Osteo-489 390.406
Osteoporos Int (1997) 7:390–406
ß 1997 European Foundation for Osteoporosis and the National Osteoporosis Foundation
Position Paper
Guidelines for Diagnosis and Management of Osteoporosis
J. A. Kanis, P. Delmas, P. Burckhardt, C. Cooper and D. Torgerson
on behalf of the European Foundation for Osteoporosis and Bone Disease
Preamble. Significant developments have occurred in
The clinical significance of osteoporosis lies in the
the field of osteoporosis over the past several years.
fractures that arise. Common fractures include vertebral
There is now considerable information concerning its
compression fractures, and fractures of the distal radius
impact on general health and an international consensus
and the proximal femur (hip fracture). In addition, when
concerning the definition of osteoporosis. Conceptually,
the skeleton is osteoporotic, fractures occur more
this recognizes the multifactorial nature of the events
commonly at many other sites including the pelvis,
which give rise to the fractures, but operational
proximal humerus, distal femur and ribs. Osteoporotic
definitions have now been agreed and have gained a
fractures occurring at the spine and the forearm are
wide measure of acceptance. Accurate and precise
associated with significant morbidity, but the most
diagnostic tools are also available. Finally, there is
serious consequences arise in patients with hip fracture,
substantial evidence that the natural history of osteo-
which is associated with a significant increase in
porosis can be modulated by agents which in turn
mortality (15–20%), particularly in elderly men and
decrease the risk of fracture.
women. Hip fractures account for more than 20% of
Despite an increasing professional and public aware-
orthopaedic bed occupancy in the UK, in Scandinavia
ness of osteoporosis, the management of osteoporosis
and several other countries. After the age of 45 years, hip
has been confined mainly to specialists. With the large
fractures account for a higher proportion of hospital bed
number of affected individuals and the wider availability
occupancy than many other common disorders in
of diagnostic aids and safe treatments, there is a need for
women, including breast cancer and diabetes (Fig. 1).
osteoporosis to be managed predominantly by theprimary care physician. Against this background theEuropean Foundation for Osteoporosis and Bone Diseasethrough their Scientific Advisory Board has recognized aneed to develop practice guidelines for primary carephysicians which are summarized in this paper.
The internationally agreed definition of osteoporosis is:‘a progressive systemic skeletal disease characterized bylow bone mass and microarchitectural deterioration ofbone tissue, with a consequent increase in bone fragilityand susceptibility to fracture' [1].
———————
Correspondence and offprint requests to: Professor John A. Kanis,WHO Collaborating Centre for Metabolic Bone Diseases, Department
Fig. 1. Hospital bed occupancy in women aged 45 years or more
of Human Metabolism & Clinical Biochemistry, University of
according to diagnostic category in the Trent Region of England (9%
Sheffield Medical School, Beech Hill Road, Sheffield S10 2RX,
of the UK population). COAD, chronic obstructive airways disease;
UK. Tel: +44 (0)114 271 2649. Fax: +44 (0)114 273 9176.
MI, myocardial infarction. (Source: Trent Health.)
Guidelines for Diagnosis and Management of Osteoporosis
Table 1. Estimated remaining life-time fracture risk (%) with
measured as bone mineral that can presently be
confidence intervals in women and men from Rochester, MN, USA
measured with precision and accuracy, and its measure-
at the age of 50 years
ment forms the basis for the diagnosis of osteoporosis.
Techniques to Measure Bone Mineral
There are two widely utilized techniques to assess bonemass. They variously assess mineral content of regional
From Melton LJ, Atkinson EJ, O'Fallon WM, Wahner HW, Riggs BL.
sites, particularly those sites at risk of osteoporotic
Long-term fracture risk prediction with bone mineral measurements
fracture such as the wrist, spine and hip, but also the
made at various skeletal sites. J Bone Miner Res 1991;6 (Suppl 1):S136.
whole skeleton.
aClinically diagnosed fractures.
Single-Energy Absorptiometry. The technique measuresbone mineral at peripheral (appendicular) sites such as
The likelihood that any individual will suffer an
the heel and the wrist. Single photon absorptiometry
osteoporotic fracture is considerable. In many Western
(SPA) utilizes a photon-emitting source such as iodine-
countries the remaining life-time risk of a hip fracture in
125, and the amount of bone mineral in the tissue
white women at the age of menopause lies between 15%
traversed attenuates the photons from which the mineral
and 17%. The risk for other common types of
content is calculated. Single-energy X-ray absorptiome-
osteoporotic fractures is nearly as high (Table 1), so
try (SXA) has now supplanted SPA as the single-energy
that the combined fracture risk is 30–40%. Thus, more
technique for scanning the wrist. It is more precise and
than one third of adult women will sustain one or more
avoids the need for isotopes.
osteoporotic fractures in their life-time. This estimate isconservative since it does not include fractures at other
Dual-Energy Absorptiometry. Sites such as the spine and
sites and only takes into account those vertebral fractures
hip cannot be measured accurately by SPA or SXA.
which come to clinical attention, so that the true risk of
Dual-energy absorptiometry utilizing photons (DPA) or
fracture is higher.
X-rays (DXA) permits bone mineral to be measured at
These indices of fracture risk compare with a life-time
these sites.
risk in women at the age of 50 years of 9–12% for breastcancer and 30–40% for cardiovascular disease. This
The amount of bone mineral present at a specific site of a
indicates the widespread prevalence of osteoporosis in
scan is termed the bone mineral content. When the bone
our society. In comparison, risks for men are about one-
mineral content is divided by the area or volume
third of those in women, and are even lower for forearm
assessed (the region of interest), a value for bone
fractures, but still represent a considerable burden.
mineral density is provided. With single- and dual-
The increasing awareness of osteoporosis combined
energy absorptiometry the bone mineral content is
with the current availability and development of specific
divided by the area assessed (because of the two-
treatments is likely to increase the demand for manage-
dimensional scan) and is not, therefore, a true volumetric
ment of patients with osteoporosis. In the past the
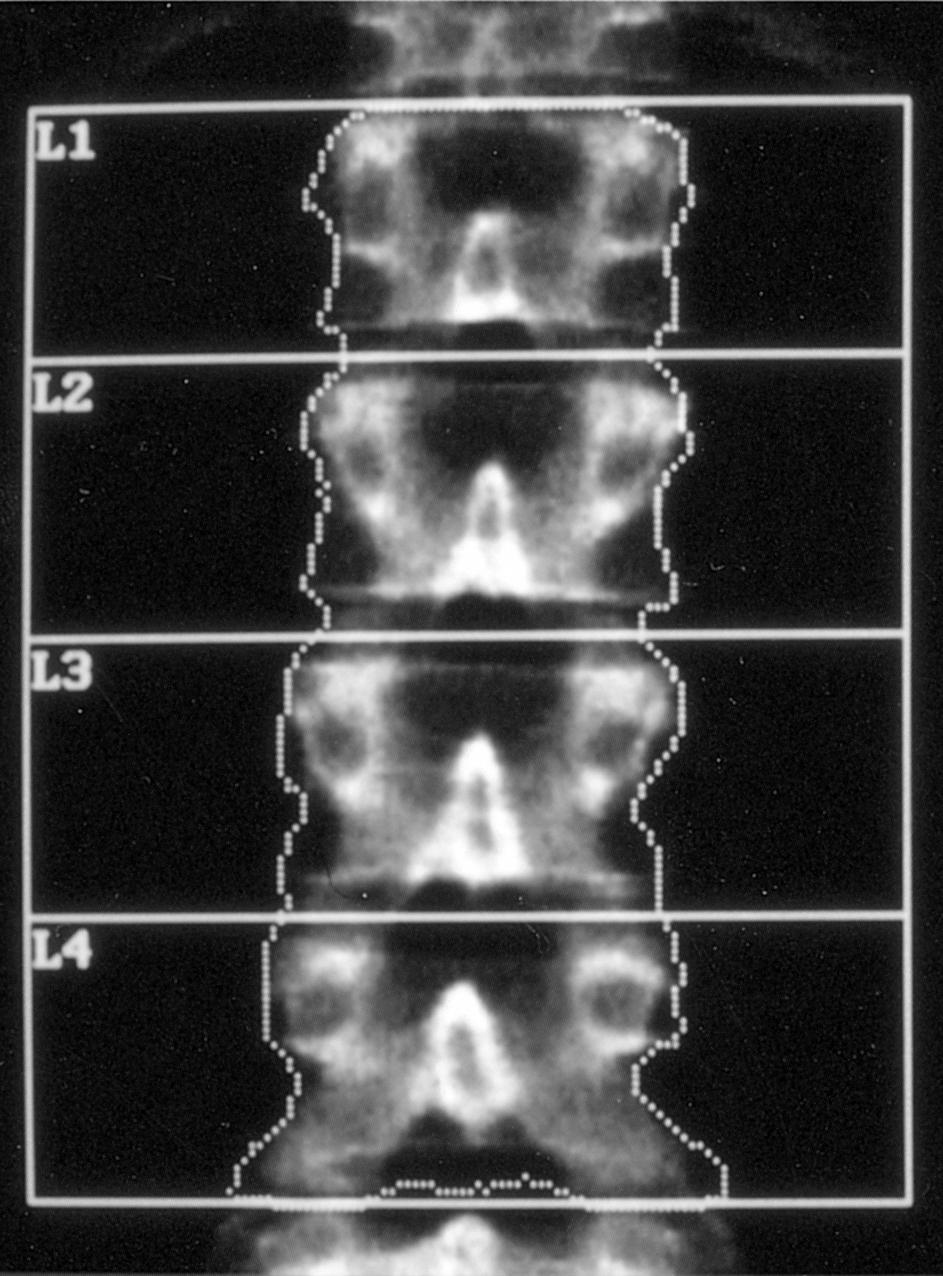
density but an areal density. A typical scan of the lumbar
management has been largely confined to specialists, but
spine is shown in Fig. 2 and an analysis in Table 2.
the increasing availability of diagnostic tools and well-
Several other techniques have been developed to
proven treatments, and the increasing numbers of
measure bone mineral, but their use is less widespread
patients identified, indicate that the burden of manag-
and in some cases confined to clinical research. They
ment will fall increasingly on the primary care physician.
include quantitative computed tomography, ultrasound
The aim of this document is to provide a framework for
evaluation of bone and several radiographic techniques
the cost-effective diagnosis and management of osteo-
including radiographic density measurements at the
porosis. These guidelines do not consider the identifica-
hand. Note that standard skeletal radiographs are a
tion of patients at risk from osteoporosis and strategies
very inaccurate method of assessing the amount of bone
for prevention of the disease, though in many respects
mineral, but apparent osteoporosis on X-rays is a
the approaches are similar.
common reason for further assessment. The majorlimitations of computed tomography at the spine arethe expense, low precision and comparatively high
Diagnosis of Osteoporosis
radiation dose. Computed tomography techniques toassess bone mineral density at appendicular sites are
The definition of osteoporosis captures the notion that
used in some countries with lower cost and radiation
low bone mass is an important component of the risk of
exposure and higher precision. Ultrasound attenuation
fracture, but that other abnormalities occur in the
and velocity measurements avoid exposure to radiation.
skeleton, and that non-skeletal factors such as falls are
They may be useful as a diagnostic aid, but their value in
also important. Nevertheless, it is only bone mass
monitoring treatments is not yet established.
J. A. Kanis et al.
adults (‘peak bone mass') is approximately normalirrespective of the technique used. Because of thisnormal distribution, bone density values in individualsare often expressed in relation to a reference populationin standard deviation units. This reduces the problemsassociated with differences in calibration between someinstruments. When standard deviation units are used inrelation to the young healthy population, this is referredto as the T-score.
For diagnostic purposes two thresholds of bone
mineral density have been proposed for Caucasianwomen based on the T-score [2]. The first defines themajority of individuals who will sustain a fracture in thefuture (osteoporosis) and the second a higher thresholdthat may identify those most likely to developosteoporosis and those women who might benefit mostby the prevention of bone loss at the time of themenopause (low bone mass or osteopenia). Osteoporosisdenotes a value for bone mineral density or bone mineralcontent that is two and a half standard deviations or morebelow the young adult mean value (T-score 4–2.5).
Osteopenia or low bone mass is a T-score that liesbetween –1 and –2.5.
Severe or ‘established' osteoporosis denotes osteo-
porosis as defined above in the presence of one or moredocumented fragility fractures, usually of the wrist, spineor hip.
In the young healthy population, 15% of women will
Fig. 2. Dual-energy X-ray absorptiometry scan of the lumbar spine in
have a T-score of less than –1, and thus have osteopenia.
a healthy, premenopausal woman aged 33 years. The computer hasselected the edge of the spine and the vertebrae have been
Approximately half a per cent will already have
distinguished by the operator to give the areas of interest to be
osteoporosis (Fig. 3). Note that these thresholds apply
to women only.
Suitable diagnostic cut-off values for men are less
secure. It has been suggested that a similar absolute
Table 2. Measurements made from an anteroposterior scan using
DXA at the lumbar spine in a 53-year-old woman at the menopause
value for bone mineral density as that used in womencan be taken as a cut-off point for the diagnosis of
Note the increase in vertebral area, mineral content and density withthe more caudal direction. The results are compared either with thepremenopausal reference range (T-score) or with an age-matchedpopulation (Z-score). In this instance the bone mineral density is 6%below the average for peak bone density but 5% above average forage.
aStandard deviation units.
Bone Mineral and Osteoporosis
Skeletal mass is relatively constant once growth has
Fig. 3. Distribution of bone mineral density in young healthy women
aged 30–40 years. Because the distribution of bone density is normal,
ceased, until the age of 50 years or so. The distribution
15% of the population have a T-score of –1 or lower and less than
of bone mineral content or density in young healthy
0.6% of the population have a T-score below –2.5.
Guidelines for Diagnosis and Management of Osteoporosis
osteoporosis; namely a value for bone mineral 2.5
proportion of patients with osteoporosis increases
standard deviations below the average for women.
exponentially with age because of the distribution ofbone mineral density in the population (Fig. 4). Boneloss occurs with age in men, but the rate of bone loss is
Natural History of Bone Loss
much slower so that the frequency of osteoporosis and offractures is less.
Bone mineral content and density are relatively constantin adult men and women under the age of 50 years. In
What Does This Tell us About Fracture Risk? The
women, loss of bone may occur before the age of
average life-time risk of the common osteoporotic
menopause at some sites, but losses are small compared
fractures in white women and men is approximately
with those in later life. Enhanced bone loss occurs
40% and 13% respectively at the age of 50 years (see
thereafter, and coincides with ovarian failure shortly
Table 1). The risk of fracture approximately doubles for
before the menopause and continues throughout life. The
each standard deviation decrease in bone mineraldensity. The risk is more than doubled in individualswith low bone mass and nearly 4-fold greater in womenwith osteoporosis (50% life-time risk at the age of 50years) compared with women with a normal bonemineral density (13% life-time risk at 50 years). Therisks can be doubled again when individuals have had afragility fracture beforehand (see below).
Estimating fracture risk by bone mineral measure-
ments is comparable to the assessment of the risk ofstroke by blood pressure readings. Blood pressure valuesare continuously distributed in the population, as is bonemineral density. In the same way that a patient above acut-off level for blood pressure is diagnosed ashypertensive, the diagnosis of osteoporosis is based ona value for bone mineral below a cut-off threshold. As isthe case for blood pressure and stroke, there is noabsolute threshold for bone mineral that discriminatesabsolutely who will or will not fracture. The perfor-mance of bone mineral density in predicting fracture is,however, at least as good as that of blood pressure inpredicting stroke, and considerably better than the use ofserum cholesterol to predict coronary artery disease.
Nevertheless, it should be recognized that, just becausebone mineral density is normal, this is no guarantee thatfracture will not occur – only that the risk is decreased.
If, however, bone mineral density is in the osteoporoticrange, then fractures are likely.
Which Site Should be Measured? The site for assessmentdepends upon the reason for undertaking the scan andalso on the age of the patient. Osteoporosis is a systemicdisease and loss of bone occurs at all sites. For thisreason bone scans for diagnostic purposes shouldnormally be undertaken at any one site. There is only asmall advantage in the measurement of multiple sites.
Because, however, the correlation between bone mass atdifferent sites is less than perfect, osteoporosis at one siteis not invariably associated with osteoporosis at othersites, and therefore assessment of the relevant biologicalsite is preferable. For these reasons, measurements madeat the wrist, spine or hip may be appropriate in younger
Fig. 4. Bone mineral density (BMD) in women at different ages and
individuals (to assess the risk of any fracture).
the prevalence of osteoporosis. Bone mineral density is normally
In the elderly hip fractures are the major concern and
distributed at all ages, but values decrease progressively with age. The
carry the highest morbidity and mortality. If the clinician
proportion of patients with osteoporosis (with a bone mineral density
wishes to predict hip fracture risk with the greatest
of 2.5 standard deviation units or less than the young adult mean)
accuracy, then measurement at that site is more useful
increases exponentially with age. (From Kanis JA, et al. OsteoporosInt 1994;4:368–81.)
than elsewhere since measurements at the site of
J. A. Kanis et al.
biological relevance predict fractures at that site most
Table 4. Clinical risk factors providing indications for the diagnostic
accurately. In addition, osteoarthrosis is particularly
use of bone densitometry
common in the spine of men and in elderly women, and
1. Presence of strong risk factors.
in such cases this site is less suitable for the
Oestrogen deficiency
measurement of bone density in these age groups.
Premature menopause (<45 years)
Changes in bone mineral density that occur in the
Prolonged secondary amenorrhoea (>1 year)
immediate postmenopausal period or as a result of
Primary hypogonadism
treatment are often more marked in the spine and can be
Corticosteroid therapy (>7.5 mg/day for 1 year or more)Maternal family history of hip fracture
detected earlier than at the hip or wrist.
Low body mass index (<19 kg/m2)Other disorders associated with osteoporosis
Problems in the Assessment of Bone Mineral
Primary hyperparathyroidismPost-transplantationChronic renal failure
There are a number of problems and limitations in the
assessment of bone mineral which should be recognized
Prolonged immobilization
in the interpretation of bone scans (Table 3). Bone
Cushing's syndrome
mineral density gives an estimate of bone mass based on
2. Radiographic evidence of osteopenia and/or vertebral deformity
its mineral content. The presence of osteomalacia, a
3. Previous fragility fracture, particularly of the hip, spine or wrist
disorder where mineralization of bone is defective thatmay occur in the elderly, will therefore, underestimate
4. Loss of height, thoracic kyphosis
bone mass. Osteoarthrosis at both the spine and the hipare common in the elderly, and will contribute to thedensity measurement, partricularly at the spine, but not
this ‘case-finding' approach. The use of risk factors
to skeletal strength. Heterogeneity of density due to
that add information on fracture risk independently of
osteoarthrosis or previous fracture can often be detected
bone mineral density improves the specificity of
on the scan and in some cases be excluded from the
analysis. In the case of the hip, smaller regions of
There are relatively few clinical risk factors that can
interest can be selected to exclude the joint.
be applied successfully to identify affected individuals(Table 4). Significant and useful factors include a
Table 3. Problems in the interpretation of bone mineral measurements
corticosteroids and several diseases that adversely
Osteoarthritis (especially the spine)
affect bone metabolism. Very low body mass index
Vascular calcification (especially the spine)
(e.g. <19 kg/m2) and a maternal history of hip fracture
Overlying metal objects
are risk factors which are in part independent of bone
Contrast media (spine)Previous gold therapy
mineral density. So too is a history of fractures after the
Previous fracture (spine, hip and wrist)
age of 45 years, which is a strong risk factor for
subsequent fractures at the spine and elsewhere. Loss of
height may be estimated from the history or from the
Vertebral deformities due to osteoarthrosis, Scheuermann's diseaseInadequate reference ranges
difference between measured height and arm span, sincein health these measurements are usually nearly thesame. Combinations of relatively weak risk factors can
It is important that an appropriate normal reference
also be used. For example, the National Osteoporosis
range is used to interpret bone density values. The ranges
Foundation of the USA uses smoking, a parental history
supplied by manufacturers may variously over- or
of hip fracture and leanness (the lowest quartile of body
underestimate the proportion of a tested population
weight). Individuals with more than two of these risk
categorized as having osteoporosis.
factors have a greater than 30% increase in fracture riskat any age.
Measurement of bone mass is indicated in individuals
Identification of Patients with Osteoporosis
who have strong risk factors to optimize selection fortreatment (Table 4), provided that it will influence
At present there is no universally accepted policy for
management decisions for the patients. This is preferred
screening to identify patients with osteoporosis. With the
to blind treatment because not all patients with strong
increasing development of effective agents specifically
risk factors will have osteoporosis. This view does not
affecting bone metabolism this view may change. In the
preclude the usefulness of measurement of bone mineral
absence of such policies patients are identified as having
density in women without risk factors. In practice,
osteoporosis largely because of a fragility fracture or
physicians also have to manage patients without risk
sometimes by the presence of strong risk factors. Bone
factors who would take treatments if their bone mineral
mineral density measurements can be used to enhance
density were low. Although the use of bone density in
Guidelines for Diagnosis and Management of Osteoporosis
Table 5. Diagnostic categories based on bone mineral density and
individuals, but life expectancy is short. Up to the age of
recommendations within each category
75 years the cut-off point of bone mineral density todiagnose osteoporosis is an appropriate treatment
Diagnostic category
threshold for several treatments. Hip fracture is a
major problem in the elderly, but after the age of 75years the life-time risk of fracture for a given bone
mineral measurement decreases (Fig. 5).
Consider prevention inperimenopausal women or
In men and women over the age of 75 years, factors
other than bone mineral density measurements may
Consider treatment in more
influence the decision to treat, such as likelihood of
elderly with history of
falling, the nutritional status for vitamin D, and life
fragility fractures
Exclude contributing causes,particularly if youngIntervention recommendedparticularly if less than
Investigation of Patients with Osteoporosis
Established osteoporosis
Very high Exclude contributing causes
Intervention strongly indicated
The same diagnostic approach should be undertaken inpatients with osteoporosis irrespective of the presence or
From The Sheffield Protocol for the Management of the Menopause
absence of fragility fractures. However, the range of
Under the Prevention and Treatment of Osteoporosis. 4th edition.
clinical and biological tests will depend on the severity
Osteoporosis 2000, PO Box 2000, Rotherham S61 2YU, UK.
of the disease, the age at presentation and the presence ofvertebral fractures. The aims of the clinical history,
this way is a component of good clinical practice, the
physical examination and biological tests (Table 6) are:
cost-benefit of this approach is not yet established.
. To exclude a disease that can mimic osteoporosis
Irrespective of the presence or absence of risk factors,
. To elucidate causes of osteoporosis and contributory
the assessment of bone mass is justified only in those
cases in which the result obtained will influencedecisions about treatment. In some instances, treatment
. To assess the severity of osteoporosis in order to
will be justified without measurement of bone mineral
determine the prognosis of the disease, i.e. the risk of
density, for example in patients with fragility fractures
subsequent fractures
and other strong risk factors. In other instances, the low
. To select the most appropriate form of treatment
cost and absence of side effects justify the use of some
. To perform baseline measurements for subsequent
agents without bone mineral density measurements in
monitoring of treatment
populations at lower risk (e.g. vitamin D in the elderly).
Table 6. Diagnostic procedures in osteoporosis
Decisions about the need for treatment depend not
only on establishing a diagnosis, but also on the age of
the patient, as well as the efficacy, costs and side effects
History and physical examination
of treatment. The decision to treat osteoporosis will
Blood cell count, sedimentation rate, serum calcium, albumin,
differ between a 50-year-old and an 80-year-old patient
phosphate, alkaline phosphatase, liver transaminases, serum proteinelectrophoresis, urinalysis
(Table 5). Osteoporosis in the latter is found in 50% of
Radiograph of lumbar and thoracic spinal columnBone mass measurement (DXA or SXA)Testosterone and gonadotrophins (in men)
OptionalSerum and urine markers of bone turnoverSerum PTH, 25–OHD, TSH, cancer markersGonadotrophinsUrinary free cortisolBone marrow examinationIliac crest bone biopsy after tetracycline double labelling for
histomorphometry and marrow analysis
Differential Diagnosis of Osteoporosis
Osteomalacia and malignancy commonly induce bone
Fig. 5. Life-time risk (LTR%) for osteoporotic fractures shown by age
loss and fractures. Osteomalacia is characterized by a
defect of mineralization of bone matrix most commonly
J. A. Kanis et al.
due to impaired intake, production or metabolism ofvitamin D. Other causes include impaired phosphatetransport or the chronic use of some drugs such asaluminium salts (and other phosphate-binding antacids),high doses of fluoride or etidronate, and chronic use ofantacids and anticonvulsants. In most cases the diagnosisof osteomalacia is suspected by the clinical history andby abnormalities in biochemical tests such as low valuesof serum and urinary calcium, serum phosphate and 25-hydroxyvitamin
D, and high values for alkaline
phosphatase and parathyroid hormone. A transiliacbone
necessary to demonstrate a defect in mineralizationunequivocally.
Diffuse osteoporosis with or without pathological
fracture is common in patients with multiple myeloma, a
Fig. 6. Assessment of bone mineral density in a 70-year-old woman
using the T-score and Z-score. The patient's value depicted by the
condition suspected by the severity of bone pain,
filled square lies 1.2 standard deviations below the average expected
increased sedimentation rate and Bence Jones proteinur-
for her age (Z-score: –1.2). Bone density is lower than 3 standard
ia and identified by marrow aspirate, serum and urine
deviations below peak bone mass (T-score = –3.0), denoting the
(immuno)electrophoresis of proteins. Similarly, patho-
presence of osteoporosis.
logical fractures due to metastatic malignancies canmimic osteoporosis and can be excluded by clinical and
radiological examination, biological tests and scintigra-
Table 7. Factors contributing to osteoporosis
phy or other imaging techniques. Finally, vertebralfractures in osteoporosis should be differentiated from
Genetic or constitutional
vertebral deformities due to other disorders such as
White or Asiatic ethnicity
scoliosis, osteoarthrosis and Scheuermann's disease.
Family (maternal history of fractures)Small body frameLong hip axis lengthPremature menopause (<45 years)
Causes of Osteoporosis and Contributing Factors
Lifestyle and nutritional
A variety of disorders is associated with an increased
NulliparityProlonged secondary amenorrhoea
risk of osteoporosis (Table 7). Many are evident from the
history or physical examination. Unusual presentations
Excessive alcohol intake
of osteoporosis should alert the physician to search for
such factors. Examples include osteoporosis before the
Prolonged immobilization
age of 50 years and osteoporosis in men. A low bone
Prolonged parenteral nutritionLow body weight
mineral density for the age of the patient may be used asa guide to search for secondary causes in both men and
Medical disorders
women. Bone mineral measurements in relation to the
Malabsorption due to gastrointestinal and hepataobiliary diseases
average value expected for that age can be expressed in
age-specific standard deviation units, commonly referred
to as the Z-score (Fig. 6). Individuals with a Z-score of
Primary hypogonadism
–1 will have approximately a 2-fold higher risk of
fractures in their remaining life-time than those with an
Osteogenesis imperfecta
average value for bone mineral for their age. Those with
Rheumatoid arthritis
a Z-score of –2.5 will have a greater than 4-fold risk.
Chronic obstructive lung disease
Such cases may require additional investigation and
Chronic neurological disordersChronic renal failure
referral to a specialist. Note, however, that some
relatively common disorders such as thyrotoxicosis or
vitamin D deficiency in the elderly may not be clinically
obvious, and for this reason appropriate tests may be
required (Table 6).
Chronic corticosteroid therapyExcessive thyroid therapyAnticoagulantsChemotherapy
Assessment of Prognosis
Gonadotropin-releasing hormone agonist or antagonistAnticonvulsant
The assessment of the severity of osteoporosis is an
Chronic phosphate-binding antacid use
important step in the clinical investigation of the disease
Guidelines for Diagnosis and Management of Osteoporosis
to provide a prognosis and optimize therapeutic
the known risk factors. Their identification is important,
strategies. Four compontents can be identified:
however, for evaluating the prognosis of osteoporosis
and in some cases for its management.
Quantification of bone mass
There are several different categories of risk factors.
. Identification of previous fractures (axial and appen-
They may be related to the determinants of bone mineral
density, capture the risk of falls, be related to skeletal
. Identification of factors that influence the risk of
fragility independently of bone mineral density or a
fractures independently of bone mass
combination of these. A risk factor for fragility fractures
. Assessment of the rate of loss of bone
independent of bone mineral is the length of the head ofthe femur (hip-axis length). In women, the longer thelength the higher the risk of hip fracture. Clinical and
Quantification of Bone Mineral. The lower the bone
environmental factors associated with an increased risk
mass, the higher the risk of fracture. With DXA or SXA,
of fracture are best documented in the elderly to assess
the risk approximately doubles for each unit decrease in
the risk of hip fracture. Excessive frailty, immobiliza-
T-score. For example, a woman with a T-score of –3.5
tion, concurrent diseases or drugs which increase the
has a 2-fold higher risk of fracture than a woman with a
liability to falls are examples. Environmental factors
T-score of –2.5, DXA and SXA are the preferred
such as slippery surfaces and inadequate lighting
techniques, but if they are not available, any estimate
increase the risk of fractures independently of bone
using a validated technique is better than none. Bone
mass by causing falls or modifying the impact of the fall.
mass can be measured at the spine, hip, forearm or heel,
Risk factors unrelated to bone mass have little impact in
because osteoporosis is a systemic disease occurring
the assessment of fracture risk in early postmenopausal
throughout the skeleton. As mentioned, site-specific
women, but in the elderly their presence appears to at
least double the risk of hip fracture.
fracture risk is best assessed at the hip.
After the age of 65 years, the lumbar spine may not be
Rates of Bone Loss. The loss of bone with age in women
the site of choice because of the errors of accuracy
and probably in men varies from patient to patient but
associated with osteoarthritis, osteoarthrosis or lumbar
continues throughout life. Where rates of bone loss are
fractures. In the majority of cases, measurement at one
high the risk of fractures is higher than where rates of
site is sufficient, although in some cases measurement at
loss are low. Direct measurement of the rate of bone loss
two sites may be justified.
in an osteoporotic patient would require at least two
The absolute risk of fracture depends not only upon
measurements of bone mass over a 2–4 year interval,
bone mineral density but also on life expectancy. Thus,
given the precision errors of the technique and the
for a given value of bone mineral density the remaining
magnitude of change in bone mass that is expected. Such
life-time risk in the absence of treatment for patients
a strategy is not practical where it is necessary to decide
aged 50 years is high compared with the same bone
whether or not to treat at the time of initial assessment.
mineral density value in a patient of the same sex at 80
Because the rate of bone loss is proportional to the rate
years. The conversion of relative risk to absolute risk is
of bone turnover in postmenopausal women, it has been
helpful information for the patient and physician and
suggested that the rate of loss can be predicted by
aids in management decisions.
assessing bone turnover with serum and/or urinarymarkers that are specific for bone formation and
Previous Fractures. Patients who have suffered one or
resorption. Serum osteocalcin and alkaline phosphatase,
more fragility fracture at any site are at increased risk of
in particular the bone-derived fraction, are validated
having subsequent fracture for any given value of bone
indices of bone formation. Urinary hydroxyproline and
mineral. The earlier the age at fracture and the greater
fasting urinary calcium/creatinine ratios are widely used
the number of previous fractures, the greater the
as indices of resorption. However, the pyridinoline
subsequent risk. The risk of vertebral fractures is
crosslinks and related peptides are more sensitive and
particularly high in those with prevalent vertebral
specific markers of bone resorption. The predictive value
fractures and is increased at least 2-fold. A wrist fracture
of future bone loss is improved by using a marker of
doubles the risk of hip fracture and triples the risk of
formation and a marker of resorption rather than one
vertebral fracture. Thus, previous fractures should be
marker alone. Although rates of loss assessed in this way
documented. A lateral radiograph of the thoracic and
are less accurate than rates of loss assessed over many
lumbar spine is necessary to detect prevalent vertebral
years by sequential bone mineral density measurements,
a high rate of bone resorption (i.e. above the referencerange for premenopausal women) is associated with a 2-
Additional Risk Factors. Although several clinical risk
fold increase in the risk of vertebral and hip fracture
factors are significantly associated with a low bone mass,
independently of the prevailing bone mineral density.
their identification cannot be used in individuals as a
Measurement of a bone marker at the time of the
surrogate for bone mass measurement. For example, in
initial investigation of osteoporosis also provides useful
women 10 years after the menopause only 15–30% of
baseline parameters for monitoring treatment using
the total variance of bone mass can be accounted for by
inhibitors of bone turnover (discussed below).
J. A. Kanis et al.
Non-drug Treatment of Osteoporosis
Table 8. Calcium content of some foods
Treatment of osteoporosis not only comprises the
modification of bone mass, but in addition involves:
. Maintenance or improvement of mobility
Milk, semi-skimmed
Nutritional advice
. Treatment of associated disorders and risk factors
Treatment of associated morbidity
Maintenance of Mobility
Canned sardines in oil
Canned pilchards in oil
Regular exercise is important for general health. Non-
weight-bearing activities provided by physiotherapy,
swimming or gymnastics variously improve well-being
and increase confidence and coordination and may
decrease the risk of falls. With respect to skeletal
health, weight-bearing activity such as walking isbeneficial. The necessary intensity and frequency ofsuch exercise is unknown.
common foods is given in Table 8. Some mineral waters
What is clear is that immobilization, even for a short
are also rich in calcium. Where dietary manipulation is
period, is deleterious. The gains from vigorous exercise
not feasible, calcium may be given in the form of
compared with everyday activities are probably small,
supplements (see later). Higher intakes of calcium may
and must be maintained to preserve any effect. Very
be required where other treatments are given.
vigorous exercise can give rise to gonadal insufficiencyand aggravate osteoporosis. Planned exercise regimensare, however, important for the rehabilitation of
Treatment of Associated Disorders and Risk Factors
individuals with established osteoporosis.
Treatment of diseases associated with osteoporosis (seeTable 7) is unlikely to reverse osteoporosis except in
children, but may prevent the progression of thedisorder. Examples include thyrotoxicosis, prolactinoma
Vitamin D deficiency impairs the mineralization of bone
and hypercortisolism. Thyroid replacement treatment
and may also accelerate osteoporosis. The recommended
should be carefully monitored and corticosteroids given
dietary allowance for vitamin D is 400 IU daily
in the lowest possible doses.
(approximately 10 mg) and, where necessary, the diet
Many modifications to lifestyle which stand to
may be modified or supplements given. The require-
improve general health may also reduce the risk of
ments for vitamin D in the elderly are not well
fracture in patients with osteoporosis. Excessive use of
established and may be as high as 800 IU daily. Intakes
alcohol should be avoided. Smoking is probably a minor
above this have no added benefits and expose patients to
risk factor, but there are many other reasons to advise
potential toxicity such as hypercalcaemia. The risks of
patients to stop smoking. The risk of falls may be
vitamin D deficiency are particularly high in institutio-
reduced by treating underlying causes and revision of
nalized individuals not exposed to sunlight.
concomitant drug treatment. Where possible, long-acting
Normal protein intake is important in the elderly, and
hypnotics and psychotropic drugs and overtreatment
attention to dietary deficiencies at the time of hip
with agents for hypertension should be avoided, since
fracture decreases the morbidity and mortality.
these may increase the risk of falls. The provision of soft
The intake of calcium that best advantages the
floor coverings or the wearing of hip protectors decrease
skeleton is controversial. The controversy surrounds
the impact of falls and the risk of fractures. Such
the requirements for peak skeletal mass rather than in
measures are particularly useful in patients in institu-
later life. In the young, the recommended dietary
tional or sheltered accommodation. These approaches
allowance (RDA) for calcium varies between countries.
should not be seen as substitutes for medical interven-
In the United Kingdom, for example, the RDA is 400–
tion, but as adjuncts to treatment.
500 mg daily, whereas in the United States it is 800 mg.
In contrast there is little disagreement that an adequate
intake of calcium attenuates, though does not reverse,
Treatment of Associated Morbidity
bone losses in individuals with osteoporosis. It isimportant, therefore, that all patients with osteoporosis
Early mobilization after fractures is a priority. In the
are encouraged to take the RDA of calcium irrespective
case of hip fracture, internal fixation or hemiarthroplasty
of other treatments. The calcium composition of some
is preferred to conservative management to avoid the
Guidelines for Diagnosis and Management of Osteoporosis
consequences of immobilization, particularly bone loss
Because of the differences in the availability of
which is not subsequently regained. In the elderly,
specific agents directed at bone metabolism in different
attention to post-operative nutrition, and particularly
countries, approaches to treatment will vary. Never-
protein intake, decreases morbidity and mortality.
theless, there are several general approaches that are
Treatment of acute and chronic back pain related to
vertebral fractures depends on general measures and noton anti-osteoporotic drugs. Acute pain due to a recentvertebral fracture responds to bed rest, analgesics, heatand gentle massage or transcutaneous electrical nerve
1. Inhibitors of Bone Turnover
stimulation (TENS) of paraspinal muscles to alleviatespasm. Total bed rest should not exceed a few days as
The majority of agents used in osteoporosis inhibit bone
prolonged immobilization may aggravate bone loss. The
resorption and thereby the turnover of bone. In
temporary use of a back support is often useful to help
osteoporosis their administration causes a small incre-
the patient to resume daily activities as soon as possible.
ment in bone mass (5–10% at the lumbar spine and less
The long-term management of pain due to vertebral
at other sites) over a period of up to 3 years. Thereafter,
fractures include the use of analgesics, physiotherapy,
bone mass is variously stabilized, decreases slowly or
TENS and intermittent use of spinal supports for some
increases slowly depending on the agent and dose
activities. A supervised exercise programme to maintain
selected. The increase in skeletal mass during the early
strength and flexibility of the thoracic and lumbar spine
years of treatment is not sufficient to restore skeletal
is desirable. The lifting of heavy weights should be
mass to normal in the osteoporotic patient. The
oestrogens and bisphosphonates in sufficient dosesprevent bone loss. Less complete effects may be seenwith other agents.
Drug Treatment of Osteoporosis
The gains in bone mass or inhibition or attenuation of
bone loss are associated with a decrease in the risk of
A number of agents which favourably affect skeletal
fractures. Observational and randomized controlled trials
metabolism are available in different countries (Table 9).
indicate the gonadal hormones, bisphosphonates, calci-
Several of these agents are utilized both in treatment and
tonins and calcium decrease fracture risk, but the level of
in prevention. The scope of these guidelines is very
evidence for anti-fracture efficacy varies markedly
much directed to the treatment of osteoporosis, but
similar considerations apply to its prevention.
Table 10. Information on the anti-fracture effects of different
therapeutic agents commonly used in osteoporosis from randomized
Table 9. Some agents available for use in the treatment of
clinical trials (RCT) and observational studies.
RCT evidence RCT evidence Observational
Inhibitors of bone turnover
Oestrogens with and without progestogens
Oestrogen derivatives and receptor agonists
Calcitonins (salmon, eel, human, porcine)
Pamidronate and others
Vitamin D derivatives ±
Anabolic steroids
Stimulators of bone formation
++, consistent effects in several studies; +, consistent effects in a few
Parathyroid hormone and other peptides
studies; 0, not studied; ±, variable effects reported; –, negative effects
Anabolic steroids
Hormone Replacement Therapy
Vitamin D and derivatives
Calciferol and cholecalciferol (vitamins D2 and D3)Calcitriol
In women with post menopausal osteoporosis, hormone
replacement therapy (HRT) should be considered early
in a management programme. HRT prevents further lossof bone at all skeletal sites, irrespective of the age of the
J. A. Kanis et al.
individual, and the effects persist for the duration of
Table 11. Potential, relative and absolute contraindications for
hormone replacement therapy
The decision to utilize HRT will depend upon a
number of factors, including:
Active endometrial or breast cancer
. Evidence of hypogonadal status
PregnancyUndiagnosed abnormal vaginal bleeding
. The absence of absolute contraindications to treatment
Severe active liver disease
. The risks and benefits of HRT for the individual
Acute deep venous thrombosis and thromboembolic disease
Recent hormone-dependent cancers
The risks and benefits perceived by the patient
Relative contraindications (specialist opinion may be sought)
The acceptability of long-term HRT to the patient
. Adequate treatment of any associated disorder,
Previous spontaneous deep venous thrombosis or pulmonary
particularly vitamin D deficiency
Systemic lupus erythemotosus
The assessment of hypogonadal status is not usually
Endometriosis (unopposed oestrogens)
problematic. The presence of postmenopausal symptoms
FibroidsPrevious breast cancer or strong family history
is presumptive evidence of hypogonadal status in
Endometrial cancer (within 5 years)
hysterectomized women. In some patients biochemical
evaluation of gonadal status by the measurement of
follicle stimulating hormone (FSH) is required.
Menopausal symptoms are a common reason why
Pre-existing gall stones
patients elect to take HRT. It should be explained,
Mild liver disease
however, that the duration of treatment required to
control menopausal symptoms is relatively short (1–2
Parenteral route preferred.
years) compared with the duration of treatment that isappropriate for osteoporosis (5–10 years or even longer).
risks and benefits perceived by the patient. Despite an
The risks and benefits of HRT should be explained to
explanation of the risks and benefits, some women will
patients. The side effects of HRT include menstrual or
prefer to avoid HRT and alternative options should be
breakthrough bleeding in non-hysterectomized women,
breast tenderness, a bloated feeling and changes in
There are few absolute contraindications to oestrogen
weight. A number of apparent contraindications given in
therapy (Table 11). Age is often cited as a contra-
product information brochures in many countries are
indication, but the risks and benefits do not change with
misleading since they are derived from the pharmaco-
age. There are, however, several disorders where a
logical effects observed with high doses of synthetic
careful assessment is appropriate and in some instances
is an appropriate reason for referral (see Table 11).
cardiovascular disease is often cited as a relative
Adequate treatment of any associated disorders should
contraindication, but current evidence suggests that the
in some cases precede or be given concurrently with
converse is true. Indeed, the presence or risk of
HRT. In the elderly it is particularly important to
cardiovascular disease is a major reason why HRT is
exclude vitamin D deficiency. For many disorders the
preferred. Patients should also be counselled on the
postmenopausal status will aggravate osteoporosis. Note
potential adverse effects of HRT, including the risk of
that HRT may be used with other treatment modalities,
breast cancer and venous thromboembolism. An in-
under specialist supervision. Examples include the use of
creased risk of breast cancer is biologically plausible. It
parathyroid hormone (PTH) and fluoride.
is known that endogenous hormonal factors play a part inthe aetiology of the disease throughout life (e.g. age at
Types of Oestrogen Therapy. Hysterectomized women
menarche, breast feeding and age at menopause). A
can be given oestrogen preparations alone. Women with
small increase in relative risk has been found by some,
a uterus should be given both an oestrogen and a
but not all studies with long-term use of HRT. If the risk
progestogen intermittently or continously, which pre-
is increased then the increase is small, and lower than the
vents the occurrence of endometrial hyperplasia and any
risks of breast cancer associated with obesity, regular
risk of endometrial carcinoma. In most countries, so-
alcohol intake or a family history of breast cancer. It
called natural oestrogens such as 17b-oestradiol are
should be explained that the reported increase in some
preferred to synthetic oestrogens. Doses which prevent
studies has not usually been associated with an increase
bone loss (on average) of various preparations are shown
in mortality and that the use of HRT implies regular
in Table 12. In the elderly it is prudent to start with small
surveillance. Women electing to take HRT should have
doses and prescribe a bone-sparing dose after several
Except in hysterectomized women and with some
In many countries, combined continuous oestrogen
HRT modalities (such as continuous combined regi-
and progestogen regimes are available. They are
mens), menstrual bleeding is an inevitable consequence.
particularly suitable for postmenopausal rather than
Whereas most analyses indicate that benefits outweigh
perimenopausal women in whom withdrawal bleeds
the risks of HRT, counselling should also elucidate the
are not tolerated. These regimens generally do not
Guidelines for Diagnosis and Management of Osteoporosis
Table 12. Bone-sparing doses of commonly used preparations
dose of 2.5 mg daily and there is usually no withdrawalbleed. The long-term effects of tibolone on cardiovas-
Bone-sparing dose (mg)
cular morbidity have not been evaluated, but it decreasesboth high density and low density lipoproteins (HDL and
Oestradiol valerate
Piperazine oestrone sulphate
Conjugated equine oestrogens
Oestradiol implants (6-monthly)
Transdermal oestradiol
women. Tamoxifen may accelerate skeletal losses
Ethinyl oestradiol
before the menopause and its prolonged use may
Oestrone sulphate
increase the risk of endometrial cancers. Tamoxifen is
Other agents
used in specialist centres, particularly in women with a
history or family history of breast cancer. New
modulators are currently being developed that may
have agonist activity on the skeleton and cardiovascular
system but not on the breast and endometrium.
Calcium. Calcium is widely available throughout theworld and is the major non-HRT intervention used in
aGiven for 12–14 days out of 28 days with continuous oestrogen.
osteoporosis. Its principal effect is to decrease the rate of
Commonly used in the United States.
bone loss rather than to prevent this loss entirely. It isless effective than many other treatments and is usually
induce cyclical bleeding and suppress endometrial
given as an adjunct to other treatments.
proliferation. In about a quarter of women, irregular
The doses of calcium required to attenuate bone loss
bleeding may occur, particularly in the first 6 months
are pharmacological, and the diet should be supplemen-
after the onset of treatment. This can be minimized by
ted with an additional 1000–1500 mg daily. It is
increasing the doses of progestogen where oestrogen and
appropriate to offer calcium either as a supplement or
progestogen are being used separately.
by dietary manipulation in all patients with osteoporosis
Oestrogens and progestogens are usually given by
in whom other treatment modalities are not prescribed.
mouth. Transdermal and subcutaneous delivery systems
The major advantage of calcium is that it is easy to use,
bypass the liver as do other parenteral routes. These
requires little monitoring, and is acceptable to patients.
routes may be advantageous in patients with mild liver
Compliance with treatment is high.
disease, previous thromboembolism or gall stones. Some
A wide variety of calcium preparations is available in
most countries. Many non-proprietary formulations are
also available, but in many countries their calcium
Implants of oestradiol are given as a pellet implanted
content is small, so that more than 10 tablets need to be
into subcutaneous fatty layers. They are most frequently
taken daily in order to provide a dose of 1000 mg. It is
used at the time of surgery in women undergoing
important to recognize that the elemental content of
oophorectomy or hysterectomy, but women with a uterus
calcium varies with the product. For example, calcium
should also take progestogens.
carbonate contains 40% of elemental calcium by weight
Topical oestrogen vaginal creams, pessaries and
whereas calcium gluconate contains only 9%.
tablets have a potent local action and effectively relieve
There are small differences in the bioavailability of
vaginal dryness and atrophic vaginitis. They relieve
calcium between proprietary preparations, but these are
urinary symptoms less consistently. They do not deliver
unlikely to be of therapeutic significance. Acute
adequate amounts to treat osteoporosis, but the rate ofabsorption of oestrogens from the vagina varies
availability is greater with meals but is again of little
considerably so that cyclical progestogens may be
therapeutic significance. It may be more important to
divide the daily dose so that each dose does not exceed500 mg, since the additional gains from larger does aretrivial.
Oestrogen Derivatives and Receptor Agonists
The risks of supplemental calcium are negligible, but
it is contraindicated in patients known to have increased
Tibolone. Tibolone is a synthetic analogue of the
intestinal absorption of calcium (e.g. due to hypercal-
gonadal steroids with combined oestrogenic, progesto-
ciuria nephrolithiasis or sarcoidosis) or hypercalcaemia.
genic and mild androgenic properties. It preventsoestrogen deficiency bone loss, is effective in controlling
Calcitonins. Calcitonin in pharmacological amounts is
hot flushes and sweats, and can also improve mood and
an inhibitor of bone resorption, and this is a major reason
libido. Its effects on fracture frequency have not been
for its use in osteoporosis. It is given either as a nasal
reported. It does not cause endometrial proliferation at a
spray or as a parenteral injection.
J. A. Kanis et al.
In addition to preventing bone loss it also has analgesic
5–10% over 2 years and thereafter is stabilized.
effects and it is an attractive option for the acute
Vertebral fracture risk is decreased. The effects on hip
management of vertebral fracture, particularly where
fracture are not known.
bed rest or other forms of immobilization are required.
Alendronate is given in a dose of 10 mg daily on a
The effects of calcitonins on bone mass and fracture after
continuous basis. Side effects are uncommon, but include
many years of administration are not yet known. Short-
upper intestinal and oesophageal irritation. Large
term studies suggest a reduction in fracture rate and
randomized controlled trials have clearly demonstrated
fracture prevention studies are currently in progress.
a beneficial effect of oral alendronate on bone mineral
Several different calcitonins are available for the
density and the incidence of fractures among women with
postmenopausal vertebral osteoporosis. In one such study
calcitonin, salmon calcitonin (salcatonin), human calci-
of women with low bone density in the lumbar spine or
tonin and an analogue of eel calcitonin. Doses used vary
femoral neck, who were treated with alendronate and
from 50 to 100 International Units (IU) daily by
calcium, patients showed progressive increases in bone
parenteral injection. A commonly used regimen is 100
mineral density in the axial and appendicular skeleton
IU three times per week. Higher doses (200 IU daily or
over a 3-year period, as compared with a calcium-treated
more) are required when salmon calcitonin is given by
control group who lost bone. Mean differences in bone
the nasal route.
mineral density between the treated and control groups
There are no absolute contraindications to calcitonin
after 3 years were 8.8% in the spine, 5.9% in the femoral
with the exception of allergy, which is extremely rare.
neck and 2.5% in the total body. In this study treatment
When given parenterally all the calcitonins induce
was associated with a 48% reduction in the proportion of
side effects which are inconvenient rather than serious.
women with new vertebral fractures, a decreased
Their frequency and severity are dose-dependent. The
progression of vertebral deformities, and a significant
most frequent effect is nausea, which occurs shortly after
reduction in height loss. In a second study, 6000 women
injection in up to 30% of patients. It may be transient or
aged 55–80 years, selected from the general population,
persist for several hours. Occasionally it may persist
underwent thoracolumbar radiography. The 2000 women
until the next injection and 5–10% of patients cannot
with vertebral deformities were randomized to receiving
tolerate long-term treatment for this reason. Nausea can
alendronate/calcium or calcium alone. The alendronate-
be managed to some degree by the concurrent
treated arm revealed a 57% reduction in painful spinal
administration of anti-emetics. Both may be given at
fractures, a 44% reduction in wrist fractures and a 50%
reduction in hip fractures. All these differences were
Other symptoms including flushing, vomiting, diar-
rhoea and local pain at the site of injection. Systemic
Much less data is available for clodronate and
side effects are rarely, if ever, encountered with the use
pamidronate. Clodronate is usually given as a daily
of nasal calcitonin, but local nasal irritation occurs in
dose of 800 mg but intermittent intravenous cyclical oral
some patients.
regimens such as every other month are given in somecountries. The most frequently used oral dose of
Bisphosphonates. Several bisphosphonates are available
pamidronate is 150 mg daily. It may cause upper-
in different countries for the management of osteoporo-
intestinal intolerance and for this reason is not widely
sis. At present etidronate and alendronate are the most
utilized. Both these bisphosphonates induce progressive
commonly used bisphosphonates, but clodronate and
increments in spinal bone mineral density.
pamidronate are available for use in several countries.
The bisphosphonates are poorly absorbed from the
gastrointestinal tract. Absorption is between 1% and 5%
2. Stimulators of Bone Formation
of the administered dose, but is reduced to nearly zero inthe presence of food or liquids containing calcium or
Several agents are capable of inducing marked increases
other divalent cation which chelate the bisphosphonate.
in skeletal mass in osteoporotic patients and indeed
Thus, the bisphosphanates when given orally need to be
skeletal mass may be restored to normal. Agents include
taken away from food or calcium-containing liquids. A
parathyroid hormone and its analogues, combination and
proportion of the dose is bound to calcium in the
sequential regimens using several interventions, and
skeleton and the remainder excreted unchanged in the
fluoride. With the exception of fluoride in some
urine. At skeletal sites they inhibit bone resorption in a
countries, they are used in specialist centres.
Etidronate is usually given in a dose of 400 mg daily
for 2 weeks of a 13-week cycle. Usually, calcium is
Fluoride Salts
given continuously in the 11 weeks that the patient is nottaking etidronate. It is important that etidronate is not
Fluoride salts are available in many countries but not
given continuously since this may impair the miner-
consistently, and where unavailable are utilized by
alization of bone. Side effects are few and usually related
specialist centres. Preparations of fluoride include
sodium fluoride as a tablet and enteric coated or
expected, bone mass increases at the lumbar spine by
sustained release preparations. Disodium monofluoro-
Guidelines for Diagnosis and Management of Osteoporosis
phosphate is available in several European countries. A
have been less well characterized than the inhibitors of
dose of 100 mg is equivalent to 16.4 mg of fluoride ion
bone turnover or stimulators of bone formation.
or 36 mg of sodium fluoride. Fluoride is one of the fewagents
cancellous bone mass on a long-term basis, but its
Anabolic Steroids
effects on vertebral fracture are inconsistent. It must begiven with calcium to prevent secondary hyperparathy-
Anabolic steorids can be broadly divided according to
roidism and cortical bone porosity which may increase
structural additions at the carbon 17 position. 17a-
the risk of hip fracture. With the exception of calcium
alkylated agents include stanozolol and oxymetholone.
monofluorophosphate and some soluble calcium salts,
17b-esterified derivatives include testosterone and
calcium should be given away from fluoride since it
nandrolone. The side effect profile is determined, in
impairs its bioavailability. Appropriate doses of bio-
part, by these different conformations.
available fluoride ion are 10–15 mg daily.
The anabolic steroids most commonly used in
Side effects of fluoride therapy are common, but
osteoporosis are stanozolol and nandrolone, but they
mainly reversible when treatment is stopped. They
are not universally approved for use; in countries where
include gastrointestinal irritation (nausea, vomiting,
their use is restricted they are commonly given in
pain, diarrhoea and occasionally gastrointestinal bleed-
specialist centres. Stanozolol is given by mouth 5 mg
ing) and osteoarticular pain. Side effects are dose
daily. The most common route for nandrolone is by
dependent. Gastrointestinal side effects appear to be
intramuscular injection of nandrolone decanoate (50 mg
most troublesome with solutions, and are improved by
i.m. every 2–4 weeks).
tablet formulations and when taken with food. Fewer
The anabolic steroids prevent bone loss, probably by a
gastrointestinal side effects are noted with sustained
preferential effect on endocortical bone. In addition to
release or enteric coated preparations.
their effects on skeletal metabolism, they have marked
Osteoarticular pain is also dose dependent and
anabolic effects on muscle mass and are commonly used
commonly resolves after stopping treatment over 4–8
in the frail elderly population. They are also one of the
weeks. It may be associated with the presence of
few anti-osteoporotic agents which make patients feel
microfractures visible on bone scans. These fractures
better. A major difficulty with their use is side effects.
occur most commonly in patients with lower bone
Agents given by mouth such as stanozolol increase
mineral density. Treatment may be resumed at a lower
hepatic transaminases in approximately 50% of patients.
dose when bone pain has ceased.
These changes are reversible when treatment is stopped.
A major problem in the management of osteoporosis
Treatment is commonly continued unless liver enzyme
with fluoride is that the response to treatment is
activity exceeds 2 times the upper limit of the reference
heterogeneous and up to 40% of patients show little or
range. Another effect of stanozolol is the induction of an
no anabolic effect of sodium fluoride. There is currently
atherogenic lipid profile. This potential effect on
no reliable way of assessing before treatment who will
cardiovascular risk has to be weighed against the
respond poorly or favourably. Effects on bone mass can
potentially beneficial effects on coagulation, fibrinolysis
be assessed either quantitatively by the assessment of
and the skeleton. For this reason stanozolol and
bone mineral density or qualitatively by radiographic
oxandrolone may be more suitable for use in the elderly.
assessment of the spine.
Hoarseness and virilization are rare with the use of
Fluoride should not be used in patients with renal
stanozolol, but are major side effects of nandrolone. The
failure, nor in patients in whom osteomalacia is
most common side effect is hoarseness, and its
suspected. The latter are likely to respond adversely to
frequency is dose dependent. It is less frequent when
fluoride unless vitamin D is also given. Indeed,
nandrolone is given 4-weekly rather than 2-weekly.
physiological doses of vitamin D should be given
Both agents may induce mild increases in sodium
where the nutritional status of the patient is in doubt,
retention. This is rarely a reason for stopping treatment,
but pharmacological doses of vitamin D offer no
but diuretics may be required. Many patients report an
advantages over the use of fluoride and calcium alone.
improvement in general well-being. In a few, an increase
It is unclear for how long treatment should be given,
in libido is reported as an unwanted effect. Requirements
but it should not be continued indefinitely. A common
for anti-coagulants and oral hypoglycaemic agents may
strategy is to treat for 2–3 years. In specialist centres
decrease because of their effect on coagulation and
longer treatments are sometimes given to restore skeletal
glucose tolerance.
mass at cancellous skeletal sites to within the normalrange, which in most patients can be achieved within 5years.
Vitamin D and Derivatives
Calcitriol and Alfacalcidol. Alfacalcidol is a synthetic
3. Other Agents with Heterogeneous Effects
analogue of the vitamin D metabolite calcitriol (1,25-dihydroxyvitamin D3) and it is metabolized to calcitriol
Several other agents are available in different countries
by 25-hydroxylation in the liver. It is somewhat less
for the treatment of osteoporosis (see Table 9). They
potent than calcitriol. Both agents are used in some
J. A. Kanis et al.
countries for the treatment of osteoporosis. Several but
it is extensively metabolized, so that no accumulation
not all studies show decreases in vertebral fracture risk.
occurs in any body tissue. The most frequent side effects
The effects on bone mineral density have been less
No fracture data are available yet, but fracture
The major problem with the use of the vitamin D
prevention studies are currently in progress.
derivatives is hypercalcaemia and hypercalciuria. Ad-verse effects of prolonged hypercalcaemia include
Thiazide Diuretics. Thiazide diuretics are not licensed for
impairment of renal function and nephrocalcinosis. The
use in osteoporosis, but one of their actions is to increase
narrow therapeutic window demands that frequent
renal tubular reabsorption of calcium and decrease bone
surveillance of serum and possibly urine calcium
turnover, thereby decreasing skeletal losses. Where
should be undertaken in patients exposed to these
diuretics are required there is clearly an advantage to
agents. Calcium supplementation of the diet should be
the use of thiazide diuretics, where appropriate.
avoided or used with care.
Vitamin D. Low values for calcidiol (25-hydroxyvitamin
Monitoring of Treatment
D) are commonly found in the elderly, particularly thoseconfined to institutional care in whom the risk of hip and
General Measures
other fractures is much higher than in the generalcommunity. For this reason vitamin D may be used
Physical examination should be repeated at intervals that
routinely in institutionalized patients. In the elderly,
will depend on the severity of the disease, and should
privational deficiency is not always associated with
include the assessment of weight, height (especially if
florid osteomalacia, but a more common finding is
vertebral fractures are present), clinical risk factors,
secondary hyperparathyroidism. A parathyroid hormone
recent drug intervention and peripheral fractures. In case
value above normal using an intact assay or a calcidiol
of episodes of acute back pain and/or of a significant loss
value of <20 nmol/l are appropriate intervention thresh-
of height (> 1 cm), lateral radiographs of the thoracic
olds and treatment decreases fracture risk. Vitamin D2 or
and lumbar spine should be performed. Detecting new
vitamin D3 can be given alone or with calcium and other
vertebral fractures requires a careful comparison of the
supplements where other nutritional deficits are sus-
previous and recent radiographs with adequate quality
pected. In some countries combined formulations of
control, particularly centering of films.
calcium and vitamin D are available and are useful in theelderly where multiple tablet types increase the risk ofnon-compliance or toxicity. It is important, however, to
Repeated Bone Mass Measurement
check that the dose of vitamin D and calcium isappropriate.
The goal of drug therapy in a patient with osteoporosis is
Appropriate amounts of vitamin D are 400–800 IU
to prevent further bone loss in order to decrease fracture
daily. In patients who are unlikely to be compliant,
risk. After 2 years of antiresorptive therapy there is
intermittent intramuscular injection may be used. Annual
usually a small increase in bone mass in the order of 5–
injections of 150 000 or 300 000 units can be given in
10% at the lumbar spine and less than 5% at the femoral
the autumn and levels of calcidiol remain increased
neck and forearm. Gain at the spine is usually more
throughout the year.
pronounced with agents that stimulate bone formation.
The risks of appropriate doses of vitamin D are very
Fluoride induces a linear 4–8% per year increase of bone
low in the absence of sarcoidosis and idiopathic
mass at the spine and of smaller magnitude at the hip.
hypercalciuria where there is increased sensitivity to
Although these differences in response between skeletal
vitamin D. Although vitamin D status may also be
sites with both types of therapy are not fully understood,
improved by sunshine exposure and ultraviolet irradia-
they are partly explained by a greater effect of anti-
tion, radiation is less efficient in the elderly than in
osteoporotic drugs on cancellous bone – which has a
young adults. In addition, excessive sunshine exposure
high turnover – than on cortical bone – which has a
in the elderly increases the frequency of skin cancers.
lower turnover rate. Because the long-term precisionerror of the most precise techniques (DXA and SXA) isin the order of 1–2%, a change of 3–6% is required in a
single patient to assess treatment effectiveness. Thus, inmost instances, repeating bone mass measurement at an
Ipriflavone. Ipriflavone is a synthetic derivative of
interval shorter than 2 years after intitiating therapy may
naturally occurring isoflavones, and is available in
not be helpful for the physician's decision-making about
several countries for the management of osteoporosis.
treatment efficacy. It has been argued that repeating bone
It may potentiate the effects of endogenous oestrogens or
mass measurement during hormone replacement therapy
directly inhibit bone resorption.
(HRT) is not useful, because treatment is effective in up
Ipriflavone has been shown to prevent bone loss in
to 90% of patients. This does not apply to daily practice,
osteoporosis using a continuous treatment with a daily
because variable doses are used and compliance is often
oral dose of 600 mg. Its absorption is enchanced by food;
low. In a patient with osteoporosis who has already lost a
Guidelines for Diagnosis and Management of Osteoporosis
significant amount of bone, monitoring treatment
preventing hip fractures, for various agents in the
efficacy appears to be necessary, even with HRT, and
secondary prevention of vertebral fractures and for
may improve compliance.
hypothetical interventions in the elderly.
Studies of postmenopausal oestrogen replacement that
consider osteoporosis offer the following consistent
The Use of Biochemical Markers of Bone Turnover to
conclusions: (a) the cost per QALY saved when
Monitor Drug Therapy
oestrogen is used by hysterectomized women comparesfavourably with other healthcare interventions; (b) these
Antiresorptive therapy in postmenopausal osteoporosis
costs increase considerably when HRT is recommended
induces a 30–60% decrease in specific markers of bone
to all women; (c) targeting of HRT on the basis of
turnover such as serum osteocalcin, bone alkaline
fracture risk (using bone mineral density measurement)
phosphatase and urinary pyridinoline crosslinks after
is more cost-effective than treating all women; and (d)
3–6 months, followed by a plateau that is sustained as
treatment in the elderly woman (around 65 years) is
long as treatment is continued. Markers of bone
more cost-effective than treatment at the menopause. In
resorption decrease within 3 months and are followed
one such analysis, for example, it was estimated that the
by decreases in the indices of bone formation. The short-
cost per QALY of treating all postmenopausal women
term decrease in bone markers predicts the effects on
with 15 years of oestrogen was US $204 000. If women
bone mass over the subsequent 2 years, and a significant
were screened to identify the lowest 16% of the
decrease (30–60% or more depending on the marker) is a
distribution by bone mineral density at the menopause,
reliable predictor of treatment effect. Thus, repeating
the cost per QALY saved would fall to US $14 620 [3].
baseline bone marker measurements after 3 months of
therapy is likely to be helpful in the management of
cardiovascular benefit of HRT. Epidemiological studies
osteoporotic patients, since treatment effects can be
consistently show a marked effect of HRT on morbidity
detected before changes in bone mineral density. The
and mortality and the inclusion of these effects into
value of these markers other than in postmenopausal
health economic models provides economic benefits
osteoporosis has not been demonstrated.
greater than those derived from screening high-riskpopulations with bone mineral measurements. This isone of the reasons why the use of bone mineral density
measurements is not recommended for widespreadscreening at the time of the menopause.
There is an increasing need for management strategies to
Different considerations apply to non-HRT interven-
be placed in an appropriate health economic perspective.
tions and to interventions in later life [4]. The cost-
effectiveness studies of calcium and vitamin D focus on
strategies may be performed in several ways. The cost-
hip fracture prevention in the institutionalized elderly.
minimization technique involves the detailed costing of
Treatment of this subgroup of the population with
alternatives, and is dependent on the assumption that the
parenteral vitamin D may lead to resource savings. The
outcomes of different treatments are identical – an
addition of oral calcium reduces the cost-effectiveness of
assumption that is not true for medical interventions in
such a strategy, but compares favourably with other
osteoporosis. Cost-benefit analysis is a preferable form
of economic evaluation, but this requires that all the
The cost-effectiveness of a bone densitometry service
effects produced by an intervention are translated into
for clinical indications is less clear. The indications
financial terms. The value of life saved, and pain
which have been advocated by these guidelines include:
avoided, is not easily categorized in this way. Cost-
(a) subjects with vertebral fractures coming to clinical
effectiveness analysis involves costing of the alternative
attention, (b) subjects with forearm fractures or radio-
interventions, and measuring the effectiveness in some
graphic osteopenia, (c) the small subset of women who,
simple, unitary measure (for example, the cost per year
after counselling, predicate their decision on long-term
of life saved or the cost per fracture saved). A problem
oestrogen use on knowledge of low bone density, and (d)
with this approach is that the effectiveness measure for
patients commencing long-term high-dose therapy with
different illnesses is likely to vary and comparison across
corticosteroids or who have other rarer secondary causes
diseases becomes difficult. To overcome this limitation a
of osteoporosis (Table 4).
fourth technique of cost-utility analysis has been
In the United Kingdom, with a population of 52
devised. This approach involves the expression of the
million, it is estimated that 120 000 to 175 000 scans
full social costs and effects of the alternative interven-
would be required each year for these indications. The
tions, using an outcome indicator (for example, the
cost-effectiveness of the utilization of bone densitometry
quality adjusted life year; QALY) which can be used
in this way may be assessed using the following
across therapeutic categories.
The majority of economic studies of prevention and
treatment of osteoporosis focus upon the use of HRT at
(a) the underlying annual incidence is 1% for
the time of the menopause. However, analyses are also
vertebral and forearm fracture, 0.3% for hip
available for the use of calcium and/or vitamin D in
J. A. Kanis et al.
(b) referred patients have an underlying risk 3 times
using densitometry as compared with £1206 if all
that of the general population,
patients in the population were given treatment. The
(c) the direct management costs for fractures are
cost-effectiveness of a case finding strategy becomes
£1000 for vertebral and forearm fracture, and
more pronounced as the cost of treatment rises. Thus, for
£4000 for hip fracture,
a treatment that costs £350 per year, the cost per avertedfracture using bone density for clinical indications would
(d) compliance with treatment is 50%,
rise to £2887 in contrast with £8453 per averted fracture
(e) bone densitometry predicts fracture with 50%
if all eligible patients in the population were treated
sensitivity and a 15% false positive rate,
(Table 13). The marginal costs per averted fracture (the
(f) the costs of a density assessment are £38,
extra cost per fracture saved in not utilizing bone mineral
(g) treatment costs and the effects of treatment are for
density assessments) rise progressively with the cost of
5 years and cease when treatment is stopped.
treatment. Thus, the cost-effectiveness of bone mineraldensity measurements improves the more expensive the
For a treatment that costs £50 a year and reduces
therapy (and the longer the duration of treatment).
fractures by 50% skeletal assessment is of uncertain
The cost-effectiveness of preventing vertebral frac-
benefit. Whereas assessment saves resources compared
tures among subjects with established vertebral osteo-
with no assessment (Table 13), the amount is minimal.
porosis also produces estimates which are not dissimilar.
Thus, in this scenario, by treating all patients only an
Assuming a 60% predicted reduction in various
extra £1000 is spent, but about 8 more fractures are
fractures, and annual (1994) costs of treatment, the
costs per fracture averted are as follows: (a) Premarin£138, (b) Prempak C £277, (c) transdermal oestrogen
Table 13. Estimates of cost-effectiveness of a treatment strategy with
£560, (d) Didronel PMO £1880, (e) intranasal calcitonin
and without assessment of bone mineral density. For assumptions see
On the basis of these estimates, the treatment of
Cost of treatmenta
established osteoporosis and the use of bone densito-
(£/averted fracture)
metry for well-defined clinical indications seem to bejustifiable in terms of their cost utility.
Acknowledgements. We are grateful to all the members of the
Scientific Advisory Board and the Board of National Societies forhelpful comments and advice, and also to the following for their help
in response to the early drafts: J. C. Branco, L. Bufalino, J. Compston,
A. J. Dixon, P. Drake, R. Francis, M. Frazer, R. Lindsay, L. J. Melton,
D. Purdie, D. M. Reid, E. Schacht, H. Schwietert and L. van Wersch.
aBoth costs and effects are discounted at 6%.
1. Consensus development conference. Diagnosis, prophylaxis and
Saves £4187 per 1000 women treated.
treatment of osteoporosis. Am J Med 1991;90:170–210.
Saves £5023 per 1000 women treated.
2. World Health Organization. Assessment of fracture risk and its
application to screening for postmenopausal osteoporosis. Techni-
However, the cost-effectiveness of skeletal assessment
cal report series 843. Geneva:WHO, 1994.
by densitometry is more favourable the greater the cost
3. Office of Technology Assessment. Effectiveness and costs of
of treatment. For a treatment that costs £100 per patient
osteoporosis screening and hormone replacement therapy. OTA-BP-H-160. 1995.
per year and reduces fracture rate by 50% over a 5-year
4. National Osteoporosis Foundation of the US. A cost-effective
period, the cost per averted fracture would be £366 by
analysis of diagnosis, prevention and treatment. 1997.
Received for publication 23 April 1997
Accepted on 16 May 1997
Source: http://projetusnet.com.br/~rededmoc/wp-content/uploads/2016/01/08-Osteoporosis_International1997.pdf
Islam and Immunization in Northern Nigeria Department of Anthropology and the Center for Afroamerican and African Studies University of Michigan 101 West Hall, 1085 S. University Ave. Ann Arbor, MI 48109-1107 Ph. (734) 647-9917; fax (734) 763-6077; email: [email protected] Draft chapter from book, Protesting Polio and the Ethics of Eradication in Northern Nigeria. Please do not reproduce or circulate without permission of author.
Revista Brasileira de Farmacognosia Brazilian Journal of Pharmacognosy Anti-hyperlipidemic activity of oryzanol, isolated from crude rice bran oil, on Triton WR-1339-induced acute hyperlipidemia in Somsuvra B. Ghatak, Shital J. Panchal* Department of Pharmacology, Institute of Pharmacy, Nirma University, India.

