drug from a different class should beinitiated when use of a single agent in adequate doses fails toachieve the goal. When BP is more than 20 mm Hg abovesystolic goal or 10 mm Hg above diastolic goal, considerationshould be given to initiate therapy with 2 drugs, either as
Figure 16. Algorithm for treatment of hypertension.
separate prescriptions or in fixed-dose combinations (Figure16).129
have not demonstrated increased ventricular ectopy as a
The initiation of therapy with more than one drug increases
result of diuretic therapy.127 Despite potential adverse
the likelihood of achieving BP goal in a more timely fashion.
metabolic effects of diuretics, with laboratory monitoring,
The use of multidrug combinations often produces greater BP
thiazide-type diuretics are effective and relatively safe for
reduction at lower doses of the component agents, resulting in
the management of hypertension.
fewer side effects.129,130
Thiazide diuretics are less expensive than other antihyper-
The use of fixed-dose combinations may be more conve-
tensive drugs, although as members of other classes of drugs
nient and simplify the treatment regimen and may cost less
TABLE 12.
Clinical Trial and Guideline Basis for Compelling Indications for Individual Drug Classes
Recommended Drugs
Compelling Indication*
Clinical Trial Basis†
ACC/AHA Heart Failure Guideline,132MERIT-HF,133 COPERNICUS,134 CIBIS,135SOLVD,136 AIRE,137 TRACE,138 ValHEFT,139RALES,140 CHARM141
ACC/AHA Post-MI Guideline,142 BHAT,143SAVE,144 Capricorn,145 EPHESUS146
High coronary disease risk
ALLHAT,109 HOPE,110 ANBP2,112 LIFE,102CONVINCE,101 EUROPA,114 INVEST147
NKF-ADA Guideline,88,89 UKPDS,148ALLHAT109
Chronic kidney disease
NKF Guideline,89 Captopril Trial,149RENAAL,150 IDNT,151 REIN,152 AASK153
Recurrent stroke prevention
BB indicates -blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; Aldo ANT, aldosterone
*Compelling indications for antihypertensive drugs are based on benefits from outcome studies or existing clinical guidelines; the compelling indication is managed
in parallel with the BP.
†Conditions for which clinical trials demonstrate benefit of specific classes of antihypertensive drugs used as part of an antihypertensive regimen to achieve BP
goal to test outcomes.
than the individual components prescribed separately. Use of
Ischemic Heart Disease
generic drugs should be considered to reduce prescription
Hypertensive patients are at increased risk for myocardial
costs, and the cost of separate prescription of multiple drugs
infarction (MI) or other major coronary event and may be at
available generically may be less than nongeneric, fixed-dose
higher risk of death following an acute MI. Myocardial
combinations. The starting dose of most fixed-dose combi-
oxygen supply in hypertensives may be limited by coronary
nations is usually below the doses used in clinical outcome
artery disease (CAD) while myocardial oxygen demand is
trials, and the doses of these agents should be titrated upward
often greater because of the increased impedance to left
to achieve the BP goal before adding other drugs. However,
ventricular ejection and the frequent presence of left ventric-
caution is advised in initiating therapy with multiple agents,
ular hypertrophy (LVH).154 Lowering both SBP and DBP
particularly in some older persons and in those at risk for
reduces ischemia and prevents CVD events in patients with
orthostatic hypotension, such as diabetics with autonomic
CAD, in part by reducing myocardial oxygen demand. One
caveat with respect to antihypertensive treatment in patientswith CAD is the finding in some studies of an apparent
Follow-Up and Monitoring
increase in coronary risk at low levels of DBP. For example,
Once antihypertensive drug therapy is initiated, most patients
in the SHEP study, lowering DBP to ⬍55 or 60 mm Hg was
should return for follow-up and adjustment of medications at
associated with an increase in cardiovascular events, includ-
monthly intervals or less until the BP goal is reached. More
ing MI.155 No similar increase in coronary events (a J-shaped
frequent visits will be necessary for patients with stage 2
curve) has been observed with SBP. Patients with occlusive
hypertension or with complicating comorbid conditions. Se-
CAD and/or LVH are put at risk of coronary events if DBP is
rum potassium and creatinine should be monitored at least 1
low. Overall, however, many more events are prevented than
to 2 times/year. After BP is at goal and stable, follow-up visits
caused if BP is aggressively treated.
can usually be at 3- to 6-month intervals. Comorbidities such
Stable Angina and Silent Ischemia
as HF, associated diseases such as diabetes, and the need for
Therapy is directed toward preventing MI and death and
laboratory tests influence the frequency of visits. Other
reducing symptoms of angina and the occurrence of ischemia.
cardiovascular risk factors should be monitored and treated to
Unless contraindicated, pharmacological therapy should be
their respective goals, and tobacco avoidance must be pro-
initiated with a BB.142,156 BBs will lower BP, reduce symp-
moted vigorously. Low-dose aspirin therapy should be con-
toms of angina, improve mortality, and reduce cardiac output,
sidered only when BP is controlled because of the increased
heart rate, and AV conduction. The reduced inotropy and
risk of hemorrhagic stroke when the hypertension is not
heart rate decrease myocardial oxygen demand. Treatment
should also include smoking cessation, management of dia-betes, lipid lowering, antiplatelet agents, exercise training,
Special Situations in
and weight reduction in obese patients.
If angina and BP are not controlled by BB therapy alone, or
if BBs are contraindicated, as in the presence of severe
Hypertension may exist in association with other conditions
reactive airway disease, severe peripheral arterial disease,
in which there are compelling indications for use of a
high-degree AV block, or the sick sinus syndrome, either
particular treatment based on clinical trial data demonstrating
long-acting, dihydropyridine or nondihydropyridine-type
benefits of such therapy on the natural history of the associ-
CCBs may be used. CCBs decrease total peripheral resis-
ated condition (Table 12). Compelling indications for specific
tance, which leads to reduction in BP and in wall tension.
therapy involve high-risk conditions that can be direct se-
CCBs also decrease coronary resistance and enhance postste-
quelae of hypertension (HF, ischemic heart disease, chronic
notic coronary perfusion. Nondihydropyridine CCBs also can
kidney disease, recurrent stroke) or commonly associated
decrease heart rate, but when in combination with a BB, they
with hypertension (diabetes, high coronary disease risk).
may cause severe bradycardia or high degrees of heart block.
Therapeutic decisions in such individuals should be directed
Therefore, long-acting dihydropyridine CCBs are preferred
at both the compelling indication and BP lowering.
for combination therapy with BBs. If angina or BP is still notcontrolled on this two-drug regimen, nitrates can be added,
The absence of a positive indication can signify a lack of
but these should be used with caution in patients taking
information for a particular drug class. For example, in
phosphodiesterase-5 inhibitors such as sildenafil. Short-
recurrent stroke, there is no study employing CCBs or ARBs.
acting dihydropyridine CCBs should not be used because of
Different stages of the conditions may dictate different
their potential to increase mortality, particularly in the setting
strategies. In HF management, thiazide-type diuretics are
of acute MI.
recommended for reducing the incidence of HF but not inlengthening survival in individuals who already have the
condition. Furthermore, widespread use of combination ther-
The HF syndrome occurs when the heart is incapable of
apy in clinical trials confounds interpretation of the effects of
maintaining sufficient flow to accommodate tissue perfusion
single drugs. In the Perindopril Protection Against Recurrent
and metabolic requirements. Forty to 50% of patients with
Stroke Study (PROGRESS) trial, recurrent stroke rate was
symptoms of HF may have preserved systolic function. These
reduced only when a thiazide-type diuretic was added to
patients are more likely to have hypertension, LVH, and
ACEI background therapy.
isolated diastolic dysfunction and are more likely to be
Chobanian et al
JNC 7 – COMPLETE REPORT
women.141,157 A variety of neurohormonal systems, especially
tality by 34%.140 In the Eplerenone Post-Acute Myocardial
the renin-angiotensin-aldosterone and sympathetic nervous
Infarction Heart Failure Efficacy and Survival Study (EPHE-
systems may be activated in response to the LV dysfunction,
SUS), eplerenone reduced mortality by 15% in patients
but such activation may lead to abnormal ventricular remod-
following a recent MI with LVEF ⱕ40%, 90% of whom had
eling, further LV enlargement, and reduced cardiac contrac-
HF symptoms.140 Hyperkalemia is a risk with aldosterone
tility. The inexorable progression to more severe stages of LV
antagonists, even at low doses (especially since most patients
dysfunction can be significantly reduced by effective therapy
also are taking ACEIs or ARBs), but its incidence can be
with ACEIs, BBs, and diuretics.
reduced by limiting therapy to patients with serum creatinine
Hypertension precedes the development of HF in approx-
⬍2.5 mg/dL and monitoring serum potassium carefully.
imately 90% of patients and increases risk for HF by 2- to
BP targets in HF have not been firmly established, but
3-fold. Hypertension is especially important in HF affecting
lowering SBP is almost uniformly beneficial. In most suc-
African Americans and the elderly. CAD is the cause of HF
cessful trials, systolic blood pressures were lowered to the
in approximately two-thirds of HF patients in the United
range of 110 to 130 mm Hg. One trial demonstrated benefits
States. The true incidence of HF has been unchanged in men
of -blockade in patients with SBP ⬎85 mm Hg,134 suggest-
and has declined among women during the past 50 years.158
ing that very low BPs (eg, SBP ⬍100 mm Hg) may be
However, HF hospitalization rates have more than doubled in
desirable in some HF patients.
the past 20 years159 because of the improved therapy resulting
Digoxin continues to be used in HF despite inconsistent
in increased life expectancy. HF will probably become even
clinical results. In the Digitalis Investigation Group (DIG)
more prevalent in the future as our population ages.
trial, it did not reduce mortality in NYHA class II–III patients
Optimal therapy for HF may require the use of specialized
taking ACEIs and diuretics but did reduce HF symptoms and
HF disease management programs and utilization of a variety
of health professionals to reinforce treatment recommenda-tions. American College of Cardiology/American Heart As-
Diabetes and Hypertension
sociation (ACC/AHA) guidelines are available to manage
The combined unadjusted prevalence of total diabetes and
HF.132 In the stage A group (New York Heart Association
impaired fasting glucose in those over 20 years old is 14.4%
[NYHA] class I), those at high risk for HF but no demon-
and is the leading cause of blindness, ESRD, and nontrau-
strable clinical symptoms or LV dysfunction, treatment
matic amputations.161–165 Type 2 diabetes constitutes over
should include fastidious risk factor management to control
90% of diabetes in the United States and is associated with a
BP, hypercholesterolemia, and hyperglycemia. ACEIs may
70% to 80% chance of premature death from CVD and
be appropriate because of their beneficial effects on mortality
stroke.166–170 The concordance of hypertension and diabetes
in patients at high risk for CVD.110,114 The ALLHAT study
is increased in the population; hypertension is disproportion-
also has suggested that thiazide-diuretic therapy is useful in
ately higher in diabetics,171 while persons with elevated BP
preventing disease progression.109 In stage B HF (NYHA
are 2.5 times more likely to develop diabetes within 5
class I) as defined by the presence of reduced LV function
years.172,173 The common absence of normal nocturnal "dip-
(ejection fraction [EF] ⱕ40%) in otherwise asymptomatic
ping" of BP in diabetics is linked to other CVD surrogates
individuals, ACEIs and BBs are recommended. Stage C
such as LVH and microalbuminuria.171
patients (NYHA class II–III) manifest LV dysfunction and
The coexistence of hypertension in diabetes is particularly
overt symptoms, and in these individuals, ACEIs and BBs are
pernicious because of the strong linkage of the 2 conditions
again indicated. Aldosterone antagonists also may be of value
with all CVD,168,169 stroke,87,109,110,168,169,174–176 progression
in this situation.140 Loop diuretics are often necessary to
of renal disease,165,175,177,178 and diabetic retinopathy.179 The
control volume retention. However, there is no evidence that
United Kingdom Prospective Diabetes Study (UKPDS)174
diuretics prevent progression of disease, and diuretics can
demonstrated that each 10 mm Hg decrease in SBP was
also increase serum creatinine levels when used in excess.
associated with average reductions in rates of diabetes-related
Patients with stage D (NYHA class IV) HF may require
mortality of 15%; myocardial infarction, 11%; and the
advanced care, such as inotropic drugs, implantable defibril-
microvascular complications of retinopathy or nephropathy,
lators, biventricular pacemakers, mechanical-assist devices,
13%. Randomized controlled trials that have included large
or transplantation, in addition to the treatment described
diabetic populations, including UKPDS, Hypertension Opti-
above for stage C patients.
mal Treatment (HOT) Trial, SHEP, Syst-EUR,67 HOPE
HF is a "compelling indication" for the use of ACEIs.
Study,110 Losartan Intervention For Endpoint Reduction in
Abundant evidence exists to justify their use with all stages of
Hypertension Study (LIFE), and ALLHAT, have demon-
HF (Table 12). In patients intolerant of ACEIs, ARBs may be
strated that adequate BP control improves CVD outcomes,
used. BBs are also recommended in HF because of clinical
especially stroke, when aggressive BP targets are
studies demonstrating decreased morbidity and mortality and
improvement in HF symptoms (Table 12).
Microalbuminuria (30 to 300 mg/d) is associated with
Aldosterone antagonists may provide additional benefit in
increased CVD risk in diabetics and other high-risk pa-
patients with severe LV dysfunction, usually late stage C
tients.67,181 Overt albuminuria (⬎300 mg/d or ⬎200 mg/g
(NYHA class III–IV). In the Randomized Aldactone Evalu-
creatinine on spot urine) or renal insufficiency (estimated
ation Study (RALES), low-dose spironolactone (12.5 to 25
GFR ⬍60 mL/min, corresponding to serum creatinine ⬎1.5
mg daily), when added to standard therapy, decreased mor-
in men or ⬎1.3 mg/dL in women) defines the presence of
chronic kidney disease (CKD) in diabetic patients. SBP
Calcium channel blockers may be useful in diabetics,
correlates better than DBP with renal disease progression in
particularly as part of combination therapy to control BP.
diabetics.171,177,178,182,183 The rate of decline in renal function
They were shown to reduce CVD events in diabetics com-
among patients with diabetic nephropathy has been reported
pared with placebo in several clinical outcome tri-
to be a continuous function of arterial pressure down to
als.87,101,113,118 In the diabetic cohort of ALLHAT, amlodipine
approximately 125 to 130 mm Hg SBP and 70 to 75 mm Hg
was as effective as chlorthalidone in all categories except HF,
where it was significantly inferior.109 The Appropriate Blood
The JNC 7 recommendations are consistent with guidelines
Pressure Control in Diabetes (ABCD) study in diabetics was
from the American Diabetes Association (ADA),88,164 which
stopped prematurely when it was found that the dihydropyr-
has also recommended that BP in diabetics be controlled to
idine nitrendipine was inferior to lisinopril in reducing the
levels of 130/80 mm Hg or lower (although available data are
incidence of ischemic cardiac events.188 However, in normo-
somewhat sparse to justify the low target level of 130/
tensive diabetics in the Second ABCD (ABCD2) study,
80 mm Hg). Whatever the goal level, rigorous control of BP
nitrendipine was equivalent to lisinopril in stroke prevention
is paramount for reducing the progression of diabetic ne-
and in retardation of the development of albuminuria.189
phropathy to ESRD.88,164,177,178,181–183
Chronic Kidney Disease
Regarding the selection of medications, clinical trials with
diuretics, ACEIs, BBs, ARBs, and calcium antagonists have
Age and Kidney Function
demonstrated benefit in the treatment of hypertension in both
Renal excretory function, as represented by GFR, deteriorates
type 1 and type 2 diabetics.87,88,109,164,175,180 The question of
with age beginning in the third or fourth decade of life. By the
which agent class is superior for lowering BP is somewhat
sixth decade, GFR commonly declines by 1 to 2 mL/min per
moot because the majority of diabetic patients will require 2
year. This age-related loss of renal function is proportional to
or more drugs to achieve BP control.164,171,184
BP level, and the rate of GFR deterioration can accelerate to4 to 8 mL/min per year if SBP remains uncontrolled.165 Such
Thiazide-type diuretics are beneficial in diabetics, either
rates of deterioration may lead to the development of ESRD
alone or as part of a combined regimen. In the prespecified
and the need for dialysis or transplantation, especially in
diabetic subgroup of ALLHAT, therapy that began with
those with other coexistent renal disease.
chlorthalidone reduced the primary end point of fatal CHD
CKD is defined as either (1) reduced excretory function
and MI to the same degree as therapy based on lisinopril or
with an eGFR ⬍60 mL/min/1.73 m2 (approximately corre-
amlodipine. Of potential concern is the tendency for thiazide-
sponding to a creatinine of ⬎1.5 mg/dL in men or ⬎1.3
type diuretics to worsen hyperglycemia, but this effect tended
mg/dL in women) or (2) the presence of albuminuria (⬎300
to be small and did not produce more CV events compared
mg/d or 200 mg/g creatinine). In a number of laboratories,
with the other drug classes.185
serum creatinine is being replaced as an index of renal
Therapy with an ACEI also is an important component of
function by eGFR, the values of which are derived from
newer algorithms that include adjustments for gender, race,
tients.67,172,173,178,179 ACEIs may be used alone for BP lower-
and age. These algorithms are available on web sites.66 The
ing but are much more effective when combined with a
measurements appear to be of greater value than 24-hour
thiazide-type diuretic or other antihypertensive drugs. The
urine collections for creatinine clearance.
ADA has recommended ACEIs for diabetic patients over 55
Urinary albumin excretion has diagnostic and prognostic
years old at high risk for CVD and BBs for those with known
value equivalent to reduced eGFR. To avoid inaccuracies
CAD.88 In the Micro-Hope subanalysis of the HOPE Study,
associated with 24-hour urine collections, spot urine samples
which included both hypertensive and normotensive individ-
may be used and the ACR determined. Microalbuminuria is
uals,186 high-risk diabetic patients treated with ACEI added to
present when the spot urine ACR is between 30 and 200 mg
conventional therapy showed a reduction in combined MI,
albumin/g creatinine. ACR values ⬎200 mg albumin/g cre-
stroke, and CVD death of about 25% and reduction in stroke by
atinine signify the presence of CKD.
about 33% compared with placebo plus conventional therapy.
With respect to microvascular complications, the ADA has
CVD Risk in CKD
recommended both ACEIs and ARBs for use in Type 2 diabetic
CVD is the most common cause of death in individuals with
patients with CKD because these agents delay the deterioration
CKD, and CKD is itself an independent risk factor for CVD.
in GFR and the worsening of albuminuria.88,164,171,181
Individuals with eGFR ⬍60 mL/min have an approximate
BBs, especially 
16% increase in CVD mortality, and individuals with eGFR
1-selective agents, are beneficial in dia-
betics as part of multidrug therapy, but their value as
30 mL/min, a 30% increase.190 CVD risk also exhibits a
continuous relationship with albuminuria; the presence of
monotherapy is less clear. A BB is indicated in a diabetic with
microalbuminuria confers a 50% increase in risk and the
ischemic heart disease but may be less effective in preventing
presence of macroalbuminuria, a 350% increase.191
stroke than an ARB, as was found in the LIFE study.187Although BBs can cause adverse effects on glucose ho-
meostasis in diabetics, including worsening of insulin sensi-
NHANES III data indicated that about 3% (5.6 million
tivity and potential masking of the epinephrine-mediated
people) of adults in the United States had elevated serum
symptoms of hypoglycemia, these problems are usually easily
creatinine values and 70% of these had hypertension.192
managed and are not absolute contraindications for BB use.
While 75% of individuals received treatment, only 11% with
Chobanian et al
JNC 7 – COMPLETE REPORT
hypertension and elevated serum creatinine had BP ⬍130/
stroke period and is thought by some to be a compensatory
85 mm Hg and only 27% had BP ⬍140/90 mm Hg.193 In the
physiological response to improve cerebral perfusion to
prevention of CKD, the value of vigorous antihypertensive
ischemic brain tissue. As a result, it has been common
therapy is most pronounced in those individuals with the
practice after acute cerebral infarction to reduce or withhold
greatest degrees of albuminuria. In the Modification of Diet
BP treatment until the clinical condition has stabilized. There
and Renal Disease (MDRD) study, individuals with protein-
still are no large clinical studies on which to base definitive
uria had slower rates of progression to ESRD if their SBP
recommendations. Nevertheless, the American Stroke Asso-
values were ⬍130 mm Hg. A meta-analysis of individuals
ciation has provided the following guidelines: In patients with
with CKD and albuminuria found that positive predictors of
recent ischemic stroke whose SBP is ⬎220 mm Hg or DBP
outcome were lower SBP levels (110 to 129 mm Hg), lower
120 to 140 mm Hg, cautious reduction of BP by about 10% to
albumin excretion ratio (AER) (⬍1.0 g/d), and the presence
15% is suggested, while carefully monitoring the patient for
of ACEI therapy.194,195 However, in the African American
neurological deterioration related to the lower pressure. If the
Study of Kidney Disease and Hypertension (AASK) study of
DBP is ⬎140 mm Hg, carefully monitored infusion of so-
African American individuals with hypertensive CKD, those
dium nitroprusside should be used to reduce the BP by 10 to
achieving a mean BP of 128/78 mm Hg experienced renal
deterioration at the same rate as those achieving a mean of
BP control affects the use of thrombolytic agents in
141/85 mm Hg.196 Many studies demonstrate that antihyper-
ischemic stroke. SBP ⬎185 mm Hg or diastolic pressures
tensive regimens that include an ACEI or ARB are more
⬎110 mm Hg are contraindications to the use of tissue
effective in slowing progression of CKD than other antihy-
plasminogen activator (t-PA) within the first 3 hours of an
ischemic stroke. Once a thrombolytic agent has been initi-
The joint recommendations of the American Society of
ated, BP should be monitored closely, especially in the first
Nephrology and the National Kidney Foundation (NKF)
24 hours after initiation of treatment. SBP ⱖ180 mm Hg or
provide useful guidelines for management of hypertensive
DBP ⱖ105 mm Hg usually necessitates therapy with intra-
patients with CKD. They recommend a goal BP for all CKD
venous agents to prevent intracerebral bleeding.199
patients of ⬍130/80 mm Hg and a need for more than 1
Other Special Situations
antihypertensive drug to achieve this goal. The guidelinesindicate that most patients with CKD should receive an ACEI
or an ARB in combination with a diuretic and that many will
The prevalence, impact, and control of hypertension differ
require a loop diuretic rather than a thiazide. In addition, if
across racial and ethnic subgroups of the US population. In
there is a conflict between the goals of slowing progression of
African Americans, hypertension is more common, more
CKD and CVD risk reduction, individual decision-making is
severe, develops at an earlier age, and leads to more clinical
recommended, based on risk stratification.
sequelae than in age-matched non-Hispanic whites.200 Mex-ican Americans and Native Americans have lower control
Patients with Cerebrovascular Disease
rates than non-Hispanic whites and African Americans.201,202
The risk of clinical complications of cerebrovascular disease
The pathogenesis of hypertension in different racial sub-
including ischemic stroke, hemorrhagic stroke, and dementia
groups may differ with respect to the contributions of such
increases as a function of BP levels. Given the population
factors as salt, potassium, stress, cardiovascular reactivity,
distribution of BP, most ischemic strokes occur in individuals
body weight, nephron number, sodium handling, or hormonal
with prehypertension or stage 1 hypertension. The incidence
systems, but in all subgroups, the pathogenesis is multifacto-
of ischemic or hemorrhagic stroke is reduced substantially by
rial.200,203 African Americans have a greater prevalence of
treatment of hypertension. No specific agent has proven to be
other cardiovascular risk factors, especially obesity.200,203
clearly superior to all others for stroke protection. In the LIFE
Much of the variance in hypertension-related sequelae across
study, there were fewer strokes in the losartan-treated group
racial or ethnic groups may be attributable to differences in
than in the group treated with atenolol.102 In the ALLHAT
socioeconomic conditions, access to healthcare services, or
study, the stroke incidence was 15% greater with ACEI than
attitudes, beliefs, and deficits in accurate health-related infor-
with thiazide-type diuretic or dihydropyridine CCB, but the
mation.200,203 For example, when medications and provider
BP reduction in the lisinopril group was also less than with
services were provided free of charge as in the Hypertension
chlorthalidone or amlodipine.109
Detection and Follow-up Program, African American men
With respect to the prevention of recurrent stroke,
treated with the intensive "Stepped-Care Approach" actually
PROGRESS demonstrated that addition of the diuretic inda-
benefited more than whites.204
pamide to the ACEI perindopril caused a 43% reduction in
Weight reduction and sodium reduction are recommended
stroke occurrence.111 The reduced incidence of stroke ap-
for all prehypertensive and hypertensive patients but may be
peared related to the BP reduction obtained by the combina-
particularly effective in minorities. The salt content of some
tion therapy even though many patients on entry into the
traditional diets in minorities may be very high.205 The
study were not hypertensive.197 No significant reduction was
low-sodium DASH eating plan was associated with greater
present in those on perindopril alone whose BP was only
reductions in BP in African Americans than other demo-
5/3 mm Hg lower than in the control group.
graphic subgroups.94 In clinical trials, lowering BP prevents
The management of BP during an acute stroke remains
sequelae of hypertension in all racial or ethnic groups.200,203
controversial. BP is often elevated in the immediate post-
Nonetheless, monotherapy with BBs, ACEIs, or ARBs lowers
BP to a somewhat lesser degree in African Americans than
TABLE 13.
Clinical Criteria Defining the Metabolic Syndrome
whites.109,206–208 In the ALLHAT trial with more than 15 000
in ATP III
blacks, the ACEIs were less effective in lowering blood
Waist circumference
pressure than either the thiazide-type diuretic or the CCBs.
⬎102 cm (⬎40 inches) for men
This was associated with a 40% greater risk of stroke, 32%
⬎88 cm (⬎35 inches) for women
greater risk of HF, and 19% greater risk of CVD in thoserandomized to the ACEI versus the diuretic.109 The interracial
differences in BP-lowering observed with these drugs are
ⱖ130 mm Hg systolic and/or
abolished when they are combined with a diuretic.109,203,208
ⱖ85 mm Hg diastolic
Racial differences in incidence of antihypertensive drug
side effects may occur; African Americans and Asians have a
ⱖ110 mg/dL or 6.1 mmol/L
3- to 4-fold higher risk of angioedema109,209,210 and have more
cough attributed to ACEIs than whites.211
ⱖ150 mg/dL or 1.69 mmol/L
Several other benefits of treatment have been demonstrated
in minority populations. A 28% reduction in mortality was
⬍40 mg/dL (1.04 mmol/L) in men
observed in African Americans who received BB therapyafter acute myocardial infarction compared with those not
⬍50 mg/dL (1.29 mmol/L) in women
receiving a BB.212 A greater degree of preservation of renal
Source: Executive Summary of the Third Report of The National Cholesterol
function occurred in African Americans with hypertensive
Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treat-ment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA
nephrosclerosis treated with a regimen containing an ACEI
compared with BB or a calcium antagonist.196 No largeoutcome studies have been carried out with ARBs in African
metabolic syndrome in adults in the United States was
American and other minority patients. Unfortunately, suffi-
estimated at 23.7% or about 47 million individuals.221 BMI
cient numbers of Mexican Americans, other Hispanic Amer-
(kg/m2) is related to the metabolic syndrome in both men and
icans, Native Americans, or Asian/Pacific Islanders have not
women (Table 14).222 In addition, because abdominal obesity
been included in most of the major clinical trials to allow
is also correlated with the metabolic syndrome, ATP III uses
reaching strong conclusions about their responses to individ-
it rather than BMI. This becomes important in overweight
ual antihypertensive therapies.
individuals with a BMI 25 to 29.9 kg/m2 and large waist
Irrespective of whether race or ethnicity should be a
circumference (⬎40 inches in men, ⬎35 inches in women)
significant consideration in the choice of individual antihy-
who may have metabolic syndrome despite not being obese.
pertensive drugs, the use of combination or multiple antihy-
The metabolic syndrome will likely increase further in the
pertensive drug therapy, which usually includes a thiazide-
next several years, primarily because of the rapid increase in
type diuretic, in minority groups will lower BP and reduce the
obesity. The health problems related to the metabolic syn-
burden of hypertension-related cardiovascular and renal
drome will likely escalate dramatically.
Age Trends
The prevalence of the metabolic syndrome is highly age-dependent. A prevalence of 7% among adults aged 20 to 29
Definition and AssociationsThe term "metabolic syndrome" describes a constellation of
years rises to 40% or more among Americans over 60 years old.
cardiovascular risk factors related to hypertension, abdominal
Clinical Impact
obesity, dyslipidemia, and insulin resistance. The definition
The metabolic syndrome is associated in men with a 4-fold
adopted by the National Cholesterol Education Program
increase in risk for fatal CHD and a 2-fold greater risk of
(Adult Treatment Panel [ATP] III) guidelines in 200121 is the
CVD and all-cause mortality, even after adjustment for age,
presence of 3 or more of the 5 risk factors (Table 13). The
LDL-C, smoking, and family history of CHD.223 The meta-
World Health Organization has a somewhat different defini-
bolic syndrome is associated with increased CHD risk in
tion of the metabolic syndrome, but for consistency JNC 7
women.224 Patients with the metabolic syndrome have a 5- to
has adopted the ATP III definition.
9-fold increased risk of developing diabetes.225,226
Several other associated features have been reported, includ-
ing hyperinsulinemia, insulin resistance, and higher density of
TABLE 14.
Estimated Prevalence of the Metabolic Syndrome
LDL-C particles.213 The metabolic syndrome has also been
Using the ATP III Definition Among Normal Weight, Overweight,
associated with high levels of inflammatory risk markers,214
and Obese Men and Women in NHANES III222
reduced fibrinolysis (including elevated plasminogen activator
Metabolic Syndrome
inhibitor-1),215 heightened magnitude of oxidative stress,216,217
microalbuminuria,218 abnormalities in autonomic regulation,219and activation of the renin-angiotensin-aldosterone axis.220
When the ATP III criteria were applied to the data from the
NHANES III survey (1988 –1994), the prevalence of the
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 15.
Relative 10-Year Risk for Diabetes, Hypertension,
TABLE 16.
Lifestyle Changes Beneficial in Reducing Weight*
Heart Disease, and Stroke Over the Next Decade Among Men
Initially Free of Disease Stratified by Baseline BMI231
Decrease time in sedentary behaviors such as television watching, videogame play, or spending time online
Increase physical activity such as walking, biking, aerobic dancing, tennis,
soccer, basketball, etc.
Decrease portion sizes for meals, snacks
Reduce portion sizes or frequency of consumption of calorie-containingbeverages
*For more detailed information refer to the Clinical Guidelines on the
Identification, Evaluation, and Treatment of Overweight and Obesity in Adults.
Obes Res. 1998;6(suppl):51S–209S.
Clinical Management of the Metabolic SyndromeThe cornerstone for clinical management in adults is appro-
whom obesity and related health problems are increasing at
priate lifestyle changes.
nearly double the rate in ethnic minorities compared withwhites.232,233 The rapid increase in the population of ethnic
Overweight and Obesity. Treatment of overweight and obe-
minorities in the United States is another factor that will lead
sity is summarized in the next section using key principles in
to a rise in the prevalence of obesity and its complications
the Clinical Guidelines on the Identification, Evaluation, and
unless effective, culturally diverse, population-based health
Treatment of Overweight and Obesity in Adults.227
promotion strategies are promoted.
Physical Activity. The metabolic syndrome can improve with
Prevention and Lifestyle Modifications for Overweight
increased physical activity.228 (See the section Prevention and
and Obesity
Lifestyle Modifications for Overweight and Obesity.)
The major goal of management of both the metabolic syn-
Prehypertension and Hypertension. The vast majority of
drome and overweight and obesity is to reduce the age-related
individuals with the metabolic syndrome will fall into the
rate of weight gain. This challenging task will require a
categories of prehypertension or stage 1 hypertension. Life-
complex combination of healthy behaviors, including de-
style modification is the cornerstone of management in all
crease in sedentary activities, increase in physical activity,
patients with prehypertension or with the metabolic syn-
and reduction in calorie intake (Table 16). Simple yet
drome, but if BP exceeds 140/90 mm Hg, pharmacological
practical suggestions include reducing time spent watching
therapy is indicated as described in the hypertension treat-
television or being online and increasing time spent walking
ment algorithm (Figure 16).
or in activities that raise heart rate. The emphasis for weightmanagement should be on avoidance of excess total energy
Lipids. Elevated TG and reduced HDL are typical lipid
intake and a regular pattern of physical activity. Reducing
abnormalities in metabolic syndrome. Elevated LDL is not a
food portion sizes and limiting fat intake can assist in
prime feature of metabolic syndrome but is important in
reducing overall calorie intake. High-sodium diets may be
clinical management.21
especially deleterious in obese subjects.234
Specific nutrient intakes for individuals should be based on
Impaired Glucose Tolerance and Diabetes. Modest lifestyle
lipoprotein levels, BP, and the presence of coexisting heart
change including healthful nutrition and increased physical
disease, diabetes, and other risk factors. For example, adop-
activity can reduce the development of diabetes by nearly
tion of the well-studied low-sodium DASH eating plan94
60% in high-risk individuals.229 Management guidelines pub-
provides heart-healthy foods that can be used to promote
lished by the American Diabetes Association are appropriate
weight loss, reduce BP in both hypertensive and prehyper-
for individuals with impaired fasting glucose and diabetes.230
tensive individuals, and reduce LDL. The benefits of modest
lifestyle changes on cardiovascular risk factors are well
All patients with lipid abnormalities for LDL, HDL, or TG
documented. In the Framingham Heart Study, weight loss of
should be treated according to the ATP III recommendations.21
5 pounds or greater was associated with reductions incardiovascular risk of about 40%.235 A 10% reduction in body
Overweight and Obesity
weight can reduce disease risk factors.227
Prevalence and Epidemiology
Physical activity is a key feature of treatment. Increased
Using the NHANES databases for the periods 1988 to 1994
physical activity, when combined with a reduction in calories,
versus 1999 to 2000, the age-adjusted prevalence of obesity
is essential to weight loss success. Based on the available
(BMI ⱖ30 kg/m2) among US adults increased from 22.9% to
evidence, the recommendation is to engage in regular phys-
30.5%,33 while the prevalence of overweight (BMI ⱖ25
ical activity at least 30 minutes per day, most days of the
kg/m2) increased from 55.9% to 64.5%. Obese subjects,
week (see Table 9). In addition, physical activity is critical to
especially men, with no other risk factors have increased
the maintenance of weight loss and is important for overall
relative risk for CVD (Table 15).231
reduction in cardiovascular risk; 60 to 90 minutes per week of
Obesity occurs more often among Hispanics, Native Amer-
walking can reduce CHD mortality by about 50%.236 The
icans, and African Americans than whites in the United
CVD benefits of slow walking appear to be comparable to
States. These demographic differences extend to children, in
those of walking more quickly, suggesting that the most
important predictor of benefit was walking time, not speed.
electrocardiography, was reduced significantly more by a
Exercise programs appear beneficial at any age and are
losartan-based than atenolol-based regimen despite equiva-
associated with overall reductions in CVD outcomes by about
lent BP lowering.102
50%.237 Although aerobic fitness may negate much of thecardiovascular risk associated with obesity,
Peripheral Arterial Disease
238 studies report
Major risk factors for peripheral arterial disease (PAD) are
that individuals with obesity have much lower levels of
hypertension, diabetes, and smoking. Symptomatic peripheral
physical activity and poorer aerobic fitness than leaner
arterial disease is associated with a greatly increased risk of
death from CVD, in part because diffuse atherosclerosis,
Left Ventricular Hypertrophy
CAD, and renovascular disease frequently coexist in these
The common feature of all forms of LVH is increased left
patients. Therefore, more intensive screening for these related
ventricular mass, although there are many different presenta-
cardiovascular disorders is appropriate in persons with PAD.
tions and subtypes, each with different prognosis and thera-
Renovascular hypertension should be strongly considered in
py.240 LVH subclasses can be characterized generally by the
this population if BP is uncontrolled and if ACEI or ARB
relative wall thickness, the presence or absence of reduced
treatment is being considered.
contractility, and the end-diastolic chamber size. LVH can
Antihypertensive drug treatment is ineffective in relieving
occur in endurance athletes with normal or supranormal
the symptoms of PAD, and vasodilator agents such as ACEIs,
systolic function, large end-diastolic volumes, and elongation
CCBs, ␣-adrenergic blockers, and direct vasodilators do not
of myofibrils (eccentric hypertrophy). LVH due to hyperten-
improve walking distance or symptoms of claudication.247–249
sion is usually characterized by concentric hypertrophy with
This lack of efficacy may be due to inability of maximally
circumferential hypertrophy of myofibrils, normal or in-
dilated diseased vessels to dilate further during exercise,
creased contractility, increased relative wall thickness, nor-
redistribution of flow caused by the creation of a "steal"
mal or low end-diastolic volumes, and at times impaired
phenomenon where blood flow increases in nondiseased
relaxation (diastolic dysfunction). In population-based sam-
vascular beds at the expense of diseased beds, or alteration of
ples, 30% to 50% of individuals with stage 1 and 2 hyper-
pressure–flow relationships distal to the occluded areas by BP
tension have impaired LV relaxation, and in more severe
reduction. BBs may cause peripheral vasoconstriction and
forms of hypertension, about two-thirds have abnormal LV
have the potential to increase the frequency of intermittent
relaxation. In untreated or poorly treated individuals, LVH
claudication in individuals with PAD. However, recent stud-
becomes a major risk factor for dilated cardiomyopathy and
ies have shown that BBs have little effect on walking distance
or calf blood flow in patients with intermittent claudica-tion.250 Thus, BBs can be used in PAD patients, especially if
Detection and Risk
needed for treatment of CAD or HF.
Echocardiography is much more sensitive than electrocardi-
No selective outcome benefit has been demonstrated for
ography (ECG) for detection of LVH, although ECG-LVH is
any individual class of antihypertensive medication in pa-
a highly specific indicator for the condition. Individuals with
tients with PAD.109 Therefore, antihypertensive drug choices
LVH are more than twice as likely to suffer premature
should be made on the basis of the presence or absence of
cardiovascular events or death. Current ECG algorithms
compelling indications. If Raynaud's phenomenon is present,
defining LVH produce a high false-positive rate in African
CCBs can be used.251 LDL lowering will reduce the risk for
Americans and overestimate the prevalence of LVH in this
CVD events in people with PAD.252
population.242,243 The attributable risk of LVH for all-causemortality is greater than that of single or multivessel coronary
artery disease or low EF.
Treating hypertension in PAD patients reduces the risk of MI,stroke, HF, and death.253 A structured walking program has
been shown to increase the pain-free and maximum walking
Several studies suggest that LVH regression is associated
distances in patients with intermittent claudication.254 Smok-
with a lower overall CVD risk. Weight loss, salt restriction,
ing cessation may be the most important factor in whether
and BP lowering with most antihypertensive agents produce
PAD progresses. Patients should be encouraged and assisted
LVH regression. Selection of individual drugs appears to be
to stop smoking. Lipid abnormalities should be controlled
less important, but certain trends have emerged. Fifty studies
using lifestyle modification or drugs as appropriate. Coexist-
of LVH regression conducted before 1996 were subjected to
ing glucose intolerance or insulin resistance calls for in-
meta-analysis.244 In these studies, predictors of LV mass
creased exercise and weight reduction, and aggressive man-
reduction during treatment were higher pretreatment LV
agement of diabetes is indicated. Table 17 outlines medical
mass, greater fall in SBP or DBP, and longer duration of
therapies of PAD.
treatment. The most consistent reduction in LV mass wasachieved with ACEIs, the least reduction occurred with BBs,
Hypertension in Older People
and intermediate benefits occurred for diuretics and calcium
The number of Americans aged 65 years or older has
antagonists. However, in both the Treatment of Mild Hyper-
increased from 24.2 million to 32.6 million from 1980 to
tension Study and the VA Cooperative Monotherapy trial,
2000 and is expected to continue to rise.255 SBP increases
diuretic therapy achieved the greatest benefit in LV mass
almost linearly with age in industrialized societies (Figure
reduction.245,246 The LIFE study found that LVH, defined by
12), as does the overall prevalence of hypertension and the
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 17.
Medical Therapy of Peripheral Arterial Disease
as HF events (54%), myocardial infarctions (27%), andoverall CVD (32%)24 as compared with the placebo group.
Using a similar design and sample size, the Syst-EUR study
Achieve ideal body weight
compared a regimen based on nitrendipine to placebo and
Structure exercise program
found a significant reduction in stroke (41%) as well as
Achieve goal blood pressure
overall CVD events (31%).113 A meta-analysis of 8 placebo-
Control lipids (goal LDL ⬍100 mg/dL)
controlled trials in 15 693 elderly patients followed for 4
Prevent or control diabetes
years found that active antihypertensive treatment reduced
Administer antiplatelet therapy (aspirin, clopidogrel, or both)
coronary events (23%), strokes (30%), cardiovascular deaths(18%), and total deaths (13%), with the benefit particularly
Consider use of Cilostazol for symptoms of claudication if exercise alone isineffective
great in those older than 70 years.258 Benefits of therapy havebeen demonstrated even in individuals over 80 yearsold.116,259 Analyses of treatment trials in the elderly by the
proportion of hypertensives with isolated SBP elevation
Hypertension Trialists group have suggested that the choice
(ISH) (Figure 17).192 In contrast, DBP increases in parallel
of initial agent is less important than the degree of BP
with SBP until about age 55, after which it declines as a
reduction achieved.90
manifestation of age-related increases in central arterial
Accurate and representative BP measurement can pose
stiffness. By age 60, about two-thirds of those with hyper-
special problems in some older individuals (see the section
tension have ISH, and by age 75, almost all hypertensives
Accurate Blood Pressure Measurement in the Office). BP is
have systolic hypertension and about three-fourths of hyper-
more variable in the older patient, often due to stiff large
tensives have ISH.
arteries and age-related decreases in baroreflex buffering.
Individuals over age 60 represent the most rapidly growing
Exaggerated BP drops may occur in the elderly during
segment of the US population, and even in those who remain
postural change (see the section Orthostatic Hypotension),
normotensive between 55 and 65 years old, there remains a
after meals,260 and after exercise.97 Pseudohypertension,
lifetime risk of developing hypertension that exceeds 90%.16
where cuff BP overestimates the actual intra-arterial pressure
At the same time, there is a 3- to 4-fold increase in CVD risk
due to relative inability of the BP cuff to compress a
in older compared with younger individuals. These factsprompted the NHBPEP to issue a Clinical Advisory statement
thickened, stiff, or calcified brachial artery, is an uncommon
in May, 2000, stating that SBP should be the primary target
condition in older persons. But this condition should be
for the diagnosis and management of older people with
strongly considered if usual treatment does not reduce BP,
hypertension.256 Currently, BP control rates (systolic
especially in those patients who complain of symptoms
⬍140 mm Hg and diastolic ⬍90 mm Hg) are only about 20%
consistent with postural hypotension.261 A relatively small
in older hypertensives, largely due to poor control of SBP.257
percentage of elderly patients have a reversible form ofhypertension, most commonly due to renovascular disease,
which is seen most often in smokers.262
In the SHEP study involving hypertensives over 60 years old
SBP provides more appropriate classification and risk
with pretreatment SBP ⬎160 and DBP ⬍90 mm Hg, indi-
stratification than DBP in the elderly. In the Framingham
viduals treated with chlorthalidone (with or without BB) had
Heart Study, SBP alone correctly classified the BP stage in
reductions in the primary end point of stroke (36%), as well
94% of adults over 60 years old, while DBP alone correctlyclassified 66%.192 Pulse pressure (PP) (SBP ⫺ DBP) is onlymarginally stronger than SBP for risk stratification in indi-viduals over age 60, but under age 60, PP is not useful as aCVD risk predictor.18 PP generally decreases as a result ofSBP lowering,24,263 but no prospective clinical trial has usedPP as the primary clinical end point. Thus, on balance, SBPis superior to PP and DBP as a way to stratify patients and asa target for treatment in older persons.
Although there is no randomized prospective clinical trial
that has conclusively proven the benefits of treatment inindividuals with Stage 1 systolic hypertension (140 to159 mm Hg), hypertension therapy should not be withheld inthese patients, and therapy should not be withheld on thebasis of age. There is no definitive evidence of an increase in
Figure 17. Frequency distribution of untreated hypertensive
individuals by age and hypertension subtype. Frequency distri-
risk of aggressive treatment (a J-curve) unless DBP is
bution of untreated hypertensive individuals by age and hyper-
lowered to ⬍55 or 60 mm Hg by treatment.155
tension subtype. Numbers at the tops of bars represent theoverall percentage distribution of untreated hypertension in that
age group. f, ISH (SBPⱖ140 mm Hg and DBP ⬍90 mm Hg); u,
Weight loss and reduced sodium intake are particularly
SDH (SBP ⱖ140 mm Hg and DBP ⱖ90 mm Hg); 䡺, IDH (SBP
beneficial in older people. In Trial of nonpharmacologic
⬍140 mm Hg and DBP ⱖ90 mm Hg). Source: Franklin SS et al.
Hypertension 2001;37:869 – 874.
Interventions in the Elderly (TONE), reducing sodium to
80 mmol (2 g) per day reduced BP over 30 months, and about
sion may also lead to transient high readings that are not
40% of those on the low-salt diet were able to discontinue
experienced throughout the day. This can be documented by
their antihypertensive medications.264 When weight loss was
home BP or ambulatory BP readings.
combined with salt reduction, an additional BP decrease was
Inadequate diuretic therapy is common in resistant hyper-
seen. Older persons should also be encouraged to avoid
tension. Volume overload, once recognized, can be managed
excessive alcohol intake and remain as physically active as
by use of appropriate diuretics. While a thiazide-type diuretic
is recommended for the majority of hypertensive patients, a
Use of specific drug classes in older people is largely
loop diuretic is often required for patients who have a
similar to that recommended in the general algorithm and for
decreased GFR or HF.
individual compelling indications. Combination therapy with
Failure to receive adequate medications can be the result of
two or more drugs is generally needed to achieve optimal BP
reluctance on the part of the patient or practitioner to use
control. In routine practice, if the systolic goal is achieved,
effective doses of medications. Causes and approaches to
the diastolic goal will almost always be reached as well.
nonadherence are discussed in subsequent sections of this
A significant number of elderly individuals have widely
variable BP with exaggerated high and low extremes. Such
Drug interactions that induce resistance may be difficult to
individuals deserve consideration for a slow titration ap-
detect unless the patient is asked open-ended questions
proach, as do individuals with a history of medication side
regarding what they take when experiencing pain and what
effects and those with orthostatic hypotension. Unfortunately,
food supplements, health food preparations, and over-the-
the misperception that many elderly have "brittle hyperten-
counter and Internet-purchased medications and supplements
sion" has contributed to widespread inadequacy of drug
they use. Nonsteroidal anti-inflammatory drugs and pressor
titration and to poor BP control.
agents in cold remedies, nasal vasodilators, and some non-
traditional remedies may counter the antihypertensive effects
BP measurements are typically recorded in the sitting posi-
of prescribed medications.
tion. This practice, while convenient for the practitioner,
If resistant hypertension persists after remediable causes
limits the ability to diagnose orthostatic hypotension (OH).
are identified and corrected, then a concerted search for a
Normally, standing is accompanied by a small increase in
cause of secondary hypertension should be conducted (Table
DBP and a small decrease in SBP when compared with
7). If resistance still persists, consultation with a hypertension
supine values. OH is present when there is a supine-to-
specialist is a logical next step.
standing BP decrease ⬎20 mm Hg systolic or ⬎10 mm Hg
Specific causes of resistant hypertension are listed in Table
diastolic. There is more OH in diabetics. OH occurred in
18. They usually can be identified by appropriate evaluation,
about 7% of men over 70 years old in the Honolulu Heart
and, once identified, can almost always be treated effectively.
Study, was highly age-dependent, and carried with it a 64%
The prevalence of truly resistant hypertension is small.
increase in age-adjusted mortality compared with a controlpopulation.265 There is a strong correlation between the
Cognitive Function and Dementia
severity of OH and premature death as well as increased
Dementia and cognitive impairment occur more commonly
numbers of falls and fractures.265–267 The causes of OH
in people with hypertension. Reduced progression of
include severe volume depletion, baroreflex dysfunction,
cognitive impairment may occur with effective antihyper-
autonomic insufficiency, and certain venodilator antihyper-
tensive therapy.269,270 Narrowing and sclerosis of small
tensive drugs, especially ␣-blockers and ␣--blockers. Di-
penetrating arteries in the subcortical regions of the brain
uretics and nitrates may further aggravate OH.
are common findings on autopsy in chronic hyperten-
In treating older hypertensive patients, clinicians should be
sion.271–274 These changes are believed to contribute to
alert to potential OH symptoms such as postural unsteadiness,
hypoperfusion, loss of autoregulation, compromise of the
dizziness, or even fainting. Lying and standing BPs should be
blood-brain barrier, and ultimately to subcortical white
obtained periodically in all hypertensive individuals over 50
matter demyelination, microinfarction, and cognitive de-
years old. OH is a common barrier to intensive BP control
cline. MRI studies in persons with chronic hypertension
that should be clearly documented; if present, drug therapy
have revealed greater numbers of subcortical white matter
should be adjusted accordingly and appropriate warnings
lesions and microinfarcts, astrogliosis, ventricular enlarge-
given to patients.
ment, and extracellular fluid accumulation than in age-matched controls.275–285
Resistant Hypertension
Resistant hypertension is defined as the failure to achieve
Mild cognitive impairment (MCI) is a diagnostic category
goal BP in patients who are adhering to full doses of an
that represents a transitional state between normal aging and
appropriate 3-drug regimen that includes a diuretic. Several
mild dementia in which patients exhibit signs of poor recent
causes of resistant hypertension may be present.
memory but can still perform daily tasks such as managing
Improper BP measurement can lead to overestimation of
finances, driving, shopping, and preparing meals.286 Hyper-
intra-arterial pressure. (See section on BP measurement.)
tension and hypercholesterolemia are risk factors for MCI
Falsely high readings may also be observed in those whose
and for other signs of cognitive decline, such as impaired
brachial arteries are heavily calcified or arteriosclerotic and
attention, reaction time, verbal fluency, or executive
cannot be fully compressed.268 Clinic or white-coat hyperten-
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 18.
Causes of Resistant Hypertension
Awareness, Treatment, and Control of High BP in Women.
Women are more likely than men to know that they have
Improper BP measurement
hypertension, to have it treated, and to have it controlled.1 In
NHANES III, approximately 75% of hypertensive black and
Excess sodium intake
white women were aware of their high BP in contrast to just
Volume retention from kidney disease
65% of hypertensive men in these ethnic groups. Overall,61% of hypertensive women, but only 44% of men, were
Inadequate diuretic therapy
being treated with antihypertensive medications. The higher
Drug-induced or other causes
treatment rates in women have been attributed to increased
numbers of physician contacts.
Menopause and Blood Pressure. The effect of menopause on
BP is controversial. Longitudinal studies have not docu-
Nonsteroidal anti-inflammatory drugs; cyclooxygenase 2 inhibitors
mented a rise in BP with menopause, while cross-sectional
Cocaine, amphetamines, other illicit drugs
studies have found significantly higher SBP and DBP inpostmenopausal versus premenopausal women.294 In
Sympathomimetics (decongestants, anorectics)
NHANES III, the rate of rise in SBP tended to be steeper in
Oral contraceptive hormones
postmenopausal compared with premenopausal women until
Adrenal steroid hormones
the sixth decade, when the rate of increase tended to slow.
Cyclosporine and tacrolimus
Staessen et al296 reported that even after adjustment for ageand BMI, postmenopausal women are more than twice as
likely to have hypertension as premenopausal women. In a
Licorice (including some chewing tobacco)
prospective study of conventional and ambulatory BP levels,
Selected over-the-counter dietary supplements and medicines (eg,
postmenopausal women had higher SBP (4 to 5 mm Hg) than
ephedra, ma haung, bitter orange)
pre- and perimenopausal controls.297 The increase in SBP per
Associated conditions
decade was 5 mm Hg greater in the peri- and postmenopausal
women than in the premenopausal group. Thus, there isevidence that at least part of the rise in BP (particularly SBP)
Excess alcohol intake
seen later in life in women is due to menopause. A
Identifiable causes of hypertension (See Table 7.)
menopause-related increase in BP has been attributed to avariety of factors, including estrogen withdrawal, overpro-duction of pituitary hormones, weight gain, or a combinationof these and other yet undefined neurohumoral influences.298
Effective antihypertensive therapy strongly reduces the
Postmenopausal Hormone Therapy and BP. Results of stud-
risk of developing significant white matter changes on
ies evaluating the effects of hormone replacement therapy
MRI.290 However, existing white matter changes, once
(HRT) on BP have been inconsistent. The Women's Health
established, do not appear to be reversible.291,292 The
Initiative (WHI), the largest longitudinal study to address this
optimal SBP/DBP to prevent cognitive decline in older
question, found an average 1 mm Hg increase in SBP over 5.6
individuals is thought by some to be in the SBP 135 to
years of follow-up among 8506 postmenopausal women
150 mm Hg and DBP 70 to 79 mm Hg range.287,288 In the
randomized to conjugated equine estrogen and medroxypro-
SystEUR trial, CCB therapy was superior to placebo in
gesterone acetate as compared with a placebo group.299 There
slowing the decline in cognitive function,
was no difference in DBP between the hormone treatment
groups. Further, in the WHI cross-sectional analysis of almost
parative data are available regarding whether certain
100 000 women aged 50 to 79 years, current hormone use
classes of antihypertensive drugs are superior to others in
was associated with a 25% greater likelihood of having
preventing cognitive decline.
hypertension compared with past use or no prior use.300
Smaller observational and interventional studies have
Hypertension in Women
found different results. In the Baltimore Longitudinal Study
Nonpregnant Women
on Aging (BLSA), women receiving HRT had a significantlysmaller increase in SBP over time than nonusers, but DBP
Sexual Dimorphism of BP and Hypertension Prevalence in
was not affected. The Postmenopausal Estrogen/Progestin
Women. There is a sexual dimorphism in BP, such that
Intervention trial showed no effect of HRT on SBP or
women have lower SBP levels than men during early adult-
DBP.301 In small studies that have used 24-hour ambulatory
hood, while the opposite is true after the sixth decade of life.
monitoring to evaluate the effects of HRT on BP, while
DBP tends to be just marginally lower in women than men
overall results are inconsistent, several of the studies suggest
regardless of age.294 Similarly, in early adulthood, hyperten-
that HRT improves or restores the normal nighttime reduction
sion is less common among women than men. However, after
("dipping") in BP that may be diminished in postmenopausal
the fifth decade of life, the incidence of hypertension in-
women. Such an effect would tend to reduce total BP load
creases more rapidly in women than men, and the prevalence
and thereby reduce target organ damage.298
of hypertension in women is equal to or exceeds that in men
Overall, HRT-related change in BP is likely to be modest
during the sixth decade of life. The highest prevalence rates
and should not preclude hormone use in normotensive or
of hypertension are observed in elderly black women, with
hypertensive women. All hypertensive women treated with
hypertension occurring in more than 75% of women older
HRT should have their BP monitored closely at first and then
than 75 years.295
at 6-month intervals.
TABLE 19.
Classification of Hypertension in Pregnancy
Chronic hypertension
BP ⱖ140 mm Hg systolic or 90 mm Hg diastolic prior to pregnancy or before 20 weeks gestation
Persists ⬎12 weeks postpartum
BP ⱖ140 mm Hg systolic or 90 mm Hg diastolic with proteinuria (⬎300 mg/24 h) after 20 weeks gestation
Can progress to eclampsia (seizures)
More common in nulliparous women, multiple gestation, women with hypertension for ⱖ4 years, family history ofpreeclampsia, hypertension in previous pregnancy, renal disease
Chronic hypertension with
New onset proteinuria after 20 weeks in a woman with hypertension
In a woman with hypertension and proteinuria prior to 20 weeks gestation:
Sudden 2- to 3-fold increase in proteinuria
Sudden increase in BP
Elevated AST or ALT
Gestational hypertension
Hypertension without proteinuria occurring after 20 weeks gestation
Temporary diagnosis
May represent preproteinuric phase of preeclampsia or recurrence of chronic hypertension abated in midpregnancy
May evolve to preeclampsia
If severe, may result in higher rates of premature delivery and growth retardation than mild preeclampsia
Transient hypertension
Retrospective diagnosis
BP normal by 12 weeks postpartum
May recur in subsequent pregnancies
Predictive of future primary hypertension
ALT indicates alanine aminotransferase; AST, aspartate aminotransaminase; BP, blood pressure.
Oral Contraceptives and BP. Many women taking oral con-
also similar in men and women, but for coronary events, it
traceptives experience a small but detectable increase in BP;
was greater in men. Similarly, a placebo-controlled trial of
a small percentage experience the onset of frank hyperten-
CCB treatment showed treatment benefits for both sex-
sion. This is true even with modern preparations that contain
es.113,304 More recent outcome trials comparing ACEIs,
only 30 g estrogen. The Nurses' Health Study found that
ARBs, or CCBs with diuretics and BBs in older, high-risk
current users of oral contraceptives had a significantly in-
patients have generally shown similar benefits for women and
creased (relative risk [RR]⫽1.8; 95% confidence interval
men.101,102,109 The current evidence indicates that the sex of
[CI]⫽1.5 to 2.3) risk of hypertension compared with never
the patient should not play a role in decisions about whether
users.302 Absolute risk was small: only 41.5 cases of hyper-
or not to treat high BP.
tension per 10 000 person-years could be attributed to oralcontraceptive use. Controlled prospective studies have dem-
Choice of Antihypertensive Drugs for Women. While womengenerally respond to antihypertensive drugs similarly to men,
onstrated a return of BP to pretreatment levels within 3
some special considerations may dictate treatment choices for
months of discontinuing oral contraceptives, indicating that
women. ACEIs and ARBs are contraindicated for women
their BP effect is readily reversible.
who are or intend to become pregnant because of the risk of
Oral contraceptives occasionally may precipitate acceler-
fetal developmental abnormalities. Diuretics are particularly
ated or malignant hypertension. Family history of hyperten-
useful in elderly individuals because of a decreased risk of hip
sion, including preexisting pregnancy-induced hypertension,
fracture. Some antihypertensive drugs have gender-specific
occult renal disease, obesity, middle age (⬎35 years), and
adverse effect profiles. For example, in the TOMHS study,
duration of oral contraceptive use increase susceptibility to
women reported twice as many adverse effects as men.305
hypertension. Contraceptive-induced hypertension appears to
Women are more likely to develop diuretic-induced hypona-
be related to the progestogenic, not the estrogenic, potency of
tremia, and men more likely to develop gout. Hypokalemia is
the preparation.
more common in women taking a diuretic. ACEI-induced
Regular monitoring of BP throughout contraceptive ther-
cough is twice as common in women as in men, and women
apy is recommended, and it has been suggested that contra-
are more likely to complain of CCB-related peripheral edema
ceptive prescriptions be limited to 6 months to ensure at least
and minoxidil-induced hirsutism.
semiannual reevaluations. Withdrawal of the offending con-traceptive agent is generally desirable in cases of
Pregnant Women
contraceptive-induced hypertension, but such therapy may
Hypertensive disorders in pregnancy are a major cause of
have to be continued in some women (eg, if other contracep-
maternal, fetal, and neonatal morbidity and mortality. Hyper-
tive methods are not suitable) and combined with antihyper-
tension in pregnancy is classified into 1 of 5 categories (Table
tensive therapy.
19), and it is critical to differentiate preeclampsia, a
Outcomes of Antihypertensive Trials in Women. Relative
pregnancy-specific syndrome of exaggerated vasoconstric-
benefits of antihypertensive therapy do not appear to differ
tion and reduced organ perfusion, from pre-existing chronic
between the sexes.303 Absolute risk reduction for stroke was
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 20.
Treatment of Chronic Hypertension in Pregnancy
Preferred on the basis of long-term follow-up studies supportingsafety
Reports of intrauterine growth retardation (atenolol)
Increasingly preferred to methyldopa because of reduced sideeffects
Calcium antagonists
No increase in major teratogenicity with exposure
Not first-line agents
ACEIs, angiotensin II
receptor antagonists
Reported fetal toxicity and death
ACEIs indicate angiotensin-converting enzyme inhibitor; BBs, beta blockers.
Prepregnancy Assessment. Women should be evaluated prior
sive medications while maintaining close observation, includ-
to conception to define their BP status, and, if hypertensive,
ing use of home BP monitoring. This approach reflects
to assess its severity, possible secondary causes, and presence
concern about the safety of antihypertensive drug treatment in
of target organ damage and to plan treatment strategies. Many
pregnancy. A meta-analysis of 45 randomized controlled
hypertensive women who plan to become pregnant should be
studies of treatment with several classes of antihypertensive
screened for pheochromocytoma because of the high morbid-
drugs in Stage 1 and 2 hypertension in pregnancy showed a
ity and mortality of this condition if not diagnosed antepar-
direct linear relationship between treatment-induced fall in
tum. In hypertensive women planning to become pregnant, it
mean arterial pressure and the proportion of small-for-
may be prudent prior to conception to change to antihyper-
gestational-age infants.307 This relationship was independent
tensive medications known to be safe during pregnancy, such
of type of hypertension, type of antihypertensive agent, and
as methyldopa or BBs. ACEIs and ARBs should be discon-
duration of therapy.
tinued prior to attempts at conception or as soon as pregnancy
However, for pregnant women with target organ damage or
is confirmed. Those with progressive renal diseases should be
a prior requirement for multiple antihypertensive agents for
encouraged to complete their childbearing while their renal
BP control, antihypertensive medication should be continued
function is relatively well preserved. Mild renal disease
as needed to control BP. In all cases, treatment should be
(serum creatinine ⬍1.4 mg/dL) has a minimal effect on fetal
reinstituted once BP reaches 150 to 160 mm Hg systolic or
survival, and the underlying renal disease does not generally
100 to 110 mm Hg diastolic, in order to prevent increases in
worsen during pregnancy. However, moderate or severe renal
BP to very high levels during pregnancy. Aggressive treat-
insufficiency in pregnancy may accelerate both hypertension
ment of severe chronic hypertension in the first trimester is
and the underlying disease and markedly reduce fetal
critical, since fetal loss rates of 50% and significant maternal
mortality have been reported in these patients.308 Most of thepoor outcomes are related to superimposed preeclampsia
Treatment of Chronic Hypertension During Pregnancy.
(Table 19). Further, women with chronic hypertension are
Women with Stage 1 hypertension are at low risk for cardiovas-
also at higher risk for adverse neonatal outcomes if protein-
cular complications during pregnancy and are candidates for
uria is present early in pregnancy. Fetal loss and acceleration
lifestyle modification therapy only, as there is no evidence that
of maternal renal disease increase at serum creatinine levels
pharmacological treatment improves neonatal outcomes. Fur-
⬎1.4 mg/dL at conception.
ther, BP usually falls during the first half of pregnancy; there-
Antihypertensive Drug Selection. The primary goal of treat-
fore, hypertension may be easier to control with reduced or no
ing chronic hypertension in pregnancy is to reduce maternal
medications. With lifestyle modification, aerobic exercise
risk, but the choice of antihypertensive agent(s) is largely
should be restricted on the basis of theoretical concerns that
driven by the safety of the fetus. Methyldopa is preferred by
inadequate placental blood flow may increase the risk of
many as first-line therapy, based on reports of stable utero-
preeclampsia, and weight reduction should not be attempted,
placental blood flow and fetal hemodynamics and the absence
even in obese pregnant women. Although the data on pregnant
of long-term (7.5-year follow-up) adverse effects on devel-
women are sparse, many experts recommend restriction of
opment of children exposed to methyldopa in utero.309,310
sodium intake to the same 2.4 g sodium intake recommended for
Other treatment options are summarized in Table 20.
those with primary hypertension.7 Use of alcohol and tobaccomust be strongly discouraged. Use of antihypertensive drugs
Preeclampsia. Preeclampsia is more common in women with
in pregnant women with chronic hypertension varies greatly
chronic hypertension, with an incidence of approximately
among centers. Some clinicians prefer to stop antihyperten-
25%. Risk factors for superimposed preeclampsia include
TABLE 21.
Treatment of Acute Severe Hypertension in Preeclampsia
5 mg IV bolus, then 10 mg every 20 to 30 minutes to a maximum of25 mg, repeat in several hours as necessary
Labetalol (second-line)
20 mg IV bolus, then 40 mg 10 minutes later, 80 mg every 10 minutesfor 2 additional doses to a maximum of 220 mg
10 mg PO, repeat every 20 minutes to a maximum of 30 mg
Caution when using nifedipine with magnesium sulfate, can seeprecipitous BP drop
Short-acting nifedipine is not approved by US Food and DrugAdministration for managing hypertension
Sodium nitroprusside
0.25 g/kg/min to a maximum of 5 g/kg/min
(rarely when others fail)
Fetal cyanide poisoning may occur if used for more than 4 hours
renal insufficiency, a history of hypertension for 4 years or
might be prudent to withhold antihypertensive medication,
longer, and hypertension in a previous pregnancy. Prevention
with close monitoring of BP, and reinstitute antihypertensive
of preeclampsia relies on identification of high-risk women
therapy following discontinuation of nursing. No short-term
and close clinical and laboratory monitoring aimed at its early
adverse effects have been reported from exposure to methyl-
recognition, and institution of intensive monitoring or deliv-
dopa or hydralazine. Propanolol and labetalol are preferred if
ery when indicated. Treatment of preeclampsia includes
a BB is indicated. ACEIs and ARBs should be avoided on the
hospitalization for bed rest, control of BP, seizure prophy-
basis of reports of adverse fetal and neonatal renal effects.
laxis in the presence of signs of impending eclampsia, and
Diuretics may reduce milk volume and thereby suppress
timely delivery. Importantly, many women with preeclampsia
lactation. Breast-fed infants of mothers taking antihyperten-
have previously been normotensive, so acute BP elevations
sive agents should be closely monitored for potential adverse
even to modest levels (ie, 150/100 mm Hg) may cause
significant symptomatology and require treatment. Treatment
Recurrence of Hypertension. Hypertension recurs in a large
does not alter the underlying pathophysiology of the disease,
proportion (20% to 50%) of subsequent pregnancies. Risk
but it may slow its progression and provide time for fetal
factors for recurrence include early onset of hypertension in
maturation. Preeclampsia rarely remits spontaneously and in
the first pregnancy, a history of chronic hypertension, persis-
most cases worsens with time.
tent hypertension beyond 5 weeks postpartum, and elevated
While delivery may be appropriate therapy for the mother,
it may compromise a fetus of less than 32 weeks gestation.
BP early in pregnancy. Women with preeclampsia have a
Regardless of gestational age, delivery should be strongly
greater tendency to develop hypertension than those with
considered when there are signs of fetal distress or intrauter-
ine growth retardation or signs of maternal problems, includ-
Hypertension in Children and Adolescents
ing severe hypertension, hemolysis, elevated liver enzymes,
In children and adolescents, hypertension is defined as
low platelet count, deteriorating renal function, visual distur-
elevated BP that persists on repeated measurement at the 95th
bance, headache, or epigastric pain. Vaginal delivery is
percentile or greater for age, height, and gender (Table 22).
preferable to cesarean delivery to avoid the added stress of
As with adults, the fifth Korotkoff sound is used to define
Clinicians should be alert to the possibility of identifiable
Antihypertensive Drug Therapy. Antihypertensive therapy
causes of hypertension in younger children. Secondary forms
should be prescribed only for maternal safety; it does not
of hypertension are more common in children and in individ-
improve perinatal outcomes and may adversely affect utero-
uals with severe hypertension (⬎20 mm Hg above the 95th
placental blood flow. Selection of antihypertensive agents
percentile). Chronic hypertension is becoming increasingly
and route of administration depends on anticipated timing of
common in adolescence and is generally associated with
delivery. If delivery is likely more than 48 hours off, oral
obesity, sedentary lifestyle, and a positive family history of
methyldopa is preferred because of its safety record. Oral
hypertension and other CVDs. Like adults, children and
labetalol is an alternative, and other BBs and calcium antag-
adolescents with established hypertension develop target
onists are also acceptable on the basis of limited data (Table
organ damage, including LVH. Appropriate assessment for
20). If delivery is imminent, parenteral agents are practical
LVH, including echocardiography, should be considered in
and effective (Table 21). Antihypertensives are administered
children who have significant and persisting hypertension.
before induction of labor for persistent DBPs of 105 to
Lifestyle interventions should be recommended for all
110 mm Hg or higher, aiming for levels of 95 to 105 mm Hg.
children with hypertension, with pharmacological therapy
Treating Hypertension During Lactation. Hypertensive
instituted for higher levels of BP or if insufficient response to
mothers can usually breast-feed safely. However, all antihy-
lifestyle modifications occurs. Teenage children with BP
pertensive drugs that have been studied are excreted into
below but near the 95th percentile should adopt healthy
human breast milk. Therefore, in mothers with stage 1
lifestyles similar to adults with prehypertension. Although the
hypertension who wish to breast-feed for a few months, it
recommendations for drug choices are generally similar in
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 22.
95th Percentile of Blood Pressure by Selected Ages, by the 50th and
75th Height Percentiles, and by Gender in Children and Adolescents
Source: Adapted from Update on the 1987 Task Force Report on High Blood Pressure in Children
and Adolescents: A working group report from the National High Blood Pressure Education Program.
Pediatrics. 1996;98:649 – 658.
children and adults, dosages of antihypertensive medication
to reduce mean arterial BP by no more than 25% (within
for children should be smaller and adjusted very carefully.
minutes to 1 hour), then, if stable, to 160/100 to 110 mm Hg
ACEIs and ARBs should not be used if the patient is
within the next 2 to 6 hours. Excessive falls in pressure that
pregnant. These agents should be used with extreme caution
may precipitate renal, cerebral, or coronary ischemia should
in sexually active teenage girls and only when careful
be avoided. For this reason, short-acting nifedipine is no
counseling and effective pregnancy precautions are
longer considered acceptable in the initial treatment of
hypertensive emergencies or urgencies. If this level of BP is
The presence of uncomplicated hypertension should not be
well tolerated and the patient is clinically stable, further
a reason to restrict children from participating in physical
gradual reductions toward a normal BP can be implemented
activities, particularly because exercise may lower BP. Use of
in the next 24 to 48 hours. There are exceptions to the above
anabolic steroid hormones for the purpose of bodybuilding
recommendation—patients with an ischemic stroke in which
should be strongly discouraged. Efforts should be made to
there is no clear evidence from clinical trials to support the
identify other modifiable risk factors in children (eg, obesity,
use of immediate antihypertensive treatment, patients with
lack of physical activity, smoking), and vigorous interven-
aortic dissection who should have their SBP lowered to
tions should be made when present. Detailed recommenda-
⬍100 mm Hg if tolerated, and patients in whom BP is
tions regarding hypertension in children and adolescents can
lowered to enable the use of thrombolytic agents (see the
be found in the 1996 NHBPEP Working Group Report on
section on stroke).
Hypertension Control in Children and Adolescents.311
Some patients with hypertensive urgencies may benefit
from treatment with an oral, short-acting agent such as
Hypertensive Crises: Emergencies and Urgencies
captopril, labetalol, or clonidine followed by several hours of
Hypertensive emergencies are characterized by severe eleva-
observation. However, there is no evidence to suggest that
tions in BP (⬎180/120 mm Hg) complicated by evidence of
failure to aggressively lower BP in the emergency room is
impending or progressive target organ dysfunction. They
associated with any increased short-term risk to the patient
require immediate BP reduction (not necessarily to normal) to
who presents with severe hypertension. Such a patient may
prevent or limit target organ damage.312,313 Examples include
also benefit from adjustment in their antihypertensive ther-
hypertensive encephalopathy, intracerebral hemorrhage,
apy, particularly the use of combination drugs, or reinstitution
acute myocardial infarction, acute left ventricular failure with
of medications if noncompliance is a problem. Most impor-
pulmonary edema, unstable angina pectoris, dissecting aortic
tantly, patients should not leave the emergency room without
aneurysm, or eclampsia. Hypertensive urgencies are those
a confirmed follow-up visit within 1 to a few days.
situations associated with severe elevations in BP without
Unfortunately, the term "urgency" has led to overly ag-
progressive target organ dysfunction. Examples include upper
gressive management of many patients with severe, uncom-
levels of stage II hypertension associated with severe head-
plicated hypertension. Aggressive dosing with intravenous
ache, shortness of breath, epistaxis, or severe anxiety. The
drugs or even oral agents to rapidly lower BP is not without
majority of these patients present as noncompliant or inade-
risk. Oral loading doses of antihypertensive agents can lead to
quately treated hypertensives, often with little or no evidence
cumulative effects causing hypotension, sometimes following
of target organ damage.
discharge from the emergency room. Patients who continue to
Early triage to establish the appropriate therapeutic strate-
be noncompliant will often return to the emergency room
gies for these patients is critical to limiting morbidity and
within weeks.
mortality.314 Patients presenting with severe hypertensionmay represent as much as 25% of all patient visits to busy
Erectile Dysfunction and Hypertension
urban emergency rooms.315
Erectile dysfunction (ED), defined as the inability to have and
Patients with a hypertensive emergency should be admitted
maintain an erection adequate for intercourse, becomes in-
to an Intensive Care Unit for continuous monitoring of BP
creasingly common in men over 50 years old and is even
and parenteral administration of an appropriate agent (Table
more common if they are hypertensive.316 In a survey of over
23). The initial goal of therapy in hypertensive emergencies is
3000 health professionals, the frequency of ED was 4% in
TABLE 23.
Parenteral Drugs for Treatment of Hypertensive Emergencies*
Adverse Effects†
Special Indications
0.25–10 g/kg/min as IV
Nausea, vomiting, muscle
Most hypertensive
twitching, sweating, thiocynate and
emergencies; caution with
cyanide intoxication
high intracranial pressure orazotemia
Tachycardia, headache, flushing,
Most hypertensive
emergencies except acute
heart failure; caution withcoronary ischemia
0.1–0.3 g/kg per min IV
Tachycardia, headache, nausea,
Most hypertensive
emergencies; caution withglaucoma
5–100 g/min as IV infusion§
Headache, vomiting,
Coronary ischemia
methemoglobinemia, tolerancewith prolonged use
1.25–5 mg every 6 h IV
Precipitous fall in pressure in
Acute left ventricular failure;
high-renin states; variable
avoid in acute myocardial
Tachycardia, flushing, headache,
vomiting, aggravation of angina
Adrenergic inhibitors
20–80 mg IV bolus every 10 min
Vomiting, scalp tingling,
Most hypertensive
emergencies except acute
nausea, heart block, orthostatic
0.5–2.0 mg/min IV infusion
250–500 g/kg/min IV bolus,
Hypotension, nausea, asthma,
Aortic dissection,
then 50–100 g/kg/min by
first-degree heart block, HF
infusion; may repeat bolus after5 min or increase infusion to300 g/min
5–15 mg IV bolus
Tachycardia, flushing, headache
Catecholamine excess
*These doses may vary from those in the Physicians' Desk Reference (51st edition).
†Hypotension may occur with all agents.
‡Requires special delivery system.
men under age 50, 26% in those 50 to 59, and 40% in those
between a CCB, ACEI, hydrochlorothiazide, or BB compared
60 to 69.316 The frequency was significantly higher if they
with placebo.103 In other studies, centrally acting ␣-agonists
were hypertensive, diabetic, obese, or smokers or were taking
have been associated with ED, while ACEIs, ARBs, and
antidepressants or BBs.
CCBs have not been observed to increase its incidence.317,318
Whereas hypertension per se may be associated with
A lower risk of ED was reported among men who were
ED,317 the use of various antihypertensive medications may
physically active, not obese, and nonsmokers.316 Therefore,
increase the incidence, in part because BP lowering itself may
lifestyle modifications should be encouraged to forestall ED.
cause reduction of perfusion of genital organs. Available data
If ED appears after institution of antihypertensive drug
regarding individual effects of antihypertensive drug therapy
therapy, the offending agent should be discontinued and
are confounded by age, vascular disease, and hormonal status.
treatment restarted with another agent. Sildenafil or other
In the TOMHS study involving antihypertensive drugs from
phosphodiesterase-5 inhibitors may be prescribed without a
five different classes (excluding ARBs), participants random-
significant likelihood of adverse reactions in those with
ized to chlorthalidone reported a significantly higher inci-
concomitant antihypertensive therapy so long as nitrates are
dence of erection problems at 24 months of the study than
participants randomized to placebo. Incidence rates through
There are no definitive data on a relation between sexual
48 months were more similar among treatment groups than at
dysfunction and hypertension in women. Regardless of gen-
24 months, with nonsignificant differences between chlortha-
der, clinicians should be willing to discuss sexual dysfunction
lidone and placebo groups.123 In the VA Cooperative trial, no
problems and offer counseling to improve the patient's
difference in incidence of sexual dysfunction was noted
quality of life.
Chobanian et al
JNC 7 – COMPLETE REPORT
Urinary Outflow Obstruction
monitored closely in the dental office if general anesthesia is
Symptoms of urinary outflow obstruction or a known history
administered to hypertensives because of potential wide
of obstruction should be elicited as part of the hypertension
fluctuations in BP and the risk of hypotension in those
workup. When a normal bladder is distended beyond approx-
receiving antihypertensive drugs. CCBs and other vasodila-
imately 300 mL, sympathetic nervous system stimulation
tors may cause hypertrophy of the gums.
may cause a substantial increase in BP. Patients with highspinal cord injuries in particular may exhibit large acute BP
Obstructive Sleep Apnea
Obstructive sleep apnea (OSA) occurs in 2% to 4% of the
increases similar to individuals with autonomic dysfunction.
adult population, and over 50% of individuals with OSA have
BP control can be improved by keeping the bladder volume
hypertension.263,326–333 Obesity is so common in OSA that the
below 300 mL and by the use of sympatholytic drugs.
index of suspicion for OSA should be high in any hyperten-
Nonsurgical treatment of patients with urinary outflow ob-
sive patient whose BMI is above 27 kg/m2.331 These individ-
struction includes the use of ␣1-blockers such as terazosin,
uals should be questioned thoroughly for symptoms of OSA,
doxazosin, or prazosin, which indirectly dilate prostatic and
including snoring, witnessed apnea, irregular breathing dur-
urinary sphincter smooth muscle and also lower BP.320
ing sleep, restless sleeping, and chronic morning fatigue.
Patients Undergoing Surgery
Frequently it is the sleep partner who provides the most
Uncontrolled hypertension is associated with wider fluctua-
reliable history, especially regarding snoring, because the
tions of BP during induction of anesthesia and intubation and
affected individual may deny or be unaware of the problem.
may increase the risk for perioperative ischemic events. BP
If the diagnosis is suspected clinically, confirmation by a
levels of 180/110 mm Hg or greater should be controlled
formal sleep study is indicated. The impact of sleep apnea on
prior to surgery.321 For elective surgery, effective BP control
CVD is probably related in large part to its association with
can be achieved over several days to weeks of outpatient
elevated BP. However, OSA may act through a number of
treatment. In urgent situations, rapidly acting parenteral
mechanisms to elicit myocardial and vascular damage, in-
agents such as sodium nitroprusside, nicardipine, and labe-
cluding increase in catecholamine release,333,334 activation of
talol can be utilized to attain effective control very rapidly.
inflammatory mechanisms,335 insulin resistance,336,337 andendothelial dysfunction.338 Other cardiovascular conditions
Surgical candidates with controlled hypertension should
associated with OSA include arrhythmias, HF, myocardial
maintain their medications until the time of surgery, and
infarction, and stroke.331,332,339–344
therapy should be reinstated as soon as possible post-
Previous debate about whether OSA is an etiologic factor
operatively. Adequate potassium supplementation should be
in hypertension has focused largely around the strong asso-
provided, if needed, to correct hypokalemia well in advance
ciation of OSA with obesity. While obesity is known to
of surgery. Older patients may gain particular benefit from
contribute in large part to OSA,345–348 patients with OSA may
treatment with 1-selective BBs before and during the peri-
also be at increased risk for weight gain,349 and treatment of
operative period.322
OSA may reduce visceral fat.350 It now appears that the
Sudden intraoperative hypertension is managed by many of
potential causal association between OSA and hypertension
the same parenteral antihypertensive agents that are utilized
involves both the obesity-hypertension link and an indepen-
in the management of hypertensive emergencies (see the
dent role of OSA in chronic BP elevation. Episodes of apnea
section on emergencies and urgencies).323 Intravenous infu-
with repeated oxygen desaturation in OSA have been shown
sions of sodium nitroprusside, nicardipine, and labetalol can
to stimulate strong sympathetic nervous system discharges
be effective. Nitroglycerin is often an agent of choice in
that directly elevate BP.333,334 Poorer quality of sleep and
patients with coronary ischemia, while the very short-acting
shorter sleep periods may play a reinforcing role in the fatigue
BB esmolol may be of benefit in managing intraoperative
and daytime somnolence. Sleep deprivation alone may raise
BP351 and impair glucose tolerance.352 There is also a direct
Hypertension is very common in the early postoperative
relationship between the severity of sleep apnea and the level
period, related to increased sympathetic tone and vascular
of BP. Finally, sustained and effective treatment of OSA with
resistance.324 Contributing factors include pain and increased
continuous positive airway pressure (CPAP) has been re-
intravascular volume, which may require parenteral dosing
ported to lower nighttime and daytime BP in hypertensives
with a loop diuretic such as furosemide. If resumption of oral
with OSA.353–355
treatment must be interrupted postoperatively, periodic dos-
In addition to weight loss, improvements in the quality of
ing with intravenous enalaprilat or transdermal clonidine
sleep in OSA patients can occur as a result of a variety of
hydrochloride may be useful.
positioning measures during sleep, particularly sleeping onone's side. Treatment with CPAP can be useful in overall BP
Dental Issues in the Hypertensive Subjects
lowering and may also improve cardiac ischemia356,357 and
A concern in dental care is the use of epinephrine in local
HF symptoms.331,332 The role of oral prostheses and surgical
anesthetic solutions. Many dental providers do not use
approaches remains to be fully defined.354 No specific class
catecholamine-containing local anesthetic formulations for
of antihypertensive drugs has yet been demonstrated to be
any patient with elevated BP, as they are concerned with an
superior for BP lowering in OSA patients.354
adverse cardiovascular response. A systematic review of thistopic325 concluded that although adverse events may occur in
Hypertension and the Eye
uncontrolled hypertensive patients during dental procedures,
Hypertension can effect the retina, choroid, and optic nerve of
the use of epinephrine had a minimal effect. BP should be
the eye, particularly with stage 2 hypertension. These changes
can be appreciated with inspection of the retinal vessels by direct
ally, renal artery stenosis can lead to reduced kidney function
ophthalmoscopy, photography, or angiography.
Hypertensive retinopathy is most commonly manifested by
Clinical clues to renovascular disease include (1) onset of
generalized or focal narrowing of retinal arterioles. In acute
hypertension before age 30 (especially without a family
or advanced hypertension, the retinal vasculature may be
history) or recent onset of significant hypertension after age
injured sufficiently to cause occlusion or leakage. These
55; (2) an abdominal bruit, particularly if it continues into
changes may be manifested as nerve fiber layer infarcts (soft
diastole and is lateralized; (3) accelerated or resistant hyper-
exudates or cotton-wool patches), extravascular edema (hard
tension; (4) recurrent (flash) pulmonary edema; (5) renal
exudates), intraretinal hemorrhages, and retinal arterial
failure of uncertain etiology, especially with a normal urinary
sediment; (6) coexisting diffuse atherosclerotic vascular dis-
Hypertensive choroidopathy is most frequently seen in
ease, especially in heavy smokers; or (7) acute renal failure
young patients with acute hypertension, including cases of
precipitated by antihypertensive therapy, particularly ACEIs
eclampsia or pheochromocytoma. Findings include Elschnig
In patients with indications of renovascular disease, captopril-
spots (nonperfused areas of the choriocapillaris) and Siegrist
enhanced radionuclide renal scan, duplex Doppler flow studies,
streaks (linear hyperpigmentation over choroidal arteries).
and magnetic resonance angiography may be used as noninva-
Hypertensive optic neuropathy occurring with severe hy-
sive screening tests. Three-dimensional images can be obtained
pertension may present with flame hemorrhages, optic disc
by spiral computed tomography, a technique that necessitates the
edema, venous congestion, and macular exudates.358–360
use of intravenous contrast.81 Definitive diagnosis of renovascu-
lar disease requires renal angiography, which carries some risk,
Hypertension is a relatively common occurrence in patients
particularly of radiocontrast-induced acute renal failure or
receiving organ transplants; in those receiving kidney allo-
grafts, the prevalence of hypertension probably exceeds
In patients, usually women, with fibromuscular dysplasia,
65%.361 Nocturnal hypertension, a reversal of diurnal BP
results of percutaneous transluminal renal angioplasty
rhythm, may be present in these individuals who may need
(PTRA) have been excellent and comparable to surgical
ABPM to evaluate overall BP control. Hypertension is less
revascularization.365 Patients with normal renal function and
common in other forms of transplantation. The mechanisms
atherosclerotic renal artery stenosis that is focal, unilateral,
of hypertension in transplant patients are multifactorial, but
and nonostial also may be managed by angioplasty.365 Renal
vasoconstriction and long-term vascular structural changes
artery stenting has become an important adjunct to PTRA,
caused by chronic immunosuppressive drugs that are cal-
being used to counteract elastic recoil and to abolish theresidual stenosis often observed after PTRA.366
cineurin inhibitors (cyclosporine and tacrolimus) and corti-
Even though many patients with high-grade renal artery
costeroids are among the most important.362 Impaired renal
stenosis remain stable for prolonged periods if BP is well
function is another exacerbating factor; despite successful
controlled,367 surgical revascularization or PTRA with renal
renal transplantation, most patients have enough impairment
artery stenting may be needed to preserve renal function.81
in renal function to cause relative salt and water retention.
Transplant renal artery stenosis may also be a factor.
Drugs and Other Agents Affecting
Observational studies suggest that hypertension correlates
with deterioration in graft function. Large-scale, controlled
Many prescription drugs and some over-the-counter agents
clinical trials on the effects of BP control on GFR decline or
and herbal supplements may affect BP and complicate BP
on CVD incidence are lacking in this population. The high
control in treated hypertensives. Consequently, searching for
risk of graft occlusion and cardiovascular events has sug-
the presence of these agents in the medical history can
gested that BP should be lowered to 130/80 mm Hg or less.
identify a secondary component contributing to BP elevation.
Because of the absence of compelling data, no particular class
Such recognition may negate the need to employ unnecessary
of antihypertensives can be considered to be superior to any
and potentially hazardous testing.
other. The difficulty of lowering BP in this group makes
Use of agents that can affect BP in a given patient should
combination drugs necessary in almost all patients. As with
be suspected in the following situations: (1) loss of control of
other renal diseases, serum creatinine and potassium should
previously well-controlled hypertension, (2) presence of co-
be monitored 1 to 2 weeks following initiation or escalation
morbidities (particularly osteoarthritis), (3) biochemical evi-
in therapy with ACEIs or ARBs. A greater than 1 mg/dL
dence of intercurrent drug usage (such as an increase in serum
increase in serum creatinine should raise the question of renal
potassium or creatinine concentrations with nonsteroidal
artery stenosis.
anti-inflammatory drugs), and (4) atypical hypertension (suchas severe but transient hypertension in a young patient
Patients with Renovascular Disease
presenting with chest pain and ECG changes accompanying
Hemodynamically significant renal artery stenosis may be
possible cocaine usage).
associated with all stages of hypertension, but it is more
Table 24 provides a list of those agents that may alter BP.
commonly recognized in patients with stage 2 or resistant
They may affect BP in several ways. They may affect sodium
hypertension, since these are the individuals in whom special
balance; increase adrenergic or suppress parasympathetic
evaluation for the problem is carried out. If present bilater-
neural activity; alter the production, release, or effectiveness
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 24.
Common Substances Associated With Hypertension
tensive subjects.10 The use of ambulatory BP monitoring has
in Humans
highlighted the biphasic effects of alcohol on BP, underscor-ing the importance of the timing of BP measurement. A large
Prescription Drugs
intake of alcohol (⬎30 g) may lower BP in the first 4 hours
Cortisone and other steroids (both cortico- and mineralo-), ACTH
after ingestion. Approximately 10 to 15 hours later (perhaps
Estrogens (usually just oral contraceptive agents with high estrogenic
at the time a patient is seen for an office visit or in the
emergency room during withdrawal), BP increase may be
Nonsteroidal anti-inflammatory drugs
noted. This accounts for some of the discrepancies reported in
Phenylpropanolamines and analogues
the literature about alcohol's effect on BP. The mechanism(s)
Cyclosporine and tacrolimus
of alcohol's effect on BP are unclear but appear to result
predominantly from sympathetic neural activation, although
changes in cortisol and cellular calcium concentrations alsomay play a role.
NANSAIDs represent one of the most common medication
classes consumed by hypertensive patients. Among the NAN-
Antidepressants (especially venlafaxine)
SAIDs, older agents like indomethacin are the most exten-
sively studied. BP responses vary within the class of theNANSAIDs; however, increases in pressure are often accom-
Clonidine, BB combination
panied by peripheral edema and weight gain, supporting a
Pheochromocytoma: BB without ␣-blocker first; glucagon
salt-retention mechanism of hypertension associated with the
loss of natriuretic prostaglandins such as PGE2.368,369 Reduc-
Street drugs and other "natural products"
tion in the well-described vasodilatory effects of some pros-
Cocaine and cocaine withdrawal
taglandins is another mechanism. COX-2 inhibitors also may
Ma huang, "herbal ecstasy," and other phenylpropanolamine
cause elevation in BP.370–372 Recently, a double-blind ran-
domized trial was conducted evaluating the effects of cele-
Nicotine and withdrawal
coxib, rofecoxib, and naproxen on 24-hour BP in type 2
Anabolic steroids
diabetic patients with osteoarthritis whose hypertension was
Narcotic withdrawal
treated with ACEIs or ARBs. At equally efficacious doses forthe management of osteoarthritis, treatment with rofecoxib,
but not celecoxib or naproxen, induced a significant increase
in average 24-hour SBP in type 2 diabetic patients receiving
ACEIs or angiotensin II receptor blockers.373 Thus, current
Ergotamine and other ergot-containing herbal preparations
data suggest that certain NSAIDs and COX 2 inhibitors may
have destabilizing effects on BP control in diabetic hyperten-
sive patients. This is a major concern, as diabetic patients are
often older and obese, and both obesity and aging predisposeto osteoarthritis as well as diabetes.
Improving Hypertension Control
Tyramine-containing foods (with MAO-I)
Issues Dealing with Adherence to Regimens
Chemical elements and other industrial chemicals
Behavioral models suggest that the most effective therapy
prescribed by the most careful clinician will control hyper-
tension only if the patient is motivated to take the medication
Thallium and other heavy metals
as directed and to establish and maintain a health-promoting
Lithium salts, especially the chloride
lifestyle. Motivation improves when patients have positive
Boldfaced items within the list represent the substances of more current
TABLE 25.
Provide Empathetic Reinforcement
Adopt an attitude of concern coupled with hope and interest in the patient's
of vasoactive hormones; or exert direct effects on the endo-
thelium or vascular smooth muscle.
Provide positive feedback for BP and behavioral improvement
If BP is not at goal, ask about behaviors to achieve BP control
Alcohol
Modest consumption of alcohol (eg, ⬍30 g of ethanol a day
Hold exit interviews to clarify regimen. A patient may tell you that theyunderstand but tell the exit interviewer that they do not.
or approximately two drinks daily) is not generally associatedwith BP increases. Larger amounts of alcohol ingestion have
Schedule more frequent appointments and health care personnel contactwith patients who are not achieving goal BP
a dose-related effect on BP, both in hypertensive and normo-
TABLE 26.
Clinician Awareness and Monitoring
TABLE 28.
Patient Education About Treatment
Anticipate adherence problems for young men
Assess patient's understanding and acceptance of the diagnosis of
Consider nonadherence as a cause of
Failure to reach goal BP
Discuss patient's concerns and clarify misunderstandings
Resistant hypertension
Tell patient the BP reading and provide a written copy
Sudden loss of control
Come to agreement with the patient on goal BP
Encourage patients to bring in all medications from all physicians and other
Ask patient to rate (1 to 10) his or her chance of staying on treatment
sources, whether prescription, complementary, or over-the-counter, to each
Inform patient about recommended treatment and provide specific written
visit for review and to rule out iatrogenic causes of elevated blood pressure
information about the role of lifestyle including diet, physical activity, dietary
Ask what the patient takes for pain
supplements, and alcohol intake. Use standard brochures when available.
Recognize depression and other psychiatric illnesses, including panic
Elicit concerns and questions and provide opportunities for the patient to
attacks, and manage appropriately
state specific behaviors to carry out treatment recommendations
Be willing to change unsuccessful regimens and search for those more
likely to succeed
Need to continue treatment
Control does not mean cure
One cannot tell if BP is elevated by feeling or symptoms; BP must be
experiences with, and trust in, their clinicians. Better com-
munication improves outcomes. Empathy builds trust and is apotent motivator (Table 25).374
care managers, outside auditors) can be very effective in not
What Can the Clinician Do?
only helping to achieve BP goals but to alert clinicians to
Clinician-patient partnerships that are based on trust, respect,
missed patient appointments, necessary prescription refills,
and a holistic knowledge of the patient correlate with positive
and laboratory abnormalities.377
outcomes of care: adherence, satisfaction, and improved
Patient-centered behavioral interventions such as counsel-
health status. Patients often evaluate a clinician's competence
ing improve BP control (Table 28).378 Nurse clinicians and
by their customer service skills, not their clinical skills.375
pharmacists have proven their effectiveness in helping to
Customer service includes ease of access, minimal waiting
achieve goal BP.379 Commercial health plans may provide
time, and a positive regard from the office staff; all are known
resources for chart auditing or other assistance to improve BP
to influence provider satisfaction and patient adherence.
control.380 Clinicians should periodically audit their own
Clinicians are the role model and should train staff by
patient files to assess their degree of compliance and success
providing a positive, interactive, empathetic environment.
with established goals and treatment interventions.
This will increase patient comfort and willingness to partic-
The National Committee for Quality Assurance (NCQA)
ipate in their own care.
has established the Health Plan Employer Data and Informa-tion Set (HEDIS), a set of standardized performance mea-
Clinical Inertia
There is a broad range of clinician commitment to optimal
sures designed to ensure that purchasers and consumers have
hypertension therapy (Table 26). Failure to titrate or combine
the information they need to reliably assess quality of health
medications and to reinforce lifestyle modifications despite
knowing that the patient is not at goal BP represents clinical
of HEDIS guidelines by managed care organizations has
inertia that must be overcome. This may be due in part to
successfully increased the appropriate use of ACEIs in HF
clinician focus on relieving symptoms, a lack of familiarity
and BBs in patients who have suffered a myocardial infarc-
with clinical guidelines, or discomfort in titrating to a goal.376
tion. NCQA now monitors physician records for the percent
A number of approaches are available to overcome clinical
of patients whose BP is less than 140/90 mm Hg.381 BP
inertia. One of the most effective is to use decision support
control rates by physicians so monitored have increased to as
systems that prompt the clinician to advance therapy when a
high as 59%. Patients should be told their BP on each visit
goal has not been achieved (Table 27). Such systems can be
and be encouraged not only to ask for those numbers but to
electronic (computer- or PDA-based) or paper-based (flow
inquire as to why BP is above the goal, if that is the case.
charts, algorithms, guidelines). Feedback reminders from any
They also should be given a written record to keep as their
source (computer-based, automated telephone-based, nurse
part of this commitment.
Role of Other Healthcare Professionals
TABLE 27.
Organize Care Delivery Systems
Clinicians must work with other healthcare professionals (eg,nurse case managers and other nurses, physician assistants,
Schedule next appointment before patient leaves office
pharmacists, dentists, registered dietitians, licensed nutrition-
Use appointment reminders, preferably computer-based, and contactpatients to confirm appointments
TABLE 29.
Collaborate With Other Health Professionals
Follow up patients who missed appointments
Use an office-based systems approach for monitoring and follow-up (eg,
Use complimentary skills and knowledge of nurses, physician assistants,
educate staff to provide patient encouragement, computer or chart
pharmacists, registered dietitians, optometrists, dentists, and podiatrists
reminders, disease management aids)
Refer selected patients for more intensive counseling
Chobanian et al
JNC 7 – COMPLETE REPORT
TABLE 30.
Individualize the Regimen
TABLE 31.
Promote Social Support Systems
Include patient in decision-making
With full permission of the patient, involve caring family members or other
Simplify the regimen to once-daily dosing, if possible
social support (ie, faith-based or community organizations) in the treatmentprocess
Incorporate treatment into patient's daily lifestyle; eg, take medications justbefore or after brushing teeth
Suggest common interest group activities (eg, a walking group) to enhancemutual support and motivation
Agree with the patient on realistic short-term objectives for specificcomponents of the medication and lifestyle modification plan
Encourage discussion of diet and physical activity
second group (16%) tended to rely on medication rather thanlifestyle to control their BP. The third group (22%) had the
Encourage discussion of adverse drug effects and concerns
highest BMI, did not practice health-promoting lifestyle
Encourage self-monitoring with validated BP devices
except for low rates of alcohol consumption and tobacco
Minimize the cost of therapy. Recognize financial issues and enlist local
abuse, often forgot to take their medication, and had a lower
community and national programs to assist in affording medications.
BP control rate. These patients may benefit most from clinical
Indicate that adherence to the regimen will be a subject of discussion at
counseling and help in achieving lifestyle modifications and
will likely require more frequent office visits or contact with
Encourage gradual sustained weight loss
nurses or other providers. The last group (23%) was morelikely to be male and young, knew less about hypertension,
ists, nutrition educators, optometrists, and podiatrists) to
was least afraid of consequences of hypertension or failure to
influence or reinforce instructions to improve patient life-
take their medication, and was most likely to consume
styles and BP control (Table 29). Nurse-managed hyperten-
alcohol, abuse tobacco, and stop medication without inform-
sion clinics, worksite Occupational Health departments, man-
ing their physician. They probably require persistent rein-
aged care organizations, pharmacists, and lay community
forcement, information on the hazards of lack of BP control,
workers have all contributed to better hypertension control.
and small incremental goal-setting by allied health care
Public health nurses and community outreach workers in
personnel. Involvement of family members or other social
high-risk communities also are helpful through their efforts to
supports also may be useful (Table 31).
screen, identify cases, refer and track follow-up appoint-
Goal Setting and Behavioral Change
ments, and educate patients. All health care professionals
The clinician and patient must agree on BP goals and
must be committed to enhancing BP control through reinforc-
estimated time to reach them, and those goals should be
ing messages about the risks of hypertension, the importance
clearly recorded in the chart. With the support of the clinician,
of managing both SBP and DBP and achieving goal BP,
the patient must be empowered with the understanding that
education about effective lifestyle interventions, pharmaco-
making behavioral changes is ultimately his or her responsi-
logical therapies, and adherence to treatment.
bility. As people make behavior change, they progress
through a series of stages (precontemplation, contemplation,
Patient attitudes are greatly influenced by cultural differ-
preparation, action, and maintenance). Behavior change is
ences, beliefs, and previous experiences with the health
more successfully facilitated using this approach along with
system.382 These attitudes must be understood and respected
motivational interviewing rather than assigning the same
if the clinician is to build trust and increase communication
intervention to every patient.384,385
with patients and families (Table 30). Clinicians should
Patients can be asked, using a 1 to 10 ranking, how likely
explain to patients that the terms "hypertension" and "high
they are to follow the plan. If not likely, the clinician can use
BP" are used interchangeably and that neither indicates an
motivational interviewing to identify the barriers to adher-
anxiety state. In addition to motivation, patients need specific
ence. At visits where BP is above goal, alterations in the
education designed to help them modify their lifestyle and to
treatment plan should be made and documented accordingly.
take medications as prescribed to feel better and to reduce
Home BP devices can be very useful in involving many
patients in their own care. Devices must be calibrated by theclinician (see the section Self Measurement). This should be
Characterization of Patients Leading to Tailored Therapy
done, in part, by having the patient determine their BP with
There is a broad range of patient involvement in, and
the device in the presence of the clinician. Home-determined
commitment to, hypertension therapy. Management strategies
BP tends to be approximately 5 mm Hg lower than office BP,
need to be focused on the patient's goals when providing
and this information should be considered when assessing
advice and encouraging adherence. Optimal management
progress toward goal. But office BP should still be used to
strategies are likely to differ for patient types. Healthy
determine that a patient is at goal.
lifestyles influence adherence to medication as well as pa-
Patient satisfaction with their health care providers predicts
tient's beliefs and involvement with behaviors including
compliance with treatment. All clinicians need to provide
food, beverages, physical activity, healthy weight, salt and
positive, patient-centered care to satisfy and enable their
alcohol consumption, and smoking. A cluster analysis of 727
patients to follow treatment. Some patient-centered behav-
hypertensive patients found that the individuals fell into 4
ioral interventions, like counseling, have been shown to
categories.383 The largest group (39%) was health-oriented,
improve BP control, while the evidence for structured train-
informed about hypertension, and took their medication. A
ing or self-monitoring is less clear.
Center, Chicago, Ill); Henry R. Black, MD (Rush University Medical
The cost of medications may be a barrier to effective
Center, Chicago, Ill); Vicki Burt, ScM, RN (National Center for
treatment. Patients often perceive that lifestyle modifications
Health Statistics, Hyattsville, Md); Barry L. Carter, PharmD, FCCP(University of Iowa, Iowa City, Iowa); Francis D. Chesley, Jr., MD
such as following the DASH eating plan are expensive, but
(Agency for Healthcare Research and Quality, Rockville, Md);
following these plans can be accomplished even on modest
Jerome D. Cohen, MD (Saint Louis University School of Medicine,
budgets. Nutrition educators offer classes in schools, com-
St. Louis, Mo); Pamela J. Colman, DPM (American Podiatric
munities, and worksites on food budgeting and meal plan-
Medical Association, Bethesda, Md); William C. Cushman, MD
ning. Clinicians should refer their patients to these classes.
(Veterans Affairs Medical Center, Memphis, Tenn); Mark J.
Medical nutrition therapy by registered dietitians improves
Cziraky, PharmD, FAHA (Health Core, Inc., Newark, Del); John J.
Davis, PAC (American Academy of Physician Assistants, Memphis,
the health of patients who have high cholesterol, diabetes,
Tenn); Keith Copelin Ferdinand, MD, FACC (Heartbeats Life
obesity, or other chronic disease risk factors.386 Patients
Center, New Orleans, La); Ray W. Gifford, Jr., MD, MS (Cleveland
should be advised that most lifestyle modifications may be
Clinic Foundation, Fountain Hills, Ariz); Michael Glick, DMD (New
cost-free or may even save money (eg, smoking cessation and
Jersey Dental School, Newark, NJ); Lee A. Green, MD, MPH
reduction of alcohol consumption). Further, the beneficial
(University of Michigan, Ann Arbor, Mich); Stephen Havas, MD,
effects of lifestyle modification may include reduction in the
MPH, MS (University of Maryland School of Medicine, Baltimore,Md); Thomas H. Hostetter, MD (National Institutes of Diabetes and
amount and cost of prescribed medications and the cost of
Digestive and Kidney Diseases, Bethesda, Md); Joseph L. Izzo, Jr.,
insurance. A patient adhering to the DASH eating plan may
MD (State University of New York at Buffalo School of Medicine,
require less medication and save money. Patients need to
Buffalo, NY); Daniel W. Jones, MD (University of Mississippi
understand the important difference between the price of a
Medical Center, Jackson, Miss); Lynn Kirby, RN, NP, COHN
medication and the cost of nonadherence. The price of
(Sanofi-Synthelabo Research, Malvern, Pa); Kathryn M. Kolasa,PhD, RD, LDN (Brody School of Medicine at East Carolina
medication is the amount of money needed for purchase, and
University, Greenville, NC); Stuart Linas, MD (University of Colo-
the cost is the outcome or consequences of not adhering to
rado Health Sciences Center, Denver, Colo); William M. Manger,
this treatment advice, which may include impaired quality of
MD, PhD (New York University Medical Center, New York, NY);
life, CVD, kidney failure, stroke, and even premature death.
Edwin C. Marshall, OD, MS, MPH (Indiana University School of
The identification of persons who can assist the patient with
Optometry, Bloomington, Ind); Barry J. Materson, MD, MBA
insurance concerns and social services may be important to
(University of Miami, Miami, Fla); Jay Merchant, MHA (Centers forMedicare & Medicaid Services, Washington, DC); Nancy Houston
overall adherence. Most pharmaceutical companies have
Miller, RN, BSN (Stanford University School of Medicine, Palo
special needs programs that are often handled through their
Alto, Calif); Marvin Moser, MD (Yale University School of Medi-
cine, Scarsdale, NY); William A. Nickey, DO (Philadelphia Collegeof Osteopathic Medicine, Philadelphia, Pa); Suzanne Oparil, MD
Additional Sources of Information
(University of Alabama at Birmingham, Birmingham, Ala); Otelio S.
Additional information is available at the NHLBI web site:
Randall, MD, FACC (Howard University Hospital, Washington,
DC); James W. Reed, MD, FACP, FACE (Morehouse School ofMedicine, Atlanta, Ga); Edward J. Roccella, PhD, MPH (National
Scheme Used for Classification of
Heart, Lung, and Blood Institute, Bethesda, Md); Lee Shaughnessy(National Stroke Association, Englewood, Colo); Sheldon G. Sheps,
the Evidence
MD (Mayo Clinic, Rochester, Minn); David B. Snyder, RPh, DDS
The studies that provided evidence supporting the recom-
(Health Resources and Services Administration, Rockville, Md);
mendations of this report were classified and reviewed by the
James R. Sowers, MD, FACP, FACE (SUNY Health Science Center
staff and the executive committee. The classification scheme
at Brooklyn, Brooklyn, NY); Leonard M. Steiner, MS, OD (Eye
is from the JNC 6 report and other NHBPEP Working Group
Group, Oakhurst, NJ); Ronald Stout, MD, MPH (Procter andGamble, Mason, Ohio); Rita D. Strickland, EdD, RN (New York
Institute of Technology, Springfield Gardens, NY); Carlos Vallbona,
These symbols are appended to the citations in the refer-
MD (Baylor College of Medicine, Houston, TX); Howard S. Weiss,
MD, MPH (Georgetown University Medical Center, Washington
M: Meta-analysis; use of statistical methods to combine the
Hospital Center, Walter Reed Army Medical Center, Washington,
results from clinical trials.
DC); Jack P. Whisnant, MD (Mayo Clinic and Mayo MedicalSchool, Rochester, Minn); Laurie Willshire, MPH, RN (American
RA: Randomized controlled trials; also known as experi-
Red Cross, Falls Church, Va); Gerald J. Wilson, MA, MBA (Citizens
mental studies.
for Public Action on Blood Pressure and Cholesterol, Inc., Potomac,
RE: Retrospective analyses; also known as case-control
Md); Mary Winston, EdD, RD (American Heart Association, Dallas,
Tex); Jackson T. Wright, Jr., MD, PhD (Case Western Reserve
F: Prospective study; also known as cohort studies, includ-
University, Cleveland, Ohio)
ing historical or prospective follow-up studies.
X: Cross-sectional survey; also known as prevalence
Additional Contributors
Jan N. Basile, MD, FACP (Veterans Administration Hospital,
Charleston, SC); James I. Cleeman, MD (National Heart, Lung, and
PR: Previous review or position statements.
Blood Institute, Bethesda, Md); Darla E. Danford, MPH, DSc
C: Clinical interventions (nonrandomized).
(National Heart, Lung, and Blood Institute, Bethesda, Md); RichardA. Dart, MD, FACP, FCCP, FAHA (Marshfield Clinic, Marshfield,
Wis); Karen A. Donato, SM, RD (National Heart, Lung, and BloodInstitute, Bethesda, Md); Mark E. Dunlap, MD (Louis Stokes
National High Blood Pressure Education Program
Cleveland VA Medical Center, Cleveland, Ohio); Brent M. Egan,
Coordinating Committee Participants
MD (Medical University of South Carolina, Charleston, SC);
Claude Lenfant, MD (National Heart, Lung, and Blood Institute,
William J. Elliott, MD, PhD (Rush University Medical Center,
Bethesda, Md); George L. Bakris, MD (Rush University Medical
Chicago, Ill); Bonita E. Falkner, MD (Thomas Jefferson University,
Chobanian et al
JNC 7 – COMPLETE REPORT
Philadelphia, Pa); John M. Flack, MD, MPH (Wayne State Univer-
sity School of Medicine, Detroit, Mich); David Lee Gordon, MD
1. Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA, Higgins M, et al.
(University of Miami School of Medicine, Miami, Fla); Philip B.
Prevalence of hypertension in the US adult population. Results from the
Gorelik, MD, MPH, FACP (Rush Medical College, Chicago, Ill);
Third National Health and Nutrition Examination Survey, 1988 –1991.
Mary M. Hand, MSPH, RN (National Heart, Lung, and Blood
Hypertension. 1995;25:305–313. X
Institute, Bethesda, Md); Linda A. Hershey, MD, PhD (VA WNY
2. Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and
Healthcare System, Buffalo, NY); Norman M. Kaplan, MD (Univer-
control of hypertension in the United States, 1988 –2000. JAMA. 2003;
sity of Texas Southwestern Medical School at Dallas, Dallas, Tex);
290:199 –206. X
Daniel Levy, MD (National Heart, Lung, and Blood Institute,
3. World Health Report 2002: Reducing risks, promoting healthy life.
Geneva, Switzerland:World Health Organization, 2002. http://
Framingham, Mass); James W. Lohr, MD (VA WNY Healthcare
System and SUNY Buffalo, Buffalo, NY); Vasilios Papademetriou,
4. JNC 6. National High Blood Pressure Education Program. The sixth
MD, FACP, FACC (Veterans Affairs Medical Center, Washington,
report of the Joint National Committee on Prevention, Detection, Eval-
DC); Thomas G. Pickering, MD, DPhil (Mount Sinai Medical
uation, and Treatment of High Blood Pressure. Arch Intern Med. 1997;
Center, New York, NY); Ileana L. Pin˜a, MD, FACC (University
157:2413–2446. PR
Hospitals of Cleveland, Cleveland, Ohio); L. Michael Prisant, MD,
5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo
FACC, FACP (Medical College of Georgia, Augusta, Ga); Clive
JL Jr, et al. The seventh report of the Joint National Committee on
Rosendorff, MD, PhD, FRCP (Veterans Affairs Medical Center,
Prevention, Detection, Evaluation, and Treatment of High Blood
Bronx, NY); Virend K. Somers, MD, PhD (Mayo Clinic and Mayo
Pressure: the JNC 7 Report. JAMA. 2003;289:2560 –2572. PR
Foundation, Rochester, Minn); Ray Townsend, MD (University of
6. U. S. Department of Health and Human Services, National Heart, Lung,
Pennsylvania School of Medicine, Philadelphia, Pa); Humberto
and Blood Institute. National High Blood Pressure Education Program.
Available at: http://www.nhlbi.nih.gov/about/nhbpep/index.htm.
Vidaillet, MD (Marshfield Clinic, Marshfield, Wis); Donald G. Vidt,
Accessed November, 2003.
MD (Cleveland Clinic Foundation, Cleveland, Ohio); William
7. National High Blood Pressure Education Program. Report of the
White, MD (The University of Connecticut Health Center, Farming-
National High Blood Pressure Education Program Working Group on
High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1–S22. PR
8. Roccella E, Kaplan N. Interpretation and evaluation of clinical
Joanne Karimbakas, MS, RD (American Institutes for Research
guidelines. In: Izzo JL Jr, Black HR (eds). Hypertension Primer: The
Health Program, Silver Spring, Md).
Essentials of High Blood Pressure: Basic Science, Population Science,and Clinical Management. Philadelphia, PA: Lippincott Williams &Wilkins; 2003. pp. 126 –127. PR
The National High Blood Pressure Education
9. Sheps SG, Roccella EJ. Reflections on the sixth report of the Joint
Program (NHBPEP) Coordinating Committee
National Committee on Prevention, Detection, Evaluation, and
Treatment of High Blood Pressure. Curr Hypertens Rep. 1999;1:342–345. PR
American Academy of Family Physicians; American Academy of
10. Whelton PK, He J, Appel LJ, Cutler JA, Havas S, Kotchen TA, et al.
Neurology; American Academy of Ophthalmology; American Acad-
Primary prevention of hypertension: Clinical and public health advisory
emy of Physician Assistants; American Association of Occupational
from The National High Blood Pressure Education Program. JAMA.
Health Nurses; American College of Cardiology; American College
2002;288:1882–1888. PR
of Chest Physicians; American College of Occupational and Envi-
11. Last JM, Abramson JH. A Dictionary of Epidemiology. 3rd ed. New
ronmental Medicine; American College of Physicians-American
York, NY: Oxford University Press; 1995.
Society of Internal Medicine; American College of Preventive
12. Shaughnessy AF, Slawson DC, Bennett JH. Becoming an information
Medicine; American Dental Association; American Diabetes Asso-
master: a guidebook to the medical information jungle. J Fam Pract.
ciation; American Dietetic Association; American Heart Associa-
1994;39:489 – 499. PR
tion; American Hospital Association; American Medical Associa-
13. Slawson DC, Shaughnessy AF. Obtaining useful information from
expert based sources. BMJ. 1997;314:947–949. PR
tion; American Nurses Association; American Optometric
14. Delbecq A, Van de Ven A, Gustafson D. Group Techniques for Program
Association; American Osteopathic Association; American Pharma-
Planning: A Guide to Nominal Group and Delphi Process. Glenview,
ceutical Association; American Podiatric Medical Association;
IL: Scott, Foresman; 1975. PR
American Public Health Association; American Red Cross; Ameri-
15. Franklin SS, Gustin W, Wong ND, Larson MG, Weber MA, Kannel WB,
can Society of Health-System Pharmacists; American Society of
et al. Hemodynamic patterns of age-related changes in blood pressure. The
Hypertension; American Society of Nephrology; Association of
Framingham Heart Study. Circulation. 1997;96:308 –315. X
Black Cardiologists; Citizens for Public Action on High Blood
16. Vasan RS, Beiser A, Seshadri S, Larson MG, Kannel WB, D'Agostino
Pressure and Cholesterol, Inc.; Hypertension Education Foundation,
RB, et al. Residual lifetime risk for developing hypertension in
Inc.; International Society on Hypertension in Blacks; National
middle-aged women and men: The Framingham Heart Study. JAMA.
Black Nurses Association, Inc.; National Hypertension Association,
2002;287:1003–1010. F
Inc.; National Kidney Foundation, Inc.; National Medical Associa-
17. Vasan RS, Larson MG, Leip EP, Kannel WB, Levy D. Assessment of
frequency of progression to hypertension in nonhypertensive partic-
tion; National Optometric Association; National Stroke Association;
ipants in the Framingham Heart Study: A cohort study. Lancet. 2001;
NHLBI Ad Hoc Committee on Minority Populations; Society for
358:1682–1686. F
Nutrition Education; The Society of Geriatric Cardiology. Federal
18. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific
Agencies: Agency for Health Care Research and Quality; Centers for
relevance of usual blood pressure to vascular mortality: A meta-analysis
Medicare and Medicaid Services; Department of Veterans Affairs;
of individual data for one million adults in 61 prospective studies.
Health Resources and Services Administration; National Center for
Prospective Studies Collaboration. Lancet. 2002;360:1903–1913. M
Health Statistics; National Heart, Lung, and Blood Institute; National
19. Vasan RS, Larson MG, Leip EP, Evans JC, O'Donnell CJ, Kannel WB,
Institute of Diabetes and Digestive and Kidney Diseases.
et al. Impact of high-normal blood pressure on the risk of cardiovasculardisease. N Engl J Med. 2001;345:1291–1297. F
20. Anderson KM, Wilson PWF, Odell PM, Kannel WB. An updated
coronary risk profile. A statement for health professionals. Circulation.
This work was supported entirely by the National Heart, Lung, and
1991;83:356 –362.
Blood Institute. We appreciate the assistance by Carol Creech,
21. Expert Panel on Detection, Evaluation, and Treatment of High Blood
MILS, and Gabrielle Gessner (American Institutes for Research
Cholesterol in Adults. Third report of the National Cholesterol Edu-
Health Program, Silver Spring, Md).
cation Program (NCEP) expert panel on detection, evaluation, and
treatment of high blood cholesterol in adults (Adult Treatment Panel
42. US Department of Health and Human Services, National Institutes of
III): final report. Circulation. 2002;106:3143–3421. PR
Health, National Heart, Lung, and Blood Institute. Facts about the
22. Franklin SS, Larson MG, Khan SA, Wong ND, Leip EP, Kannel WB, et
DASH eating plan. Available at http://www.nhlbi.nih.gov/health/public/
al. Does the relation of blood pressure to coronary heart disease risk
heart/hbp/dash/index.htm. Accessed November, 2003.
change with aging? The Framingham Heart Study. Circulation. 2001;
43. National Heart, Lung, and Blood Institute. Your guide to lowering high
103:1245–1249. F
blood pressure. Available at http://www.nhlbi.nih.gov/hbp/index.html.
23. Kostis JB, Davis BR, Cutler J, Grimm RH Jr, Berge KG, Cohen JD, et
Accessed November, 2003.
al. Prevention of heart failure by antihypertensive drug treatment in
44. US Department of Health and Human Services, National Institutes of
older persons with isolated systolic hypertension. SHEP Cooperative
Health, National Heart, Lung, and Blood Institute, National High Blood
Research Group. JAMA. 1997;278:212–216. RA
Pressure Education Program. National High Blood Pressure Education
24. SHEP Cooperative Research Group. Prevention of stroke by antihyper-
Month. Available at: http://hin.nhlbi.nih.gov/nhbpep_kit/. Accessed
tensive drug treatment in older persons with isolated systolic hyper-
November, 2003.
tension. Final results of the Systolic Hypertension in the Elderly
45. US Department of Health and Human Services, National Institutes of
Program (SHEP). JAMA. 1991;265:3255–3264. RA
Health, National Heart, Lung, and Blood Institute. The heart truth: a
25. Staessen JA, Thijs L, Fagard R, O'Brien ET, Clement D, de Leeuw PW, et
national awareness campaign for women about heart disease. Available
al. Predicting cardiovascular risk using conventional vs ambulatory blood
pressure in older patients with systolic hypertension. Systolic Hypertension
November, 2003.
in Europe Trial Investigators. JAMA. 1999;282:539 –546. RA
46. National Institutes of Health, National Heart, Lung, and Blood Institute,
26. Hyman DJ, Pavlik VN. Characteristics of patients with uncontrolled
Office of Prevention, Education, and Control. Mobilizing African
hypertension in the United States. N Engl J Med. 2001;345:479 – 486. X
American communities to address disparities in cardiovascular health:
27. Lloyd-Jones DM, Evans JC, Larson MG, O'Donnell CJ, Roccella EJ,
The Baltimore City Health Partnership Strategy Development
Levy D. Differential control of systolic and diastolic blood pressure:
Workshop. Summary report. Available at: http://www.nhlbi.nih.gov/
factors associated with lack of blood pressure control in the community.
health/prof/heart/other/balt_rpt.htm. Accessed November, 2003.
Hypertension. 2000;36:594 –599. F
47. US Department of Health and Human Services, National Institutes of
28. Cushman WC, Ford CE, Cutler JA, Margolis KL, Davis BR, Grimm
Health, National Heart, Lung, and Blood Institute. NHLBI Healthy
RH, et al. Success and predictors of blood pressure control in diverse
People 2010 Gateway. Available at: http://hin.nhlbi.nih.gov/. Accessed
North American settings: The Antihypertensive and Lipid-Lowering
November, 2003.
Treatment to Prevent Heart Attack Trial (ALLHAT). J Clin Hypertens
48. National Heart, Lung, and Blood Institute. Cardiovascular disease
(Greenwich). 2002;4:393– 404. RA
enhanced dissemination and utilization centers (EDUCs) awardees.
29. Black HR, Elliott WJ, Neaton JD, Grandits G, Grambsch P, Grimm R,
Available at: http://hin.nhlbi.nih.gov/educs/awardees.htm. Accessed
et al. Baseline characteristics and early blood pressure control in the
November, 2003.
CONVINCE trial. Hypertension. 2001;37:12–18. RA
49. National Institutes of Health, National Heart, Lung, and Blood Institute.
30. Hyman DJ, Pavlik VN, Vallbona C. Physician role in lack of awareness
Hearts N' Parks. Available at: http://www.nhlbi.nih.gov/health/prof/
and control of hypertension. J Clin Hypertens (Greenwich). 2000;2:
heart/obesity/hrt_n_pk/index.htm. Accessed November, 2003.
50. National Institutes of Health. Healthbeat radio network. Available at:
31. Berlowitz DR, Ash AS, Hickey EC, Friedman RH, Glickman M, Kader
http://radiospace.com/healthbeat.htm. Accessed November, 2003.
B, et al. Inadequate management of blood pressure in a hypertensive
51. National Heart, Lung, and Blood Institute. Salud para su Corazo´n (For
population. N Engl J Med. 1998;339:1957–1963.
the Health of Your Heart). Available at: http://www.nhlbi.nih.gov/
32. Stamler J, Stamler R, Neaton JD, Wentworth D, Daviglus ML, Garside
health/prof/heart/latino/salud.htm. Accessed November, 2003.
D, et al. Low risk-factor profile and long-term cardiovascular and
52. National Institutes of Health. Mad as a hatter? Join our campaign for a
noncardiovascular mortality and life expectancy: findings for 5 large
mercury free NIH. Available at: http://www.nih.gov/od/ors/ds/
cohorts of young adult and middle-aged men and women. JAMA. 1999;
nomercury/. Accessed November, 2003.
282:2012–2018. F
53. Jones DW, Appel LJ, Sheps SG, Roccella EJ, Lenfant C. Measuring
33. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in
blood pressure accurately: new and persistent challenges. JAMA. 2003;
obesity among US adults, 1999 –2000. JAMA. 2002;288:1723–1727. X
289:1027–1030. PR
34. Cleveland LE, Goldman JD, Borrud LG. Data tables: results from
54. Working Meeting on Blood Pressure Measurement: Summary Report.
USDA's 1994 continuing survey of food intakes by individuals and1994 diet and health knowledge survey. Riverdale, MD: Agricultural
Research Service, US Department of Agriculture.1996.http://
measu.pdf. Accessed November, 2003.
55. Canzanello VJ, Jensen PL, Schwartz GL. Are aneroid sphygmoma-
35. James WP, Ralph A, Sanchez-Castillo CP. The dominance of salt in
nometers accurate in hospital and clinic settings? Arch Intern Med.
manufactured food in the sodium intake of affluent societies. Lancet.
2001;161:729 –731. PR
1987;1:426 – 429.
56. Perloff D, Grim C, Flack J, Frohlich ED, Hill M, McDonald M, et al.
36. U S Department of Health and Human Services. Physical activity and
Human blood pressure determination by sphygmomanometry. Circu-
health: a report of the Surgeon General. Atlanta, GA: US Department of
lation. 1993;88:2460 –2470. PR
Health and Human Services, Centers for Disease Control and Pre-
57. Gerin W, Schwartz AR, Schwartz JE, Pickering TG, Davidson KW,
vention, National Center for Chronic Disease Prevention and Health
Bress J, et al. Limitations of current validation protocols for home blood
Promotion. 1996. http://www.cdc.gov/nccdphp/sgr/contents.htm PR
pressure monitors for individual patients. Blood Press Monit. 2002;7:
37. Division of Adult and Community Health, National Center for Chronic
Disease Prevention and Health Promotion, Centers for Disease Control
58. World Hypertension League. Measuring your blood pressure. Available at:
and Prevention. 5 a day surveillance: behavioral risk factor surveillance
http://www.mco.edu/org/whl/bloodpre.html. Accessed November, 2003.
system online prevalence data, 1995–2000. Available at: http://
59. Pickering T. Recommendations for the use of home (self) and ambu-
apps.nccd.cdc.gov/5ADaySurveillance/. Accessed November, 2003.
latory blood pressure monitoring. American Society of Hypertension Ad
38. Stamler R. Implications of the INTERSALT study. Hypertension. 1991;
Hoc Panel. Am J Hypertens. 1996;9 :1–11. PR
17:I16 –I20.
60. Kario K, Pickering TG, Umeda Y, Hoshide S, Hoshide Y, Morinari M,
39. American Public Health Association. 2002– 4 Reducing sodium content
et al. Morning surge in blood pressure as a predictor of silent and clinical
in the American diet. Association News. 2002;5– 6.
cerebrovascular disease in elderly hypertensives: a prospective study.
40. National High Blood Pressure Education Program. Summary report: the
Circulation. 2003;107:1401–1406. F
National High Blood Pressure Education Program Coordinating Com-
61. Pickering TG, Coats A, Mallion JM, Mancia G, Verdecchia P. Blood
mittee meeting. Bethesda, MD: National High Blood Pressure Education
Pressure Monitoring. Task force V: White-coat hypertension. Blood
Program, National Heart, Lung, and Blood Institute; 2002. pp. 1–37.
Press Monit. 1999;4:333–341. PR
62. Verdecchia P. Prognostic value of ambulatory blood pressure: current
41. Office of Disease Prevention and Health Promotion, US Department of
evidence and clinical implications. Hypertension. 2000;35:844 – 851. PR
Health and Human Services. Healthy People 2010. Available at: http://
63. Clement DL, De Buyzere ML, De Bacquer DA, de Leeuw PW, Duprez
www.healthypeople.gov/. Accessed November, 2003.
DA, Fagard RH, et al. Prognostic value of ambulatory blood-pressure
Chobanian et al
JNC 7 – COMPLETE REPORT
recordings in patients with treated hypertension. N Engl J Med. 2003;
Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet.
348:2407–2415. F
1998;351:1755–1762. RA
64. Gillman MW, Kannel WB, Belanger A, D'Agostino RB. Influence of
88. American Diabetes Association. Treatment of hypertension in adults
heart rate on mortality among persons with hypertension: the Fra-
with diabetes. Diabetes Care. 2003;26:S80 –S82. PR
mingham Study. Am Heart J. 1993;125:1148 –1154. F
89. National Kidney Foundation Guideline. K/DOQI clinical practice
65. Tsuji H, Venditti FJ Jr, Manders ES, Evans JC, Larson MG, Feldman
guidelines for chronic kidney disease: Evaluation, classification, and
CL, et al. Reduced heart rate variability and mortality risk in an elderly
stratification. Kidney Disease Outcome Quality Initiative. Am J Kidney
cohort. The Framingham Heart Study. Circulation. 1994;90:878 – 883. F
Dis. 2002;39:S1–S246. PR
66. GFR /1.73 M2 by MDRD (⫾ SUN and SAlb) Calculator. Available at:
90. Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calcium
http://www.hdcn.com/calcf/gfr.htm. Accessed November, 2003.
antagonists, and other blood-pressure-lowering drugs: results of pro-
67. Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal insufficiency
spectively designed overviews of randomised trials. Blood Pressure
as a predictor of cardiovascular outcomes and the impact of ramipril: the
Lowering Treatment Trialists' Collaboration. Lancet. 2000;356:
HOPE randomized trial. Ann Intern Med. 2001;134:629 – 636. RA
68. Beddhu S, Allen-Brady K, Cheung AK, Horne BD, Bair T, Muhlestein
91. Ogden LG, He J, Lydick E, Whelton PK. Long-term absolute benefit of
JB, et al. Impact of renal failure on the risk of myocardial infarction and
lowering blood pressure in hypertensive patients according to the JNC
death. Kidney Int. 2002;62:1776 –1783. RE
VI risk stratification. Hypertension. 2000;35:539 –543. X
69. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more
92. The Trials of Hypertension Prevention Collaborative Research Group.
accurate method to estimate glomerular filtration rate from serum cre-
Effects of weight loss and sodium reduction intervention on blood
atinine: a new prediction equation. Modification of Diet in Renal
pressure and hypertension incidence in overweight people with high-
Disease Study Group. Ann Intern Med. 1999;130:461– 470. X
normal blood pressure. The Trials of Hypertension Prevention, phase II.
70. Jensen JS, Feldt-Rasmussen B, Strandgaard S, Schroll M, Borch-
Arch Intern Med. 1997;157:657– 667. RA
Johnsen K. Arterial hypertension, microalbuminuria, and risk of ische-
93. He J, Whelton PK, Appel LJ, Charleston J, Klag MJ. Long-term effects
mic heart disease. Hypertension. 2000;35:898 –903. X
of weight loss and dietary sodium reduction on incidence of hyper-
71. Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, Hoogwerf B, et
tension. Hypertension. 2000;35:544 –549. F
al. Albuminuria and risk of cardiovascular events, death, and heart
94. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et
failure in diabetic and nondiabetic individuals. JAMA. 2001;286:
al. Effects on blood pressure of reduced dietary sodium and the Dietary
Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collab-
72. Garg JP, Bakris GL. Microalbuminuria: marker of vascular dysfunction,
orative Research Group. N Engl J Med. 2001;344 :3–10. RA
risk factor for cardiovascular disease. Vasc Med. 2002;7:35– 43. PR
95. Vollmer WM, Sacks FM, Ard J, Appel LJ, Bray GA, Simons-Morton
73. Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of
DG, et al. Effects of diet and sodium intake on blood pressure: subgroup
C-reactive protein and low-density lipoprotein cholesterol levels in the
analysis of the DASH-sodium trial. Ann Intern Med. 2001;135:
prediction of first cardiovascular events. N Engl J Med. 2002;347:
96. Chobanian AV, Hill M. National Heart, Lung, and Blood Institute
74. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and
Workshop on Sodium and Blood Pressure: a critical review of current
other markers of inflammation in the prediction of cardiovascular
scientific evidence. Hypertension. 2000;35:858 – 863. PR
disease in women. N Engl J Med. 2000;342:836 – 843. F
97. Kelley GA, Kelley KS. Progressive resistance exercise and resting blood
75. Boden-Albala B, Sacco RL. Lifestyle factors and stroke risk: exercise,
pressure: a meta-analysis of randomized controlled trials. Hypertension.
alcohol, diet, obesity, smoking, drug use, and stress. Curr Atheroscler
2000;35:838 – 843. M
Rep. 2000;2:160 –166. PR
98. Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood
76. Parsons DS, Reaveley DA, Pavitt DV, Brown EA. Relationship of renal
pressure: a meta-analysis of randomized, controlled trials. Ann Intern
function to homocysteine and lipoprotein(a) levels: the frequency of the
Med. 2002;136:493–503. M
combination of both risk factors in chronic renal impairment. Am J
99. Xin X, He J, Frontini MG, Ogden LG, Motsamai OI, Whelton PK.
Kidney Dis. 2002;40:916 –923. C
Effects of alcohol reduction on blood pressure: a meta-analysis of
77. Manger WM, Gifford RW. Pheochromocytoma. J Clin Hypertens
randomized controlled trials. Hypertension. 2001;38:1112–1117. M
100. Appel LJ, Champagne CM, Harsha DW, Cooper LS, Obarzanek E,
78. Textor SC. Revascularization in atherosclerotic renal artery disease.
Elmer PJ, et al. Effects of comprehensive lifestyle modification on blood
Kidney Int. 1998;53:799 – 811.
pressure control: main results of the PREMIER clinical trial. Writing
79. Pohl MA. Renovascular hypertension and ischemic nephropathy. In:
Group of the PREMIER Collaborative Research Group. JAMA. 2003;
Wilcox CS (ed): Atlas of Diseases of the Kidney. Philadelphia, PA:
289:2083–2093. RA
Developed by Current Medicine, Inc.; 1999.
101. Black HR, Elliott WJ, Grandits G, Grambsch P, Lucente T, White WB,
80. Biglieri EG. Primary aldosteronism. Curr Ther Endocrinol Metab. 1997;
et al. Principal results of the Controlled Onset Verapamil Investigation
6:170 –172.
of Cardiovascular End Points (CONVINCE) trial. JAMA. 2003;289:
81. National High Blood Pressure Education Program Working Group. 1995
update of the working group reports on chronic renal failure and reno-
102. Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, Faire U, et
vascular hypertension. Arch Intern Med. 1996;156:1938 –1947. PR
al. Cardiovascular morbidity and mortality in the Losartan Intervention
82. Lifton RP, Gharavi AG, Geller DS. Molecular mechanisms of human
For Endpoint reduction in hypertension study (LIFE): A randomised
hypertension. Cell. 2001;104:545–556. PR
trial against atenolol. Lancet. 2002;359:995–1003. RA
83. Bray MS, Li L, Turner ST, Kardia SL, Boerwinkle E. Association and
103. Materson BJ, Reda DJ, Cushman WC, Massie BM, Freis ED, Kochar
linkage analysis of the alpha-adducin gene and blood pressure. Am J
MS, et al. Single-drug therapy for hypertension in men: a comparison of
Hypertens. 2000;13:699 –703. F
six antihypertensive agents with placebo. The Department of Veterans
84. Beeks E, Janssen RG, Kroon AA, Keulen ET, Geurts JM, de Leeuw PW,
Affairs Cooperative Study Group on Antihypertensive Agents. N Engl
et al. Association between the alpha-adducin Gly460Trp polymorphism
J Med. 1993;328:914 –921. RA
and systolic blood pressure in familial combined hyperlipidemia. Am J
104. Cutler JA, MacMahon SW, Furberg CD. Controlled clinical trials of
Hypertens. 2001;14:1185–1190. C
drug treatment for hypertension: a review. Hypertension. 1989;13:
85. Psaty BM, Smith NL, Heckbert SR, Vos HL, Lemaitre RN, Reiner AP,
et al. Diuretic therapy, the alpha-adducin gene variant, and the risk of
105. Collins R, Peto R, Godwin J, MacMahon S. Blood pressure and coro-
myocardial infarction or stroke in persons with treated hypertension.
nary heart disease. Lancet. 1990;336:370 –371.
JAMA. 2002;287:1680 –1689. RE
106. Chalmers J, Zanchetti A. The 1996 report of a World Health Organi-
86. Cooper-DeHoff RM, Bristol HA, Pepine CJ. Ethnic differences in sys-
zation expert committee on hypertension control. J Hypertens. 1996;14:
tolic blood pressure control in hypertensive patients with coronary artery
disease. Am J Hypertens. 2003;16:27A.
107. Psaty BM, Smith NL, Siscovick DS, Koepsell TD, Weiss NS, Heckbert
87. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S,
SR, et al. Health outcomes associated with antihypertensive therapies
et al. Effects of intensive blood-pressure lowering and low-dose aspirin
used as first-line agents: a systematic review and meta-analysis. JAMA.
in patients with hypertension: principal results of the Hypertension
1997;277:739 –745. M
108. Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M,
126. Franse LV, Pahor M, Di Bari M, Somes GW, Cushman WC, Applegate
Alderman MH, et al. Health outcomes associated with various antihy-
WB. Hypokalemia associated with diuretic use and cardiovascular
pertensive therapies used as first-line agents: a network meta-analysis.
events in the Systolic Hypertension in the Elderly program. Hyper-
JAMA. 2003;289:2534 –2544. M
tension. 2000;35:1025–1030. RA
109. The ALLHAT Officers and Coordinators for the ALLHAT Collabo-
127. Papademetriou V, Burris JF, Notargiacomo A, Fletcher RD, Freis ED.
rative Research Group. Major outcomes in high-risk hypertensive
Thiazide therapy is not a cause of arrhythmia in patients with systemic
patients randomized to angiotensin-converting enzyme inhibitor or
hypertension. Arch Intern Med. 1988;148:1272–1276. C
calcium channel blocker vs diuretic: the Antihypertensive and Lipid-
128. Psaty BM, Manolio TA, Smith NL, Heckbert SR, Gottdiener JS, Burke
Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA.
GL, et al. Time trends in high blood pressure control and the use of
2002;288:2981–2997. RA
antihypertensive medications in older adults: The Cardiovascular Health
110. Heart Outcomes Prevention Evaluation Study Investigators. Effects of
Study. Arch Intern Med. 2002;162:2325–2332. X
an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular
129. Sica DA. Rationale for fixed-dose combinations in the treatment of
events in high-risk patients. N Engl J Med. 2000;342:145–153. RA
hypertension: the cycle repeats. Drugs. 2002;62:443– 462. PR
130. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combi-
perindopril-based blood-pressure-lowering regimen among 6,105 indi-
nation treatment with blood pressure lowering drugs: analysis of 354
viduals with previous stroke or transient ischaemic attack. Lancet. 2001;
randomised trials. BMJ. 2003;326:1427–1434. M
358:1033–1041. RA
131. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of
112. Wing LM, Reid CM, Ryan P, Beilin LJ, Brown MA, Jennings GL, et al.
randomised trials of antiplatelet therapy for prevention of death, myo-
A comparison of outcomes with angiotensin-converting– enzyme inhib-
cardial infarction, and stroke in high risk patients. BMJ. 2002;324:
itors and diuretics for hypertension in the elderly. N Engl J Med.
2003;348:583–592. RA
132. Hunt SA, Baker DW, Chin MH, Cinquegrani MP, Feldman AM, Francis
113. Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager
GS, et al. ACC/AHA Guidelines for the evaluation and management of
WH, et al. Randomised double-blind comparison of placebo and active
chronic heart failure in the adult: executive summary. A report of the
treatment for older patients with isolated systolic hypertension. The
American College of Cardiology/American Heart Association Task
Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet.
Force on Practice Guidelines (Committee to Revise the 1995 Guidelines
1997;350:757–764. RA
for the Evaluation and Management of Heart Failure): developed in
114. The European Trial on Reduction of Cardiac Events with Perindopril in
collaboration with the International Society for Heart and Lung Trans-
Stable Coronary Artery Disease investigators. Efficacy of perindopril in
plantation;endorsed by the Heart Failure Society of America. Circu-
reduction of cardiovascular events among patients with stable coronary
lation. 2001;104:2996 –3007. PR
artery disease: randomised, double-blind, placebo-controlled, multi-
133. Tepper D. Frontiers in congestive heart failure: effect of Metoprolol
centre trial (the EUROPA study). Lancet. 2003;362:782–788. RA
CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Inter-
115. Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner T, Niklason A,
vention Trial in Congestive Heart Failure (MERIT-HF). MERIT-HF
et al. Effect of angiotensin-converting-enzyme inhibition compared with
Study Group. Congest Heart Fail. 1999;5:184 –185. RA
conventional therapy on cardiovascular morbidity and mortality in
134. Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, et al.
hypertension: the Captopril Prevention Project (CAPPP) randomised
Effect of carvedilol on survival in severe chronic heart failure. N Engl
trial. Lancet. 1999;353:611– 616. RA
J Med. 2001;344:1651–1658. RA
116. Hansson L, Lindholm LH, Ekbom T, Dahlof B, Lanke J, Schersten B, et al.
135. CIBIS Investigators and Committees. A randomized trial of beta-
Randomised trial of old and new antihypertensive drugs in elderly patients:
blockade in heart failure. The Cardiac Insufficiency Bisoprolol Study
cardiovascular mortality and morbidity: the Swedish Trial in Old Patients
(CIBIS). Circulation. 1994;90:1765–1773. RA
with Hypertension-2 study. Lancet. 1999;354:1751–1756. RA
136. The SOLVD Investigators. Effect of enalapril on survival in patients
117. Hansson L, Hedner T, Lund-Johansen P, Kjeldsen SE, Lindholm LH,
with reduced left ventricular ejection fractions and congestive heart
Syvertsen JO, et al. Randomised trial of effects of calcium antagonists
failure. N Engl J Med. 1991;325:293–302. RA
compared with diuretics and beta-blockers on cardiovascular morbidity
137. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators.
and mortality in hypertension: the Nordic Diltiazem (NORDIL) study.
Effect of ramipril on mortality and morbidity of survivors of acute
Lancet. 2000;356:359 –365. RA
myocardial infarction with clinical evidence of heart failure. Lancet.
118. Brown MJ, Palmer CR, Castaigne A, de Leeuw PW, Mancia G,
1993;342:821– 828. RA
Rosenthal T, et al. Morbidity and mortality in patients randomised to
138. Kober L, Torp-Pedersen C, Carlsen JE, Bagger H, Eliasen P, Lyngborg
double-blind treatment with a long-acting calcium-channel blocker or
K, et al. A clinical trial of the angiotensin-converting-enzyme inhibitor
diuretic in the International Nifedipine GITS study: Intervention as a
trandolapril in patients with left ventricular dysfunction after myocardial
Goal in Hypertension Treatment (INSIGHT). Lancet. 2000;356:
infarction. Trandolapril Cardiac Evaluation (TRACE) Study Group.
N Engl J Med. 1995;333:1670 –1676. RA
119. Black HR. The evolution of low-dose diuretic therapy: the lessons from
139. Cohn JN, Tognoni G. A randomized trial of the angiotensin-receptor
clinical trials. Am J Med. 1996;101:47S–52S. PR
blocker valsartan in chronic heart failure. The Valsartan Heart Failure
120. Materson BJ, Cushman WC, Goldstein G, Reda DJ, Freis ED, Ramirez
Trial Investigators. N Engl J Med. 2001;345:1667–1675. RA
EA, et al. Department of Veterans Affairs Cooperative Study Group on
140. Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The
Antihypertensive Agents: Treatment of hypertension in the elderly, I:
effect of spironolactone on morbidity and mortality in patients with
blood pressure and clinical changes. Results of a Department of
severe heart failure. Randomized Aldactone Evaluation Study Investi-
Veterans Affairs Cooperative Study. Hypertension. 1990;15:348 –360.
gators. N Engl J Med. 1999;341:709 –717. RA
121. Siscovick DS, Raghunathan TE, Psaty BM, Koepsell TD, Wicklund KG,
141. McMurray J, Ostergren J, Pfeffer M, Swedberg K, Granger C, Yusuf S,
Lin X, et al. Diuretic therapy for hypertension and the risk of primary
et al. Clinical features and contemporary management of patients with
cardiac arrest. N Engl J Med. 1994;330:1852–1857. RE
low and preserved ejection fraction heart failure: baseline characteristics
122. Flack JM, Cushman WC. Evidence for the efficacy of low-dose diuretic
of patients in the Candesartan in Heart failure-Assessment of Reduction
monotherapy. Am J Med. 1996;101:53S– 60S. PR
in Mortality and morbidity (CHARM) programme. Eur J Heart Fail.
123. Grimm RH Jr, Grandits GA, Prineas RJ, McDonald RH, Lewis CE,
Flack JM, et al. Long-term effects on sexual function of five antihyper-
142. Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas
tensive drugs and nutritional hygienic treatment in hypertensive men and
JS, et al. ACC/AHA 2002 guideline update for the management of
women. Treatment of Mild Hypertension Study (TOMHS). Hyper-
patients with chronic stable angina–summary article: a report of the
tension. 1997;29:8 –14. RA
American College of Cardiology/American Heart Association Task
124. Moser M. Why are physicians not prescribing diuretics more frequently
Force on practice guidelines (Committee on the Management of Patients
in the management of hypertension? JAMA. 1998;279:1813–1816.
With Chronic Stable Angina). J Am Coll Cardiol. 2003;41:159 –168. PR
125. Lakshman MR, Reda DJ, Materson BJ, Cushman WC, Freis ED. Di-
143. -Blocker Heart Attack Trial Research Group. A randomized trial of
uretics and beta-blockers do not have adverse effects at 1 year on plasma
propranolol in patients with acute myocardial infarction, I: mortality
lipid and lipoprotein profiles in men with hypertension. Department of
results. JAMA. 1982;247:1707–1714. RA
Veterans Affairs Cooperative Study Group on Antihypertensive Agents.
144. Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ Jr, Cuddy TE,
Arch Intern Med. 1999;159:551–558. RA
et al. Effect of captopril on mortality and morbidity in patients with left
Chobanian et al
JNC 7 – COMPLETE REPORT
ventricular dysfunction after myocardial infarction. Results of the
165. Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, et
Survival and Ventricular Enlargement trial. The SAVE Investigators.
al. Preserving renal function in adults with hypertension and diabetes: a
N Engl J Med. 1992;327:669 – 677. RA
consensus approach. National Kidney Foundation Hypertension and
145. The Capricorn Investigators. Effect of carvedilol on outcome after myo-
Diabetes Executive Committees Working Group. Am J Kidney Dis.
cardial infarction in patients with left-ventricular dysfunction: The CAP-
2000;36:646 – 661. PR
RICORN randomised trial. Lancet. 2001;357:1385–1390. RA
166. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality
146. Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, et al.
from coronary heart disease in subjects with type 2 diabetes and in
Eplerenone, a selective aldosterone blocker, in patients with left ven-
nondiabetic subjects with and without prior myocardial infarction.
tricular dysfunction after myocardial infarction. N Engl J Med. 2003;
N Engl J Med. 1998;339:229 –234. F
348:1309 –1321.
167. Assman G, Cullen P, Schulte H. The Munster Heart Study (PROCAM):
147. Pepine CJ, Handberg EM, Cooper-DeHoff RM, Marks RG, Kowey P,
results of follow-up at 8 years. Eur Heart J. 1998;19:A2–A11. F
Messerli F, et al. for the INVEST Investigators. A calcium antagonist
168. Fagan TC, Sowers J. Type 2 diabetes mellitus: greater cardiovascular
versus a noncalcium antagonist hypertension treatment strategy for
risks and greater benefits of therapy. Arch Intern Med. 1999;159:
patients with coronary artery disease. The International Verapamil-
Trandolapril Study (INVEST): a randomized controlled trial. JAMA.
169. Davis TM, Millns H, Stratton IM, Holman RR, Turner RC. Risk factors for
stroke in type 2 diabetes mellitus: United Kingdom Prospective Diabetes
148. UKPDS 39. Efficacy of atenolol and captopril in reducing risk of
Study (UKPDS) 29. Arch Intern Med. 1999;159:1097–1103. RA
macrovascular and microvascular complications in type 2 diabetes:
170. Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV,
UKPDS 39. UK Prospective Diabetes Study Group. BMJ. 1998;317:
et al. Diabetes and cardiovascular disease: a statement for healthcare
professionals from the American Heart Association. Circulation. 1999;
149. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angioten-
100:1134 –1146. PR
sin-converting-enzyme inhibition on diabetic nephropathy. The Collab-
171. Sowers JR, Haffner S. Treatment of cardiovascular and renal risk factors
orative Study Group. N Engl J Med. 1993;329:1456 –1462. RA
in the diabetic hypertensive. Hypertension. 2002;40:781–788.
150. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving
172. Gress TW, Nieto FJ, Shahar E, Wofford MR, Brancati FL. Hypertension
HH, et al. Effects of losartan on renal and cardiovascular outcomes in
and antihypertensive therapy as risk factors for type 2 diabetes mellitus.
patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;
Atherosclerosis Risk in Communities Study. N Engl J Med. 2000;342:
345:861– 869. RA
151. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, et al.
173. Sowers JR, Bakris GL. Antihypertensive therapy and the risk of type 2
Renoprotective effect of the angiotensin-receptor antagonist irbesartan
diabetes mellitus. N Engl J Med. 2000;342:969 –970.
in patients with nephropathy due to type 2 diabetes. N Engl J Med.
174. Adler AI, Stratton IM, Neil HA, Yudkin JS, Matthews DR, Cull CA, et
2001;345:851– 860. RA
al. Association of systolic blood pressure with macrovascular and micro-
152. The GISEN Group (Gruppo Italiano di Studi Epidemiologici in
vascular complications of type 2 diabetes (UKPDS 36): prospective
Nefrologia). Randomised placebo-controlled trial of effect of ramipril on
observational study. BMJ. 2000;321:412– 419. RA
decline in glomerular filtration rate and risk of terminal renal failure in
175. UKPDS 38. Tight blood pressure control and risk of macrovascular and
proteinuric, non-diabetic nephropathy. Lancet. 1997;349:1857–1863.
microvascular complications in type 2 diabetes: UKPDS 38. UK Pro-
spective Diabetes Study Group. BMJ. 1998;317:703–713. RA
153. Wright JT Jr, Agodoa L, Contreras G, Greene T, Douglas JG, Lash J, et
176. Goldstein LB, Adams R, Becker K, Furberg CD, Gorelick PB,
al. Successful blood pressure control in the African American Study of
Hademenos G, et al. Primary prevention of ischemic stroke: a statement
Kidney Disease and Hypertension. Arch Intern Med. 2002;162:
for healthcare professionals from the Stroke Council of the American
Heart Association. Circulation. 2001;103:163–182. PR
154. Rosendorff C. Treatment of hypertension patients with ischemic heart
177. Maki DD, Ma JZ, Louis TA, Kasiske BL. Long-term effects of antihy-
disease. In: Izzo JL Jr, Black HR (eds): Hypertension Primer: The
pertensive agents on proteinuria and renal function. Arch Intern Med.
Essentials of High Blood Pressure: Basic Science, Population Science,
1995;155:1073–1080. M
and Clinical Management. Philadelphia, PA: Lippincott Williams &
178. Nelson RG, Bennett PH, Beck GJ, Tan M, Knowler WC, Mitch WE, et
Wilkins; 2003. pp. 456 – 459. PR
al. Development and progression of renal disease in Pima Indians with
155. Somes GW, Pahor M, Shorr RI, Cushman WC, Applegate WB. The role
non-insulin-dependent diabetes mellitus. Diabetic Renal Disease Study
of diastolic blood pressure when treating isolated systolic hypertension.
Group. N Engl J Med. 1996;335:1636 –1642. C
Arch Intern Med. 1999;159:2004 –2009. RA
179. Kohner EM, Aldington SJ, Stratton IM, Manley SE, Holman RR,
156. Chrysant GS, Oparil S. Treatment of hypertension in the patient with
Matthews DR, et al. United Kingdom Prospective Diabetes Study, 30:
cardiovascular disease. In: Antman EM (ed): Cardiovascular Thera-
diabetic retinopathy at diagnosis of non-insulin-dependent diabetes
peutics: A Companion to Braunwald's Heart Disease. Philadelphia, PA:
mellitus and associated risk factors. Arch Ophthalmol. 1998;116:
WB Saunders; 2001. pp. 768 –795. PR
157. Senni M, Redfield MM. Heart failure with preserved systolic function.
180. Tuomilehto J, Rastenyte D, Birkenhager WH, Thijs L, Antikainen R,
A different natural history? J Am Coll Cardiol. 2001;38:1277–1282. PR
Bulpitt CJ, et al. Effects of calcium-channel blockade in older patients
158. Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, et
with diabetes and systolic hypertension. Systolic Hypertension in
al. Long-term trends in the incidence of and survival with heart failure.
Europe Trial Investigators. N Engl J Med. 1999;340:677– 684. RA
N Engl J Med. 2002;347:1397–1402. F
181. Remuzzi G, Schieppati A, Ruggenenti P. Clinical practice: nephropathy
159. American Heart Association. Heart disease and stroke statistics–2003
in patients with type 2 diabetes. N Engl J Med. 2002;346:1145–1151.
update. Dallas, TX: American Heart Association; 2002.
182. Parving HH, Andersen AR, Smidt UM, Hommel E, Mathiesen ER,
160. The Digitalis Investigation Group. The effect of digoxin on mortality
Svendsen PA. Effect of antihypertensive treatment on kidney function in
and morbidity in patients with heart failure. N Engl J Med. 1997;336:
diabetic nephropathy. BMJ (Clin Res Ed). 1987;294:1443–1447. F
183. Mogensen CE, Keane WF, Bennett PH, Jerums G, Parving HH, Passa P,
161. Mokdad AH, Ford ES, Bowman BA, Nelson DE, Engelgau MM,
et al. Prevention of diabetic renal disease with special reference to
Vinicor F, et al. Diabetes trends in the U S: 1990 –1998. Diabetes Care.
microalbuminuria. Lancet. 1995;346:1080 –1084. PR
2000;23:1278 –1283. X
184. Sowers JR, Reed J. 1999 clinical advisory: treatment of hypertension
162. Prevalence of Diabetes and Impaired Fasting Glucose in Adults–United
and diabetes. J Clin Hypertens (Greenwich). 2000;2:132–133. PR
States, 1999 –2000. Morbidity and Mortality Weekly Report. 2003;52:
185. Weinberger MH. Blood pressure and metabolic responses to hydrochlo-
rothiazide, captopril, and the combination in black and white mild-to-
163. Collins AJ, Kasiske B, Herzog C, Chen S-C, Everson S, Constantini E,
moderate hypertensive patients. J Cardiovasc Pharmacol. 1985;7:
et al. Excerpts from the United States Renal Data System 2001 Annual
Data Report: Atlas of End-Stage Renal Disease in the United States.
186. Heart Outcomes Prevention Evaluation Study Investigators. Effects of
Am J Kidney Dis. 2001;38:S7–S247.
ramipril on cardiovascular and microvascular outcomes in people with
164. American Diabetes Association. Diabetic nephropathy. Diabetes Care.
diabetes mellitus: results of the HOPE study and MICRO-HOPE
2002;25:S85–S89. PR
substudy. Lancet. 2000;355:253–259. RA
187. Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U,
2010. Washington, DC: United States Government Printing Office;
et al. Cardiovascular morbidity and mortality in patients with diabetes in
2000. pp. 19 –31.
the Losartan Intervention For Endpoint reduction in hypertension study
206. Jamerson K, DeQuattro V. The impact of ethnicity on response to
(LIFE): a randomised trial against atenolol. Lancet. 2002;359:
antihypertensive therapy. Am J Med. 1996;101:22S–32S. PR
207. Saunders E, Weir MR, Kong BW, Hollifield J, Gray J, Vertes V, et al.
188. Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford N, Schrier
A comparison of the efficacy and safety of a beta-blocker, a calcium
RW. The effect of nisoldipine as compared with enalapril on cardiovas-
channel blocker, and a converting enzyme inhibitor in hypertensive
cular outcomes in patients with non-insulin-dependent diabetes and
blacks. Arch Intern Med. 1990;150:1707–1713. RA
hypertension. N Engl J Med. 1998;338:645– 652. RA
208. Cushman WC, Reda DJ, Perry HM, Williams D, Abdellatif M, Materson
189. Schrier RW, Estacio RO, Esler A, Mehler P. Effects of aggressive blood
BJ. Regional and racial differences in response to antihypertensive
pressure control in normotensive type 2 diabetic patients on albuminuria,
medication use in a randomized controlled trial of men with hyper-
retinopathy and strokes. Kidney Int. 2002;61:1086 –1097. RA
tension in the United States. Department of Veterans Affairs Coop-
190. Manjunath G, Tighiouart H, Ibrahim H, MacLeod B, Salem DN, Griffith
erative Study Group on Antihypertensive Agents. Arch Intern Med.
JL, et al. Level of kidney function as a risk factor for atherosclerotic
2000;160:825– 831. RA
cardiovascular outcomes in the community. J Am Coll Cardiol. 2003;
209. Brown NJ, Ray WA, Snowden M, Griffin MR. Black Americans have
an increased rate of angiotensin converting enzyme inhibitor-associated
191. Hillege HL, Fidler V, Diercks GF, van Gilst WH, de Zeeuw D, van
angioedema. Clin Pharmacol Ther. 1996;60:8 –13. RE
Veldhuisen DJ, et al. Urinary albumin excretion predicts cardiovascular
210. Lawrence J, Stockbridge N, Hung HMJ, Chi G. Joint statistical-clinical
and noncardiovascular mortality in general population. Circulation.
review: NDA resubmission dated 14 December 2001, including the
2002;106:1777–1782. F
results of the OCTAVE study. FDA, Center for Drug Evaluation and
192. Franklin SS, Jacobs MJ, Wong ND, L'Italien GJ, Lapuerta P. Predom-
Research, Division of Cardio-Renal Drug Products. NDA: 21–188
inance of isolated systolic hypertension among middle-aged and elderly
(omapatrilat for hypertension), June 2002. pp. 1–31. http://
US hypertensives: analysis based on National Health and Nutrition
Examination Survey (NHANES) III. Hypertension. 2001;37:869 – 874.
211. Elliott WJ. Higher incidence of discontinuation of angiotensin con-
193. Coresh J, Wei GL, McQuillan G, Brancati FL, Levey AS, Jones C, et al.
verting enzyme inhibitors due to cough in black subjects. Clin
Prevalence of high blood pressure and elevated serum creatinine level in
Pharmacol Ther. 1996;60:582–588. X
the United States: findings from the third National Health and Nutrition
212. Gottlieb SS, McCarter RJ, Vogel RA. Effect of beta-blockade on mor-
Examination Survey (1988 –1994). Arch Intern Med. 2001;161:
tality among high-risk and low-risk patients after myocardial infarction.
N Engl J Med. 1998;339:489 – 497. RE
194. Jafar TH, Schmid CH, Landa M, Giatras I, Toto R, Remuzzi G, et al.
213. Reaven GM. Pathophysiology of insulin resistance in human disease.
Angiotensin-converting enzyme inhibitors and progression of nondi-
Physiol Rev. 1995;75:473– 486. PR
abetic renal disease: a meta-analysis of patient-level data. Ann Intern
214. Esposito K, Pontillo A, Di Palo C, Giugliano G, Masella M, Marfella R,
Med. 2001;135:73– 87. M
et al. Effect of weight loss and lifestyle changes on vascular inflam-
195. Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, de Jong PE, et
matory markers in obese women: a randomized trial. JAMA. 2003;289:
al. Progression of chronic kidney disease: the role of blood pressure
control, proteinuria, and angiotensin-converting enzyme inhibition: a
215. Bastard JP, Pieroni L, Hainque B. Relationship between plasma plas-
patient-level meta-analysis. Ann Intern Med. 2003;139:244 –252. M
minogen activator inhibitor 1 and insulin resistance. Diabetes Metab Res
196. Wright JT Jr, Bakris G, Greene T, Agodoa LY, Appel LJ, Charleston J,
Rev. 2000;16:192–201. PR
et al. Effect of blood pressure lowering and antihypertensive drug class
216. Kunsch C, Medford RM. Oxidative stress as a regulator of gene
on progression of hypertensive kidney disease: results from the AASK
expression in the vasculature. Circ Res. 1999;85:753–766. PR
trial. JAMA. 2002;288:2421–2431. RA
217. Facchini FS, Hua NW, Reaven GM, Stoohs RA. Hyperinsulinemia: the
197. Tzourio C, Anderson C, Chapman N, Woodward M, Neal B, MacMahon
missing link among oxidative stress and age-related diseases? Free
S, et al. Effects of blood pressure lowering with perindopril and inda-
Radic Biol Med. 2000;29:1302–1306.
pamide therapy on dementia and cognitive decline in patients with
218. Rowley K, O'Dea K, Best JD. Association of albuminuria and the
cerebrovascular disease. Arch Intern Med. 2003;163:1069 –1075. RA
metabolic syndrome. Curr Diab Rep. 2003;3:80 – 86. PR
198. Adams HP Jr, Adams RJ, Brott T, del Zoppo GJ, Furlan A, Goldstein
LB, et al. Guidelines for the early management of patients with ischemic
219. Egan BM. Insulin resistance and the sympathetic nervous system. Curr
stroke: a scientific statement from the Stroke Council of the American
Hypertens Rep. 2003;5:247–254. PR
Stroke Association. Stroke. 2003;34 :1056 –1083. PR
220. Licata G, Scaglione R, Corrao S, Ganguzza A, Mazzola G, Arnone S, et al.
199. The National Institute of Neurological Disorders and Stroke rt-PA
Heredity and obesity-associated hypertension: impact of hormonal charac-
Stroke Study Group. Tissue plasminogen activator for acute ischemic
teristics and left ventricular mass. J Hypertens. 1995;13:611– 618. C
stroke. N Engl J Med. 1995;333:1581–1587. RA
221. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome
200. Cooper R, Rotimi C. Hypertension in blacks. Am J Hypertens. 1997;10:
among US adults: findings from the third National Health and Nutrition
Examination Survey. JAMA. 2002;287:356 –359. X
201. National Heart, Lung, and Blood Institute. Strong Heart Study Data
222. Park YW, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield
Book: A Report to American Indians Communities. Bethesda, MD:
SB. The metabolic syndrome: prevalence and associated risk factor
National Institutes of Health, National Heart, Lung, and Blood Institute.
findings in the US population from the Third National Health and
NIH Publication No. 01–3285, 2001. pp. 19. http://www.nhlbi.nih.gov/
Nutrition Examination Survey, 1988 –1994. Arch Intern Med. 2003;163:
202. Crespo CJ, Loria CM, Burt VL. Hypertension and other cardiovascular
223. Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E,
disease risk factors among Mexican Americans, Cuban Americans, and
Tuomilehto J, et al. The metabolic syndrome and total and cardiovas-
Puerto Ricans from the Hispanic Health and Nutrition Examination
cular disease mortality in middle-aged men. JAMA. 2002;288:
Survey. Public Health Rep. 1996;111:7–10.
203. Douglas JG, Bakris GL, Epstein M, Ferdinand KC, Ferrario C, Flack
224. Hsia J, Bittner V, Tripputi M, Howard BV. Metabolic syndrome and
JM, et al. Management of high blood pressure in African Americans:
coronary angiographic disease progression: the Women's Angiographic
consensus statement of the Hypertension in African Americans Working
Vitamin & Estrogen trial. Am Heart J. 2003;146:439 – 445.
Group of the International Society on Hypertension in Blacks. Arch
225. Laaksonen DE, Lakka HM, Niskanen LK, Kaplan GA, Salonen JT,
Intern Med. 2003;163:525–541. PR
Lakka TA. Metabolic syndrome and development of diabetes mellitus:
204. Hypertension Detection and Follow-up Program Cooperative Group.
application and validation of recently suggested definitions of the met-
Persistence of reduction in blood pressure and mortality of participants
abolic syndrome in a prospective cohort study. Am J Epidemiol. 2002;
in the Hypertension Detection and Follow-up Program. JAMA. 1988;
156:1070 –1077. F
259:2113–2122. F
226. Wilson PWF, D'Agostino RB, Parise H, Meigs JB. The metabolic
205. U S Department of Health and Human Services. Understanding and
syndrome as a precursor of cardiovascular disease and type 2 diabetes
improving health and objectives for improving health. Healthy People
mellitus. Diabetes. 2002;51:A242. F
Chobanian et al
JNC 7 – COMPLETE REPORT
227. National Institutes of Health. Clinical guidelines on the identification,
hypertension complicated by intermittent claudication. Lancet. 1987;2:
evaluation, and treatment of overweight and obesity in adults: the
evidence report. Obes Res. 1998;6:(suppl 2):51S–209S. PR
249. Solomon SA, Ramsay LE, Yeo WW, Parnell L, Morris-Jones W. Beta
228. Laaksonen DE, Lakka HM, Salonen JT, Niskanen LK, Rauramaa R,
blockade and intermittent claudication: placebo controlled trial of
Lakka TA. Low levels of leisure-time physical activity and cardiorespi-
atenolol and nifedipine and their combination. BMJ. 1991;303:
ratory fitness predict development of the metabolic syndrome. Diabetes
250. Radack K, Deck C. Beta-adrenergic blocker therapy does not worsen
229. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM,
intermittent claudication in subjects with peripheral arterial disease. A
Walker EA, et al. Reduction in the incidence of type 2 diabetes with
meta-analysis of randomized controlled trials. Arch Intern Med. 1991;
lifestyle intervention or metformin. Diabetes Prevention Program
151:1769 –1776. M
Research Group. N Engl J Med. 2002;346:393– 403. RA
251. Haynes WG, Lopez JAG, Mark AL. Treatment of hypertension
230. American Diabetes Association. Standards of medical care for patients
combined with cardiovascular disease. In: Smith TW (ed): Cardiovas-
with diabetes mellitus. Diabetes Care. 2002;25:S33–S49. PR
cular Therapeutics: A Companion to Braunwald's Heart Disease. Phil-
231. Field AE, Coakley EH, Must A, Spadano JL, Laird N, Dietz WH, et al.
adelphia, PA: WB Saunders; 1996. pp. 503–504. PR
Impact of overweight on the risk of developing common chronic diseases
252. Heart Protection Study Collaborative Group. MRC/BHF Heart Pro-
during a 10-year period. Arch Intern Med. 2001;161:1581–1586. F
tection Study of cholesterol lowering with simvastatin in 20,536
232. Gidding SS, Falkner B. Are we losing the game? Cardiovascular health
high-risk individuals: a randomised placebo-controlled trial. Lancet.
in minority children. Ethn Dis. 2002;12:171–173.
233. Strauss RS, Pollack HA. Epidemic increase in childhood overweight,
253. Olin JW. Treatment of hypertensive patients with peripheral arterial
1986 –1998. JAMA. 2001;286:2845–2848. X
disease. In: Izzo JL Jr, Black HR (eds): Hypertension Primer: The
234. He J, Ogden LG, Vupputuri S, Bazzano LA, Loria C, Whelton PK.
Essentials of High Blood Pressure: Basic Science, Population Science,
Dietary sodium intake and subsequent risk of cardiovascular disease in
and Clinical Management. Philadelphia, PA: Lippincott Williams &
overweight adults. JAMA. 1999;282:2027–2034. F
Wilkins; 2003. pp. 467– 469.
235. Wilson PW, Kannel WB, Silbershatz H, D'Agostino RB. Clustering of
254. Hiatt WR, Regensteiner JG, Hargarten ME, Wolfel EE, Brass EP.
metabolic factors and coronary heart disease. Arch Intern Med. 1999;
Benefit of exercise conditioning for patients with peripheral arterial
159:1104 –1109. F
disease. Circulation. 1990;81:602– 609.
236. Lee IM, Rexrode KM, Cook NR, Manson JE, Buring JE. Physical
255. U S. Census Bureau. Persons 65 Years Old and Over–Characteristics by
Sex: 1980 to 2000. Statistical Abstracts of the United States: 2002.
activity and coronary heart disease in women: is "no pain, no gain"
Washington, DC: U S Census Bureau; 2001. pp. 43.
passe? JAMA. 2001;285:1447–1454. F
256. Izzo JL Jr, Levy D, Black HR. Clinical Advisory Statement. Importance
237. Gregg EW, Cauley JA, Stone K, Thompson TJ, Bauer DC, Cummings
of systolic blood pressure in older Americans. Hypertension. 2000;35:
SR, et al. Relationship of changes in physical activity and mortality
among older women. JAMA. 2003;289:2379 –2386. F
257. Burt VL, Cutler JA, Higgins M, Horan MJ, Labarthe D, Whelton P, et
238. Stevens J, Cai J, Evenson KR, Thomas R. Fitness and fatness as
al. Trends in the prevalence, awareness, treatment, and control of hyper-
predictors of mortality from all causes and from cardiovascular disease
tension in the adult US population: data from the health examination
in men and women in the lipid research clinics study. Am J Epidemiol.
surveys, 1960 to 1991. Erratum in: Hypertension. 1996 May;27:1192.
2002;156:832– 841. F
Hypertension. 1995;26:60 – 69. X
239. Simons-Morton DG, Hogan P, Dunn AL, Pruitt L, King AC, Levine BD,
258. Staessen JA, Gasowski J, Wang JG, Thijs L, Den Hond E, Boissel JP, et
et al. Characteristics of inactive primary care patients: baseline data from
al. Risks of untreated and treated isolated systolic hypertension in the
the activity counseling trial. For the Activity Counseling Trial Research
elderly: meta-analysis of outcome trials. Lancet. 2000;355:865– 872. M
Group. Prev Med. 2000;31:513–521.
259. Gueyffier F, Bulpitt C, Boissel JP, Schron E, Ekbom T, Fagard R, et al.
240. Devereux R. Management of hypertensive patients with left ventricular
Antihypertensive drugs in very old people: a subgroup meta-analysis of
hypertrophy and diastolic dysfunction. In: Izzo J Jr, Black H (eds):
randomised controlled trials. INDANA Group. Lancet. 1999;353:
Hypertension Primer: The Essentials of High Blood Pressure: Basic
Science, Population Science, and Clinical Management. Philadelphia,
260. Jonsson PV, Lipsitz LA, Kelley M, Koestner J. Hypotensive responses
PA: Lippincott Williams & Wilkins; 2003. pp. 460 – 463.
to common daily activities in institutionalized elderly. A potential risk
241. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic
for recurrent falls. Arch Intern Med. 1990;150:1518 –1524. C
implications of echocardiographically determined left ventricular mass
261. Spence JD, Sibbald WJ, Cape RD. Pseudohypertension in the elderly.
in the Framingham Heart Study. N Engl J Med. 1990;322:1561–1566. F
Clin Sci Mol Med Suppl. 1978;55:399s– 402s. C
242. Okin PM, Wright JT, Nieminen MS, Jern S, Taylor AL, Phillips R, et al.
262. Nally J Jr. Management of renovascular hypertension. In: Izzo J Jr,
Ethnic differences in electrocardiographic criteria for left ventricular
Black H (eds): Hypertension Primer: The Essentials of High Blood
hypertrophy: the LIFE study. For the LIFE Study Investigators. Am J
Pressure: Basic Science, Population Science, and Clinical Management.
Hypertens. 2002;15:663– 671.
Philadelphia, PA: Lippincott Williams & Wilkins; 2003. pp. 500 –502.
243. Koren MJ, Mensah GA, Blake J, Laragh JH, Devereux RB. Comparison
263. Koch-Weser J. The therapeutic challenge of systolic hypertension.
of left ventricular mass and geometry in black and white patients with
N Engl J Med. 1973;289:481– 483.
essential hypertension. Am J Hypertens. 1993;6:815– 823.
264. Appel LJ, Espeland MA, Easter L, Wilson AC, Folmar S, Lacy CR.
244. Schmieder RE, Schlaich MP, Klingbeil AU, Martus P. Update on
Effects of reduced sodium intake on hypertension control in older
reversal of left ventricular hypertrophy in essential hypertension (a
individuals: results from the Trial of Nonpharmacologic Interventions in
meta-analysis of all randomized double-blind studies until December
the Elderly (TONE). Arch Intern Med. 2001;161:685– 693.
1996). Nephrol Dial Transplant. 1998;13:564 –569. M
265. Masaki KH, Schatz IJ, Burchfiel CM, Sharp DS, Chiu D, Foley D, et al.
245. Liebson PR, Grandits GA, Dianzumba S, Prineas RJ, Grimm RH Jr,
Orthostatic hypotension predicts mortality in elderly men: the Honolulu
Neaton JD, et al. Comparison of five antihypertensive monotherapies
Heart Program. Circulation. 1998;98:2290 –2295. F
and placebo for change in left ventricular mass in patients receiving
266. Mukai S, Lipsitz LA. Orthostatic hypotension. Clin Geriatr Med. 2002;
nutritional-hygienic therapy in the Treatment of Mild Hypertension
Study (TOMHS). Circulation. 1995;91:698 –706. RA
267. Ooi WL, Hossain M, Lipsitz LA. The association between orthostatic
246. Gottdiener JS, Reda DJ, Massie BM, Materson BJ, Williams DW,
hypotension and recurrent falls in nursing home residents. Am J Med.
Anderson RJ. Effect of single-drug therapy on reduction of left ventric-
ular mass in mild to moderate hypertension: comparison of six antihy-
268. Oster JR, Materson BJ. Pseudohypertension: a diagnostic dilemma.
pertensive agents. The Department of Veterans Affairs Cooperative
J Clin Hypertens. 1986;4:307–313.
Study Group on Antihypertensive Agents. Circulation. 1997;95:
269. Staessen JA, Wang J. Blood-pressure lowering for the secondary pre-
vention of stroke. Lancet. 2001;358:1026 –1027.
247. Coffman JD. Drug therapy: vasodilator drugs in peripheral vascular
270. Di Bari M, Pahor M, Franse LV, Shorr RI, Wan JY, Ferrucci L, et al.
disease. N Engl J Med. 1979;300:713–717. PR
Dementia and disability outcomes in large hypertension trials: lessons
248. Roberts DH, Tsao Y, McLoughlin GA, Breckenridge A. Placebo-
learned from the Systolic Hypertension in the Elderly Program (SHEP)
controlled comparison of captopril, atenolol, labetalol, and pindolol in
trial. Am J Epidemiol. 2001;153:72–78.
271. Reed DM, Resch JA, Hayashi T, MacLean C, Yano K. A prospective
294. Rosenthal T, Oparil S. Hypertension in women. J Hum Hypertens.
study of cerebral artery atherosclerosis. Stroke. 1988;19:820 – 825. F
2000;14:691–704. PR
272. Furuta A, Ishii N, Nishihara Y, Horie A. Medullary arteries in aging and
295. Wolz M, Cutler J, Roccella EJ, Rohde F, Thom T, Burt V. Statement
dementia. Stroke. 1991;22:442– 446. C
from the National High Blood Pressure Education Program: prevalence
273. Dozono K, Ishii N, Nishihara Y, Horie A. An autopsy study of the
of hypertension. Am J Hypertens. 2000;13:103–104. X
incidence of lacunes in relation to age, hypertension, and arteriosclero-
296. Staessen J, Bulpitt CJ, Fagard R, Lijnen P, Amery A. The influence of
sis. Stroke. 1991;22:993–996. RE
menopause on blood pressure. J Hum Hypertens. 1989;3:427– 433. RA
274. Leung SY, Ng TH, Yuen ST, Lauder IJ, Ho FC. Pattern of cerebral
297. Staessen JA, Ginocchio G, Thijs L, Fagard R. Conventional and ambu-
atherosclerosis in Hong Kong Chinese: severity in intracranial and
latory blood pressure and menopause in a prospective population study.
extracranial vessels. Stroke. 1993;24:779 –786. PR
J Hum Hypertens. 1997;11:507–514. F
275. Schmidt R, Fazekas F, Koch M, Kapeller P, Augustin M, Offenbacher
298. Calhoun DA, Oparil S. Gender and blood pressure. In: Izzo JL Jr, Black
H, et al. Magnetic resonance imaging cerebral abnormalities and neu-
HR (eds): Hypertension Primer: The Essentials of High Blood Pressure:
ropsychologic test performance in elderly hypertensive subjects: a case-
Basic Science, Population Science, and Clinical Management. Phila-
control study. Arch Neurol. 1995;52:905–910. RE
delphia, PA: Lippincott Williams & Wilkins; 2003. pp. 253–257. PR
276. Longstreth WT Jr, Manolio TA, Arnold A, Burke GL, Bryan N, Jungreis
299. Manson JE, Hsia J, Johnson KC, Rossouw JE, Assaf AR, Lasser NL, et
CA, et al. Clinical correlates of white matter findings on cranial
al. Estrogen plus progestin and the risk of coronary heart disease. N Engl
magnetic resonance imaging of 3301 elderly people. The Cardiovascular
J Med. 2003;349:523–534. RA
Health Study Collaborative Research Group. Stroke. 1996;27:
300. Wassertheil-Smoller S, Anderson G, Psaty BM, Black HR, Manson J,
Wong N, et al. Hypertension and its treatment in postmenopausal
277. Awada A, Omojola MF. Leuko-araiosis and stroke: a case-control study.
women: baseline data from the Women's Health Initiative. Hyper-
Acta Neurol Scand. 1996;94:415– 418. RE
tension. 2000;36:780 –789.
278. Swan GE, DeCarli C, Miller BL, Reed T, Wolf PA, Jack LM, et al.
301. The Writing Group for the PEPI Trial. Effects of estrogen or estrogen/
Association of midlife blood pressure to late-life cognitive decline and
progestin regimens on heart disease risk factors in postmenopausal
brain morphology. Neurology. 1998;51:986 –993. F
women. The Postmenopausal Estrogen/Progestin Interventions (PEPI)
279. Koga H, Yuzuriha T, Yao H, Endo K, Hiejima S, Takashima Y, et al.
Trial. JAMA. 1995;273:199 –208. RA
Quantitative MRI findings and cognitive impairment among community
302. Chasan-Taber L, Willett WC, Manson JE, Spiegelman D, Hunter DJ,
dwelling elderly subjects. J Neurol Neurosurg Psychiatry. 2002;72:
Curhan G, et al. Prospective study of oral contraceptives and hyper-
tension among women in the United States. Circulation. 1996;94:
280. Del Bigio MR, Yan HJ, Kozlowski P, Sutherland GR, Peeling J. Serial
magnetic resonance imaging of rat brain after induction of renal hyper-
303. Gueyffier F, Boutitie F, Boissel JP, Pocock S, Coope J, Cutler J, et al.
tension. Stroke. 1999;30:2440 –2447.
Effect of antihypertensive drug treatment on cardiovascular outcomes in
281. Awad IA, Johnson PC, Spetzler RF, Hodak JA. Incidental subcortical
women and men: a meta-analysis of individual patient data from ran-
lesions identified on magnetic resonance imaging in the elderly, II:
domized, controlled trials. The INDANA Investigators. Ann Intern Med.
postmortem pathological correlations. Stroke. 1986;17:1090 –1097.
1997;126:761–767. M
282. Marshall VG, Bradley WG Jr, Marshall CE, Bhoopat T, Rhodes RH.
304. Staessen JA, Fagard R, Thijs L, Celis H, Birkenhager WH, Bulpitt CJ,
Deep white matter infarction: correlation of MR imaging and his-
et al. Subgroup and per-protocol analysis of the randomized European
topathologic findings. Radiology. 1988;167:517–522. F
Trial on Isolated Systolic Hypertension in the Elderly. Arch Intern Med.
283. Estes ML, Chimowitz MI, Awad IA, McMahon JT, Furlan AJ, Ratliff
1998;158:1681–1691. RA
NB. Sclerosing vasculopathy of the central nervous system in nonelderly
305. Lewis CE, Grandits A, Flack J, McDonald R, Elmer PJ. Efficacy and
demented patients. Arch Neurol. 1991;48:631– 636. RE
tolerance of antihypertensive treatment in men and women with stage 1
284. Chimowitz MI, Estes ML, Furlan AJ, Awad IA. Further observations on
diastolic hypertension: results of the Treatment of Mild Hypertension
the pathology of subcortical lesions identified on magnetic resonance
Study. Arch Intern Med. 1996;156:377–385. RA
imaging. Arch Neurol. 1992;49 :747–752. RE
306. Taler SJ. Treatment of pregnant hypertensive patients. In: Izzo JL Jr, Black
285. Baloh RW, Vinters HV. White matter lesions and disequilibrium in
HR (eds): Hypertension Primer: The Essentials of High Blood Pressure:
older people, II: clinicopathologic correlation. Arch Neurol. 1995;52:
Basic Science, Population Science, and Clinical Management. Philadelphia,
PA: Lippincott Williams & Wilkins; 2003. pp. 491– 493. PR
286. Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins PV, et al.
307. von Dadelszen P, Ornstein MP, Bull SB, Logan AG, Koren G, Magee
Current concepts in mild cognitive impairment. Arch Neurol. 2001;58:
LA. Fall in mean arterial pressure and fetal growth restriction in
pregnancy hypertension: a meta-analysis. Lancet. 2000;355:87–92. M
287. Glynn RJ, Beckett LA, Hebert LE, Morris MC, Scherr PA, Evans DA.
308. Buchbinder A, Sibai BM, Caritis S, Macpherson C, Hauth J, Lindheimer
Current and remote blood pressure and cognitive decline. JAMA. 1999;
MD, et al. Adverse perinatal outcomes are significantly higher in severe
281:438 – 445. F
gestational hypertension than in mild preeclampsia. Am J Obstet
288. Sacktor N, Gray S, Kawas C, Herbst J, Costa P, Fleg J. Systolic blood
Gynecol. 2002;186:66 –71. RE
pressure within an intermediate range may reduce memory loss in an
309. ACOG Practice Bulletin. Chronic hypertension in pregnancy. ACOG
elderly hypertensive cohort. J Geriatr Psychiatry Neurol. 1999;12:1– 6.
Committee on Practice Bulletins. Obstet Gynecol. 2001;98:177–185. PR
310. Sibai BM. Treatment of hypertension in pregnant women. N Engl J Med.
289. Kivipelto M, Helkala EL, Hanninen T, Laakso MP, Hallikainen M,
1996;335:257–265. PR
Alhainen K, et al. Midlife vascular risk factors and late-life mild cog-
311. National High Blood Pressure Education Program. Update on the 1987
nitive impairment: a population-based study. Neurology. 2001;56:
Task Force Report on High Blood Pressure in Children and Adolescents:
A working group report from the National High Blood Pressure Edu-
290. Dufouil C, de Kersaint-Gilly A, Besancon V, Levy C, Auffray E,
cation Program. National High Blood Pressure Education Program
Brunnereau L, et al. Longitudinal study of blood pressure and white
Working Group on Hypertension Control in Children and Adolescents.
matter hyperintensities: the EVA MRI Cohort. Neurology. 2001;56:
Pediatrics. 1996;98:649 – 658. PR
312. Calhoun DA. Hypertensive crisis. In: Oparil S, Weber MA (eds): Hyper-
291. Yamaguchi S, Kobayashi S, Okada K, Koide H, Bokura H, Tsuchiya H,
tension: A Companion to Brenner and Recot's The Kidney. Philadelphia,
et al. Cognitive decline associated with worsening of white matter
PA: WB Saunders Co.; 2000. pp. 715–718. PR
lesions: a 6-year follow-up study. J Stroke Cerebrovasc Dis. 1996;6:
313. Vidt DG. Management of hypertensive urgencies and emergencies. In:
Izzo JL Jr, Black HR (eds): Hypertension Primer: The Essentials of
292. Schmidt R, Fazekas F, Kapeller P, Schmidt H, Hartung HP. MRI white
High Blood Pressure. Dallas, TX: American Heart Association; 1999.
matter hyperintensities: three-year follow-up of the Austrian Stroke
pp. 437– 440. PR
Prevention Study. Neurology. 1999;53:132–139. F
314. Vidt DG. Emergency room management of hypertensive urgencies and
293. Forette F, Seux ML, Staessen JA, Thijs L, Birkenhager WH, Babar-
emergencies. J Clin Hypertens (Greenwich). 2001;3:158 –164. PR
skiene MR, et al. Prevention of dementia in randomised double-blind
315. Zampaglione B, Pascale C, Marchisio M, Cavallo-Perin P. Hypertensive
placebo-controlled Systolic Hypertension in Europe (Syst-Eur) trial.
urgencies and emergencies: prevalence and clinical presentation. Hyper-
Lancet. 1998;352:1347–1351. RA
tension. 1996;27:144 –147. X
Chobanian et al
JNC 7 – COMPLETE REPORT
316. Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Glasser DB,
resistance vessels in patients with obstructive sleep apnea. Circulation.
Rimm EB. Sexual function in men older than 50 years of age: results
2000;102:2607–2610. C
from the Health Professionals Follow-Up Study. Ann Intern Med. 2003;
339. Javaheri S, Parker TJ, Liming JD, Corbett WS, Nishiyama H, Wexler L,
et al. Sleep apnea in 81 ambulatory male patients with stable heart
317. Della Chiesa A, Pfiffner D, Meier B, Hess OM. Sexual activity in
failure: types and their prevalences, consequences, and presentations.
hypertensive men. J Hum Hypertens. 2003;17:515–521. RA
Circulation. 1998;97:2154 –2159. F
318. Fogari R, Zoppi A, Poletti L, Marasi G, Mugellini A, Corradi L. Sexual
340. Kaneko Y, Floras JS, Usui K, Plante J, Tkacova R, Kubo T, et al.
activity in hypertensive men treated with valsartan or carvedilol: a
Cardiovascular effects of continuous positive airway pressure in patients
crossover study. Am J Hypertens. 2001;14:27–31. RA
with heart failure and obstructive sleep apnea. N Engl J Med. 2003;348:
319. Kloner RA, Brown M, Prisant LM, Collins M. Effect of sildenafil in
patients with erectile dysfunction taking antihypertensive therapy. Sil-
341. Leung RS, Bradley TD. Sleep apnea and cardiovascular disease. Am J
denafil Study Group. Am J Hypertens. 2001;14:70 –73. RA
Respir Crit Care Med. 2001;164:2147–2165. PR
320. Kirby RS. Doxazosin in benign prostatic hyperplasia: effects on blood
342. Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et
pressure and urinary flow in normotensive and hypertensive men.
al. Sleep-disordered breathing and cardiovascular disease: cross-
Urology. 1995;46:182–186. RA
sectional results of the Sleep Heart Health Study. Am J Respir Crit Care
321. Eagle KA, Berger PB, Calkins H, Chaitman BR, Ewy GA, Fleischmann
Med. 2001;163:19 –25. X
KE, et al. ACC/AHA guideline update for perioperative cardiovascular
343. Kanagala R, Murali NS, Friedman PA, Ammash NM, Gersh BJ,
evaluation for noncardiac surgery: executive summary: a report of the
Ballman KV, et al. Obstructive sleep apnea and the recurrence of atrial
American College of Cardiology/American Heart Association Task
fibrillation. Circulation. 2003;107:2589 –2594. F
Force on Practice Guidelines (Committee to Update the 1996 Guidelines
344. Dyken ME, Somers VK, Yamada T, Ren ZY, Zimmerman MB. Inves-
on Perioperative Cardiovascular Evaluation for Noncardiac Surgery).
tigating the relationship between stroke and obstructive sleep apnea.
Circulation. 2002;105:1257–1267. PR
Stroke. 1996;27:401– 407. F
322. Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on
345. Levinson PD, McGarvey ST, Carlisle CC, Eveloff SE, Herbert PN,
mortality and cardiovascular morbidity after noncardiac surgery. Mul-
Millman RP. Adiposity and cardiovascular risk factors in men with
ticenter Study of Perioperative Ischemia Research Group. N Engl J Med.
obstructive sleep apnea. Chest. 1993;103:1336 –1342. C
1996;335:1713–1720. RA
346. Millman RP, Carlisle CC, McGarvey ST, Eveloff SE, Levinson PD.
323. Vidt DG. Treatment of hypertensive emergencies and urgencies. In: Izzo
Body fat distribution and sleep apnea severity in women. Chest. 1995;
JL Jr, Black HR, Goodfriend TL (eds): Hypertension Primer: The
Essentials of High Blood Pressure: Basic Science, Population Science,
347. Newman AB, Nieto FJ, Guidry U, Lind BK, Redline S, Shahar E, et al.
and Clinical Management. Philadelphia, PA: Lippincott Williams &
Relation of sleep-disordered breathing to cardiovascular disease risk factors:
Wilkins;2003. pp. 452– 459. PR
the Sleep Heart Health Study. Am J Epidemiol. 2001;154:50 –59. X
324. Alper A, Calhoun D. Hypertensive emergencies. In: Antman EM (ed):
348. Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. Longitudinal
Cardiovascular Therapeutics: A Companion to Braunwald's Heart
study of moderate weight change and sleep-disordered breathing. JAMA.
Disease. Philadelphia, PA: WB Saunders Co; 2002. pp. 817– 831. PR
2000;284:3015–3021. F
325. Bader JD, Bonito AJ, Shugars DA. A systematic review of cardiovas-
349. Phillips BG, Kato M, Narkiewicz K, Choe I, Somers VK. Increases in
cular effects of epinephrine on hypertensive dental patients. Oral Surg
leptin levels, sympathetic drive, and weight gain in obstructive sleep
Oral Med Oral Pathol Oral Radiol Endod. 2002;93:647– 653. PR
apnea. Am J Physiol Heart Circ Physiol. 2000;279:H234 –H237. C
326. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The
350. Chin K, Shimizu K, Nakamura T, Narai N, Masuzaki H, Ogawa Y, et al.
occurrence of sleep-disordered breathing among middle-aged adults.
Changes in intra-abdominal visceral fat and serum leptin levels in
N Engl J Med. 1993;328:1230 –1235. X
patients with obstructive sleep apnea syndrome following nasal con-
327. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the
tinuous positive airway pressure therapy. Circulation. 1999;100:
association between sleep-disordered breathing and hypertension.
N Engl J Med. 2000;342:1378 –1384. F
351. Kato M, Phillips BG, Sigurdsson G, Narkiewicz K, Pesek CA, Somers
328. Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, et al.
VK. Effects of sleep deprivation on neural circulatory control. Hyper-
Association of sleep-disordered breathing, sleep apnea, and hyper-
tension. 2000;35:1173–1175. C
tension in a large community-based study. Sleep Heart Health Study.
352. Spiegel K, Leproult R, Van Cauter E. Impact of sleep debt on metabolic
JAMA. 2000;283:1829 –1836. X
and endocrine function. Lancet. 1999;354:1435–1439. C
329. Young T, Peppard P, Palta M, Hla KM, Finn L, Morgan B, et al.
353. Faccenda JF, Mackay TW, Boon NA, Douglas NJ. Randomized
Population-based study of sleep-disordered breathing as a risk factor for
placebo-controlled trial of continuous positive airway pressure on blood
hypertension. Arch Intern Med. 1997;157:1746 –1752. F
pressure in the sleep apnea-hypopnea syndrome. Am J Respir Crit Care
330. Bradley TD, Floras JS. Sleep apnea and heart failure, part I: obstructive
Med. 2001;163:344 –348. RA
sleep apnea. Circulation. 2003;107:1671–1678. PR
354. Somers VK. Management of sleep apnea. In: Izzo JL Jr, Black HR (eds):
331. Dart RA, Gregoire JR, Gutterman DD, Woolf SH. The association of
Hypertension Primer: The Essentials of High Blood Pressure: Basic
hypertension and secondary cardiovascular disease with sleep-
Science, Population Science, and Clinical Management. Philadelphia,
disordered breathing. Chest. 2003;123:244 –260. M
PA: Lippincott Williams & Wilkins; 2003. pp. 512–516. PR
332. Wolk R, Kara T, Somers VK. Sleep-disordered breathing and cardio-
355. Becker HF, Jerrentrup A, Ploch T, Grote L, Penzel T, Sullivan CE, et al.
vascular disease. Circulation. 2003;108:9 –12.
Effect of nasal continuous positive airway pressure treatment on blood
333. Morgan BJ. Pathophysiology of sleep apnea. In: Izzo JL Jr, Black H
pressure in patients with obstructive sleep apnea. Circulation. 2003;107:
(eds): Hypertension Primer: The Essentials of High Blood Pressure:
Basic Science, Population Science, and Clinical Management. Phila-
356. Franklin KA, Nilsson JB, Sahlin C, Naslund U. Sleep apnoea and
delphia, PA: Lippincott Williams & Wilkins; 2003. pp. 156 –158. PR
nocturnal angina. Lancet. 1995;345:1085–1087. C
334. Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural
357. Peled N, Abinader EG, Pillar G, Sharif D, Lavie P. Nocturnal ischemic
mechanisms in obstructive sleep apnea. J Clin Invest. 1995;96:1897–1904.
events in patients with obstructive sleep apnea syndrome and ischemic
335. Shamsuzzaman AS, Winnicki M, Lanfranchi P, Wolk R, Kara T,
heart disease: effects of continuous positive air pressure treatment. J Am
Accurso V, et al. Elevated C-reactive protein in patients with obstructive
Coll Cardiol. 1999;34:1744 –1749. C
sleep apnea. Circulation. 2002;105:2462–2464. C
358. Wang JJ, Mitchell P, Leung H, Rochtchina E, Wong TY, Klein R.
336. Vgontzas AN, Papanicolaou DA, Bixler EO, Hopper K, Lotsikas A, Lin
Hypertensive retinal vessel wall signs in a general older population: the
HM, et al. Sleep apnea and daytime sleepiness and fatigue: relation to
Blue Mountains Eye Study. Hypertension. 2003;42:534 –541.
visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endo-
359. Wong TY, Klein R, Sharrett AR, Manolio TA, Hubbard LD, Marino
crinol Metab. 2000;85:1151–1158. C
EK, et al. The prevalence and risk factors of retinal microvascular
337. Punjabi NM, Sorkin JD, Katzel LI, Goldberg AP, Schwartz AR, Smith
abnormalities in older persons: The Cardiovascular Health Study. Oph-
PL. Sleep-disordered breathing and insulin resistance in middle-aged
thalmology. 2003;110:658 – 666.
and overweight men. Am J Respir Crit Care Med. 2002;165:677– 682. C
360. American Academy of Ophthalmology. Basic and Clinical Science
338. Kato M, Roberts-Thomson P, Phillips BG, Haynes WG, Winnicki M,
Course, Section 12, 1999 –2000. San Francisco, CA: American
Accurso V, et al. Impairment of endothelium-dependent vasodilation of
Academy of Ophthalmology; 1999. pp. 68 –70.
361. Textor SC. Hypertension and transplantation. In: Izzo JL Jr, Black HR
373. Sowers JR, White WB, Pitt B, Whelton A, Simon L, van Ingen H, et al.
(eds): Hypertension Primer: The Essentials of High Blood Pressure:
Rofecoxib, but not celecoxib or naproxen, increases mean 24-hour
Basic Science, Population Science, and Clinical Management. Phila-
systolic blood pressure in treated hypertensive patients with osteoar-
delphia, PA: Lippincott Williams & Wilkins; 2003. pp. 163–165. PR
thritis and type 2 diabetes mellitus. J Am Coll Cardiol. 2003;41:320A.
362. Canzanello VJ. Management of posttransplant hypertension. In: Izzo JL Jr,
Black HR (eds): Hypertension Primer: The Essentials of High Blood
374. Barrier PA, Li JT, Jensen NM. Two words to improve physician-patient
Pressure: Basic Science, Population Science, and Clinical Management.
communication: What else? Mayo Clin Proc. 2003;78:211–214. PR
Philadelphia, PA: Lippincott Williams & Wilkins; 2003. pp. 519 –522. PR
375. Herzlinger RE. Market-Driven Health Care: Who Wins, Who Loses in
the Transformation of America's Largest Service Industry. Reading,
363. Textor SC. Renal failure related to angiotensin-converting enzyme in-
MA: Addison-Wesley Publishing Co; 1997. pp. 65–75, 231.
hibitors. Semin Nephrol. 1997;17:67–76. PR
376. Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL,
364. Appel RG, Bleyer AJ, Reavis S, Hansen KJ. Renovascular disease in
et al. Clinical inertia. Ann Intern Med. 2001;135:825– 834.
older patients beginning renal replacement therapy. Kidney Int. 1995;
377. Balas EA, Weingarten S, Garb CT, Blumenthal D, Boren SA, Brown
GD. Improving preventive care by prompting physicians. Arch Intern
365. Bonelli FS, McKusick MA, Textor SC, Kos PB, Stanson AW, Johnson
Med. 2000;160:301–308. C
CM, et al. Renal artery angioplasty: technical results and clinical
378. Boulware LE, Daumit GL, Frick KD, Minkovitz CS, Lawrence RS,
outcome in 320 patients. Mayo Clin Proc. 1995;70:1041–1052. RE
Powe NR. An evidence-based review of patient-centered behavioral
366. Sos TA. Angioplasty for the treatment of azotemia and renovascular
interventions for hypertension. Am J Prev Med. 2001;21:221–232.
hypertension in atherosclerotic renal artery disease. Circulation. 1991;
83(Suppl I):I-162–I-166. F
379. Hill MN, Miller NH. Compliance enhancement: a call for multidisci-
367. Harden PN, MacLeod MJ, Rodger RS, Baxter GM, Connell JM,
plinary team approaches. Circulation. 1996;93:4 – 6.
Dominiczak AF, et al. Effect of renal-artery stenting on progression of
380. Maue SK, Rivo ML, Weiss B, Farrelly EW, Brower-Stenger S. Effect of
renovascular renal failure. Lancet. 1997;349:1133–1136. C
a primary care physician-focused, population-based approach to blood
368. Johnson AG, Nguyen TV, Day RO. Do nonsteroidal anti-inflammatory
pressure control. Fam Med. 2002;34:508 –513. F
drugs affect blood pressure? A meta-analysis. Ann Intern Med. 1994;
381. Shih SC, Bost JE, Pawlson LG. Standardized health plan reporting in
121:289 –300. M
four areas of preventive health care. Am J Prev Med. 2003;24:293–300.
369. Whelton A. Nephrotoxicity of nonsteroidal anti-inflammatory drugs:
382. Betancourt JR, Carrillo JE, Green AR. Hypertension in multicultural and
physiologic foundations and clinical implications. Am J Med. 1999;106:
minority populations: linking communication to compliance. CurrHypertens Rep. 1999;1:482– 488.
383. Weir MR, Maibach EW, Bakris GL, Black HR, Chawla P, Messerli
370. Whelton A, White WB, Bello AE, Puma JA, Fort JG. Effects of
FH, et al. Implications of a health lifestyle and medication analysis
celecoxib and rofecoxib on blood pressure and edema in patients ⬎ or
for improving hypertension control. Arch Intern Med. 2000;160:
65 years of age with systemic hypertension and osteoarthritis. Am J
Cardiol. 2002;90:959 –963. RA
384. Emmons KM, Rollnick S. Motivational interviewing in health care
371. White WB, Kent J, Taylor A, Verburg KM, Lefkowith JB, Whelton
settings: opportunities and limitations. Am J Prev Med. 2001;20:68 –74.
A. Effects of celecoxib on ambulatory blood pressure in hypertensive
385. Bandura A. Social Learning Theory. Englewood Cliffs, NJ: Prentice
patients on ACE inhibitors. Hypertension. 2002;39:929 –934. RA
372. Whelton A, Fort JG, Puma JA, Normandin D, Bello AE, Verburg
386. Pignone MP, Ammerman A, Fernandez L, Orleans CT, Pender N, Woolf
KM. Cyclooxygenase-2–specific inhibitors and cardiorenal function:
S, et al. Counseling to promote a healthy diet in adults: a summary of the
a randomized, controlled trial of celecoxib and rofecoxib in older
evidence for the U. S. Preventive Services Task Force. Am J Prev Med.
hypertensive osteoarthritis patients. Am J Ther. 2001;8:85–95. RA
2003;24:75–92. PR
Source: https://pri.rn.dk/Assets/6042/JNC7-Guidelines.pdf
N e w s l e t t e r vol. 10, no. 4 - 2007 "the recent initiative of EU Commission to identify "lead markets for biobased products" has shown that there is a need for realistic surveys in the EU-markets for RRMs and RRM based products.In the last edition of Green Tech letters 3/2007 the French Agency ADEME published the results of the ALCIMED survey on existing markets and future perspectives in France.
for International 13.10.2010 12:54:31 Uhr for International © DAAD, as for October 2010, no updates within the PDF version! Publisher DAADDeutscher Akademischer AustauschdienstGerman Academic Exchange ServiceKennedyallee 50, 53175 Bonn (Germany)www.daad.de Section: Promotion of Study and Research in Germany Project Coordination Dr. Ursula Egyptien Gad, Anne Münkel, Silvia Schmid

