Rfs1.fhb.gov.hk
Volume 18 #
Number 4 #
August 2012
Hong Kong MedicAl journAl
The official publication of the
Hong Kong Academy of Medicine
and the Hong Kong Medical Association
Health and Health Services Research
Fund
Research Fund for the Control of
Research Dissemination Reports
Volume 18
Health Services Research
#
A
ugust 2012
HONG KONG MEDICAL JOURNAL
Vol 18 No 4 August 2012
Supplement 3
Health and Health Services Research Fund
Ignatius TS Yu 余德新
Research Fund for the Control of Infectious Diseases
Research Dissemination Reports
PT Cheung 張璧濤
CB Chow 周鎮邦
Editorial
Albert KK Chui 徐家強
Michael G Irwin
HealtH ServiceS reSearcH
Smoking reduction intervention for smokers not willing to quit
KL Chan 陳廣亮
smoking: a randomised controlled trial
KS Chan 陳健生
TH Lam, SSC Chan, ASM Abdullah, V Taam Wong, AYW Chan, AJ Hedley
Henry LY Chan 陳力元
David VK Chao 周偉強
Prevalence of chronic pain, insomnia, and fatigue in Hong Kong
TW Chiu 趙多和
R Fielding, WS Wong
Stanley ST Choi 蔡兆棠
LW Chu 朱亮榮
Neck pain in Hong Kong: a telephone survey on consequences and
WK Hung 熊維嘉
health service utilisation
TL Kwan 關添樂
TW Chiu, SL Leung, KW Lam
Alvin KH Kwok 郭坤豪
Paul BS Lai 賴寶山
Eric CH Lai 賴俊雄
Severe acute reSpiratory Syndrome
Stephen TS Lam 林德深
WY Lam 林永賢
Impact of SARS-coronavirus-encoded proteins on cellular signalling 16
Patrick CP Lau 劉志斌
pathways and cytokine/chemokine gene expression
Arthur CW Lau 劉俊穎
JKL Chan, P Cheung, M He, Z Wu
Nelson LS Lee 李禮舜
Danny WH Lee 李偉雄
Neuroprotection in steroid therapy: a rodent model
KY Leung 梁國賢
KF So, SW Tang, TMC Lee
Danny TN Leung 梁子昂
Thomas WH Leung 梁慧康
WK Leung 梁惠強
Mental health impact of severe acute respiratory syndrome: a
Kenneth KW Li 李啟煌
David TL Liu 劉大立
YK Wing, CM Leung
Janice YC Lo 羅懿之
Herbert HF Loong 龍浩鋒
Role of dendritic cells in SARS coronavirus infection
James KH Luk 陸嘉熙
YL Lau, JSM Peiris, HKW Law
Ronald CW Ma 馬青雲
Ada TW Ma 馬天慧
Detection of body temperature with infrared thermography:
Henry KF Mak 麥嘉豐
Jacobus KF Ng 吳國夫
accuracy in detection of fever
Hextan YS Ngan 顏婉嫦
BMY Cheung, LS Chan, IJ Lauder, CR Kumana
Martin W Pak 白威
Edward CS So 蘇超駒
Characterisation of animal angiotensin-converting enzyme 2
PC Tam 談寶雛
receptors and use of pseudotyped virus to correlate receptor
SW Tang 鄧兆華
binding with susceptibility of SARS-CoV infection
William YM Tang 鄧旭明
KKB Li, CW Yip, CC Hon, CY Lam, F Zeng, FCC Leung
Clement CY Tham 譚智勇
Martin CS Wong 黃至生
Kenneth KY Wong 黃格元
TW Wong 黃大偉
Patrick CY Woo 胡釗逸
TK Yau 游子覺
Advisors on Biostatistics
William B Goggins
Eddy KF Lam 林國輝
Advisor on Clinical Epidemiology
Shelly LA Tse 謝立亞
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 1
Sexually tranSmitted infectionS
Voluntary counselling and testing plus information distribution to
reduce HIV-related risk behaviours among Hong Kong male cross-
Sabaratnam Arulkumaran
border truck drivers: a randomised controlled study
JTF Lau, HY Tsui
United Kingdom
Robert Atkins
Prevalence and risk factors of sexually transmitted infections in
female sex workers in Hong Kong
WCW Wong, YL Yim, TN Leung, H Lynn, DC Ling
Author index
Disclaimer
United Kingdom
Willard Fee, Jr
United States
Robert Hoffman
United States
Sean Hughes
United Kingdom
Arthur Kleinman
United States
Xiaoping Luo
United States
Rainer Schmelzeisen
United Kingdom
Homer Yang
Cyrus R Kumana
Managing Editor
Yvonne Kwok 郭佩賢
Assistant Managing Editors
Warren Chan 陳俊華
Betty Lau 劉薇薇
2 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Dissemination reports are concise informative reports of health-related research supported by funds administered by
the Food and Health Bureau, namely the
Research Fund for the Control of Infectious Diseases (RFCID) and the
Health
and Health Services Research Fund (HHSRF). In this edition, 11 dissemination reports of projects related to health
services research, severe acute respiratory syndrome, and sexually transmitted infections are presented. In particular, three
projects are highlighted due to their potentially significant findings, impact on health care delivery and practice, and/or
contribution to health policy formulation in Hong Kong.
Chronic pain, insomnia, and fatigue are important public health problems but are poorly documented in Chinese
populations. Fielding and Wong1 conducted a cross-sectional, population-based, observational study via structured
telephone interviews on more than 5000 randomly selected ethnic Chinese adults. This study aimed to determine the
prevalence and severity of chronic pain, fatigue, and insomnia in the general adult population of Hong Kong, identify
associated factors, and quantify the health care utilisation associated with these conditions during the preceding 3 months.
The authors found that these chronic symptoms affected a substantial proportion of the general population, with as many
as a quarter of the adult population experiencing at least one of them. There is a considerable burden to society in terms of
individual suffering and to the health care system. Risk factors for the development of these chronic symptoms included
older age, female gender, higher levels of education, and other health problems.
The severe acute respiratory syndrome (SARS) epidemic struck Hong Kong in 2003. Mental health morbidity of
patients was reported during the acute and early discharge period. However, the impact of SARS did not end with the
resolution of the infection. During rehabilitation, many patients faced psychosocial difficulties including stigmatisation,
grief, unemployment, functional impairment, and medical co-morbidities. Despite improvements in their physical
condition, their stress and psychiatric symptoms persisted for up to 12 months. Among SARS survivors, chronic fatigue
was common. Wing and Leung2 investigated
inter alia the prevalence and associated risk factors for psychiatric disorders
and chronic fatigue syndrome in SARS survivors. Nearly half of the SARS survivors had one or more psychiatric disorders
in their lifetime—most of whom still had the disorder 3 years after the SARS epidemic. Chronic fatigue was common
among SARS survivors, and SARS was not simply an infection but a disastrous experience for these patients.
Sexually transmitted infections (STIs) remain a major public health problem in Hong Kong. Sex workers are reservoirs
and vectors for the transmission of STIs in the community. To formulate prevention strategies, the prevalence and risk
factors of STIs among asymptomatic female sex workers (FSW) should be determined. Wong et al3 recruited 511 FSWs
aged 18 to 55 years from the well woman clinic of a non-governmental organisation. The prevalence of hepatitis B surface
antigen positivity, syphilis, gonorrhoea, chlamydia, and HIV were 8.5%, 1.8%, 1.8%, 4.6%, and 0.2%, respectively. Risk
factors for STIs included alcohol consumption, place of origin, a history of termination of pregnancy, higher education
level, having multiple partners, and being a non-smoker. Importantly, the reported inconsistent use of condoms when
having sex with regular partners among FSWs may have a bridging effect in the spread of STIs to other population groups.
The authors note that continued surveillance of STIs in FSWs in Hong Kong is important and suggest that a coherent
policy and holistic approach is necessary to control the spread of STIs in the community.
We hope you will enjoy this selection of research dissemination reports. Electronic copies of these dissemination
reports and the corresponding full reports can be downloaded individually from the Research Fund Secretariat website
(http://www.fhb.gov.hk/grants). Researchers interested in the funds administered by the Food and Health Bureau may
visit the website for detailed information about application procedures.
Supplement co-editors
Dr Richard A Collins
Associate Consultant
Scientific Review Director
(Research Office)
(Research Office)
Food and Health Bureau
Food and Health Bureau
1. Fielding R, Wong WS. Prevalence of chronic pain, insomnia, and fatigue in Hong Kong. Hong Kong Med J 2012;18(Suppl 3):9-12.
2. Wing YK, Leung CM. Mental health impact of severe acute respiratory syndrome: a prospective study. Hong Kong Med J 2012;18(Suppl 3):24-7.
3. Wong WC, Yim YL, Leung TN, Lynn H, Ling DC. Prevalence and risk factors of sexually transmitted infections in female sex workers in Hong
Kong. Hong Kong Med J 2012;18(Suppl 3):42-6.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 3
HEALTH AND HEALTH SERVICES RESEARCH FUND
SSC Chan 陳肇始
Smoking reduction intervention for
ASM Abdullah 阿卜杜拉
smokers not wil ing to quit smoking:
V Taam Wong 黃譚智媛
AYW Chan 陳英偉
a randomised control ed trial
AJ Hedley 賀達理
Key Messages
1. This smoking reduction study examined
the effectiveness of smoking reduction
counsel ing together with free nicotine
China has the largest smoking population in the world, but most smokers are not
replacement therapy (NRT) for smoking
wil ing to quit smoking. In Hong Kong, the prevalence of smoking was 11.8% in
cessation and tested the effectiveness of
2008, according to a household survey.1 Although smoking cessation decreases
brief counsel ing on adherence to NRT
among Chinese smokers who were not
the health risks associated with tobacco use, many smokers were unmotivated
wil ing to quit but intended to reduce
to quit, and 67% of Hong Kong Chinese smokers had never tried to give up
cigaret e consumption.
smoking.1 Smoking reduction may provide an intermediate step for complete
2. The smoking reduction intervention
was effective in helping the
cessation, especial y for those who are unready or unwil ing to quit. Although
unmotivated smokers in quit ing
nicotine replacement therapy (NRT) increases the quit rate, few smokers
(intervention: 17.0% vs control: 10.2%,
P=0.012) and in reducing their daily
undergoing NRT adhere to the recommended regimen.2
cigaret e consumption by 50% or more
(intervention: 50.9% vs control: 25.7%,
There has been no randomised control ed trial on intervention to increase
P<0.001) at 6-month fol ow-up.
3. Our results provided evidence for the
NRT adherence. The present study aimed to evaluate the effectiveness of
effectiveness of smoking reduction
smoking reduction therapy and adherence intervention for 6 months among
intervention, which is important for
Chinese smokers in Hong Kong who were unmotivated to quit smoking. We
planning smoking cessation services.
4. Free NRT was widely accepted by
hypothesised that the smoking reduction and adherence counsel ing would lead
participants (8-week NRT adherence
to a higher rate of abstinence, reduction, and adherence to NRT, compared to
rate: 54.5%). Free NRT together with
smoking reduction counsel ing was a
feasible and cost-effective approach to
help unmotivated smokers to reduce and
quit smoking, especial y in developing
countries like China where NRT is
A single-blinded randomised controlled trial was conducted from October
expensive and not used extensively.
5. The motivation to quit smoking was
2004 to April 2007. Subjects were eligible for inclusion if they were ethnic
not undermined by smoking reduction
Chinese, aged 18 years or above, smoked at least two cigarettes daily, had no
intervention. To the contrary, offering
intention to quit in the near future or had failed in previous attempts to quit
assistance to reduce smoking could
at ract smokers who were not wil ing or
using NRT, intended to reduce smoking within the next 7 days using NRT, had
ready to quit.
no contraindication to NRT, and were not following other smoking cessation
or reduction interventions. People who were psychologically or physically
unable to communicate, pregnant or intending to become pregnant within the
Hong Kong Med J 2012;18(Suppl 3):S4-8
next 6 months, on regular psychotropic medications, or with any serious health
problems such as stroke, palpitations or other life-threatening conditions were
The University of Hong Kong:
Department of Community Medicine, School
of Public Health
TH Lam, AJ Hedley
After informed consent, the subjects were randomised into the control group
Department of Nursing Studies
or one of the two intervention groups. In the control group, subjects received
School of Public Health, Boston University,
simple advice on smoking cessation and a self-help quit ing pamphlet only. In
Boston, USA
the reduction and adherence intervention group, subjects received 15-minute
Professional Services Department, Hospital
face-to-face smoking reduction counsel ing and 3-minute adherence counsel ing
Authority, Hong Kong
for NRT by a trained smoking cessation counsel or. Information on health
Council on Smoking and Health, Hong Kong
consequences of smoking and benefits of quit ing was provided. Smokers were
encouraged to reduce consumption before quit ing. Using the ‘5R' approach
HHSRF project number: 01030611
(relevance, risk, rewards, roadblocks, and repetition), the counsel ing focused
on the importance and function of smoking reduction when complete cessation
Principal applicant and corresponding author:
Prof Tai-Hing Lam
is difficult. In addition, the importance of adherence to the prescribed NRT
Department of Community Medicine, School of
dosage and the advantages of adherence were emphasised. Ways to overcome
Public Health, 5/F William MW Mong Block,
21 Sassoon Road, Pokfulam, Hong Kong SAR,
barriers were discussed. Problem-orientated interventions to improve adherence
were delivered. Strict adherence to the prescribed dosage for at least 4 weeks
Tel: (852) 2819 9280
Fax: (852) 2819 9528
was advised. In the reduction intervention group, subjects received smoking
reduction counsel ing only.
4 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Smoking reduction intervention for smokers not wil ing to quit smoking
For both intervention groups, 1 week of NRT was control groups, and (3) rate of continuous NRT use for 4
provided at the first contact. Further smoking reduction weeks (4-week adherence rate) at month 3 between the two
counsel ing and free NRT were provided at the 1-week intervention groups. Secondary outcome measures were:
and 4-week fol ow-ups. For the reduction and adherence (1) validated quit rate at month 6, (2) self-reported quit rate
intervention group, NRT usage was checked by counting the at month 1, (3) self-reported continuous use of NRT for at
amount of NRT left, and additional adherence counsel ing least 8 weeks, and (4) the number of quit at empts up to
was provided. At month 3, information on NRT use in the month 6.
intervention groups up to 4 and 8 weeks was col ected. At
month 6, al subjects (including controls) were interviewed The required sample size was calculated based on
via telephone using a standard questionnaire. Al self- primary outcome measures to provide at least 90% power
reported quit ers (with 7-day abstinence) and reducers with a significance level of 5%. We estimated that there
(reducing daily consumption by ≥50%) were invited for would be (1) a 4% difference in the self-reported quit rate
biochemical validation of exhaled carbon monoxide and between the intervention and control groups, (2) a 12%
urinary cotinine levels.
difference in the self-reported reduction rate between the
intervention and control groups, and (3) a 10% difference
The primary outcome measures were: (1) self-reported in the adherence rate between the intervention groups.
7-day point-prevalence tobacco abstinence at month Thus, 3246 subjects (1229 in the reduction and adherence
6, (2) self-reported reduction rate (≥50%) of cigaret e intervention group, 1229 in the reduction intervention
consumption at month 6 between the intervention and group, and 788 in the control group) were needed.
Assessed for eligibility (n=14 953)
Excluded (n=13 809)
Not meeting inclusion criteria (n=8578)
Refused to participate (n=5231)
Consented and completed baseline questionnaire (n=1154)
Reduction and adherence group
Reduction intervention group (n=449)
Control group (n=226) received simple
(n=479) received smoking reduction
received smoking reduction counsel ing
advice and self-help quitting pamphlet
counsel ing with adherence intervention
and 1 week's free NRT
and 1 week's free nicotine replacement
Lost to fol ow-up (n=59)
Lost to fol ow-up (n=60)
Lost to fol ow-up (n=10)
Lost contact (n=7)
Lost contact (n=6)
Lost contact (n=5)
At week 1, subjects received further
At week 1, subjects received further
face-to-face (n=404) or telephone
face-to-face (n=376) or telephone
(n=16) smoking reduction counsel ing
(n=13) smoking reduction counsel ing
with adherence intervention and 3
and 3 week's free NRT
Lost to fol ow-up (n=98)
Lost to fol ow-up (n=96)
Lost contact (n=83)
Lost contact (n=80)
At month 1, subjects received further
At month 1, subjects received further
face-to-face (n=347) or telephone
face-to-face (n=331) or telephone
(n=34) smoking reduction counsel ing
(n=22) smoking reduction counsel ing
with adherence intervention and 4
and 4 week's free NRT
Lost to fol ow-up (n=31)
Lost to fol ow-up (n=23)
6-month fol ow-up (n=427)
6-month fol ow-up (n=405)
6-month fol ow-up (n=216)
Fig. Consolidated standards of reporting trials flow chart of the study
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 5
Al analyses were based on the intention-to-treat the reduction and adherence intervention group (22.1%
principle. To test the effectiveness of the smoking reduction vs 16.5% vs 12.4% respectively, Table 1). The fol ow-up
counsel ing and NRT, the two intervention groups were rates of the combined intervention group at the 1-week,
combined and compared with the control group. To test 1-month, and 3-month fol ow-up were 87.2%, 79.1%, and
the effectiveness of the adherence intervention to NRT, 85.9%, respectively. At 6 months, 89.7% of the combined
the two intervention groups were compared. Recruitment intervention group and 95.6% of the control group were
of subjects was stopped upon advice from the Independent fol owed up.
Data Monitoring Commit ee after the interim analysis
showed that the self-reported quit rate at month 6 was
Cigarette consumption and abstinence
significantly different between the intervention and control Smoking status of al subjects was assessed by research
groups, and that the adherence rates to NRT between the assistants at the 6-month fol ow-up by telephone interview.
two intervention groups were almost identical. Tobacco The mean daily cigaret e consumption of the intervention
abstinence rates, reduction rates, and the adherence rates groups was significantly lower than that of the controls
between groups were compared using the Pearson Chi- (9.5 vs 13.1 cigaret es, P<0.001, Table 2). The quit
squared test, odds ratios, and 95% confidence intervals.
rate was significantly higher in the intervention groups
than the controls (17.0% vs 10.2%, P=0.012, Table 2).
Subjects who reported complete abstinence were invited
for biochemical validation, and the participation rate was
From October 2004 to April 2007, 1154 participants were 56.4% (102/181); 74 (quit rate of 8.0%) of the intervention
randomised into the smoking reduction and NRT adherence group subjects passed the validation test, with urinary
intervention group (n=479), the smoking reduction group cotinine concentrations of <115 ng/ml and expired carbon
(n=449), and the control group (n=226). A consolidated monoxide levels of <9 ppm, compared to 10 (quit rate of
standards of reporting trials flow chart detailing the 4.4%) of the controls (P=0.066).
enrolment, al ocation and fol ow-up of participants is
shown in the Figure. Table 1 outlines characteristics of
Smoking reduction and quit attempts
participants and results of baseline measurements. No Successful smoking reduction was defined as a self-reported
significant difference was noted in baseline variables across reduction in daily cigaret es by ≥50% at the 6-month
the three groups, except that there were more females in fol ow-up. The smoking reduction rates were significantly
Table 1. Patients' demographics, smoking profiles, quitting history, and self-efficacy to resist smoking at baseline*
Reduction and adherence
Reduction intervention
intervention (n=479)
Patient age (years)
Tertiary or above
Age started smoking (years)
Years of regular smoking
Daily cigarette consumption
Previous use of nicotine replacement therapy
Self-efficacy to resist smoking†
Importance of reducing smoking
Difficulty in reducing smoking
Confidence in reducing smoking
Confidence in quitting smoking (years)
* Data are presented as No. (%) or mean±SD† Range from 0 indicating not important, not difficult, or not confident at all to 100 indicating very important, very difficult, or very confident
6 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Smoking reduction intervention for smokers not wil ing to quit smoking
Table 2. Abstinence, reduction, quit attempts and adherence rates of the intervention and control groups
Abstinence and reduction rate
No. (%) of subjects
Self-reported 7-day point prevalence quit rate
Biochemical validated quit rate*
Self-reported reduction in daily cigarette consumption by ≥50%
Tried to quit smoking for at least 24 hours within last 30 days
172 (22.9) of 770
(excluding the quitters)
Self-reported 7-day point prevalence quit rate at month 3
Self-reported 7-day point prevalence quit rate at month 6
Biochemical validated quit rate*
4-week adherence rate to nicotine replacement therapy at month 3
8-week adherence rate to nicotine replacement therapy at month 3
* Quitting is confirmed by an expired carbon monoxide level of <9 ppm and a urinary cotinine level of <115 ng/ml
higher in the intervention groups than in the control group, fol ow up, NRT was widely accepted (54.5%), compared
including and excluding the quit ers (50.9% vs 25.7%, to previous studies that have reported rates of 16 to 46%.2-4
P<0.001; 41.2% vs 17.2%, P<0.001, respectively). Those This was likely to be due to provision of free NRT. Cost is
who had an expired carbon monoxide level reduced by ≥1 the main reason for NRT discontinuation; offering free NRT
ppm were classified as validated reducers. The participation with smoking reduction counsel ing is feasible and cost-
rate was 48.9% (171/350). There were more validated effective in helping unmotivated smokers to reduce and quit
reducers in the intervention groups than the control group smoking, especial y for those in developing countries like
(11.2% [104/928] vs 5.3% [12/226], P=0.008). Excluding China where NRT is expensive and not widely used.
the quit ers, more smokers in the intervention groups tried
to stop smoking for at least 24 hours within the previous 30 Reduction counsel ing may undermine smoking
days than controls did (22.9% vs 20.7%, P>0.05).
cessation and smokers' motivation to quit, as smokers
may rationalise that reducing consumption is what they
Adherence to nicotine replacement therapy
can accomplish and perceive reduction as an alternative to
Comparing the two intervention groups, there was no complete cessation.5 Our study does not support this notion.
significant difference in the adherence rates to NRT at week Compared with the controls at month 6, smoking reduction
4 (69.7% vs 67.7%, P=0.51) and week 8 (56.4% vs 52.6%, intervention plus nicotine treatment achieved significantly
P=0.25), as wel as the self-reported 7-day quit rate (14.0% higher abstinence rates, reduction rates, and quit at empts.
vs 12.9%, P=0.91) at month 3. Nonetheless, the quit rate No evidence of undermined motivation for quit ing
was significantly higher in the reduction and adherence smoking was noted. To the contrary, offering assistance to
intervention group (20.9% vs 12.9%, P=0.001).
reduce smoking may at ract the smokers who are unwil ing
or unready to quit.
The main limitation of our study was the difficulty
Smoking reduction counsel ing, with or without NRT in subject recruitment despite vigorous promotional
adherence counsel ing, was effective in helping ‘pre- campaigns, and thus stopping recruitment before reaching
contemplators' to quit or reduce their daily cigaret e our planned number of participants. From our previous
consumption by ≥50%. This is important for planning experience, 60% of the current smokers were not intending
local smoking cessation services (when most smokers are to quit or join a cessation programme. This percentage
unmotivated to quit) and making smoking reduction an was much lower when the smokers were sought from our
intermediate step toward complete cessation.
database. Further studies on new adherence intervention
are needed. Our study provided multi-session counsel ing
In our study, the effectiveness of the 3-minute adherence (baseline, 1-week and 1-month) with telephone fol ow-
counsel ing on NRT was examined. Although there was no up, but 20% of the participants were lost to fol ow-up and
significant difference in the 4-week and 8-week adherence hence did not receive the complete intervention, possibly
rates between the two intervention groups at the 3-month weakening effectiveness.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 7
smoking reduction counsel ing, Mr Alex Au Yeung for
coordination and data analysis, and student helpers from
Smoking reduction counsel ing together with NRT was the University of Hong Kong for assistance.
effective in achieving smoking reduction and complete
cessation for smokers who were not ready to quit. Although
References
there was no significant difference in the 4-week and 8-week
adherence rates to NRT between the two intervention 1. Census and Statistics Department. Thematic Household Survey,
groups, the group receiving the adherence intervention
Report No. 36: Pattern of Smoking. Hong Kong: 2008.
2. Lam TH, Abdullah AS, Chan SS, Hedley AJ; Hong Kong Council
achieved a significantly higher quit rate.
on Smoking and Health Smoking Cessation Health Centre (SCHC)
Steering Group. Adherence to nicotine replacement therapy
versus quitting smoking among Chinese smokers: a preliminary
investigation. Psychopharmacology (Berl) 2005;177:400-8.
This study was supported by the Health and Health Services 3. Bolliger CT, Zellweger JP, Danielsson T, et al. Smoking reduction
with oral nicotine inhalers: double blind, randomised clinical trial of
Research Fund, Food and Health Bureau, Hong Kong
efficacy and safety. BMJ 2000;321:329-33.
SAR Government (#01030611). We thank the Hong Kong 4. Etter JF, Laszlo E, Zellweger JP, Perrot C, Perneger TV. Nicotine
Council on Smoking and Health and Pfizer Inc. for support.
replacement to reduce cigarette consumption in smokers who
We also thank the trained smoking cessation counsel ors
are unwilling to quit: a randomized trial. J Clin Psychopharmacol
(Dr Doris Leung, Mr Bernard Yeung, Ms Lorraine Chiu, Mr 5. Warner KE. Tobacco harm reduction: promise and perils. Nicotine
David Wong, and Mr Al an Lau) for providing professional
Tob Res 2002;4(Suppl 2):S61-71.
8 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
HEALTH AND HEALTH SERVICES RESEARCH FUND
R Fielding 莊日昶
WS Wong 黃穎詩
Prevalence of chronic pain, insomnia,
and fatigue in Hong Kong
Key Messages
1. Chronic pain, insomnia and
fatigue affect a substantial
proportion of the Hong Kong
general population; as much as
Chronic pain, insomnia, and fatigue are important public health problems but are
a quarter of the adult population
poorly documented in Chinese populations. About 11% of Hong Kong's adult
experience one of these chronic
population are affected by chronic pain and insomnia. The prevalence of fatigue
symptoms. The prevalence
among women has been reported to be as high as 71%. There may be considerable
of comorbidity is also high,
overlapping among these three symptoms, but the extent of comorbidity is
impacting nearly one-third of
uncertain. These chronic symptoms pose significant burdens on the health care
the adult population. This is a
system, social security, and quality of life of those affected. This study aimed to:
considerable burden to society
(1) determine the prevalence and severity of chronic pain, fatigue, and insomnia
in terms of individual suffering
in the general adult population of Hong Kong; (2) identify associated factors; and
and disability and to the health
(3) quantify the health care utilisation associated with these conditions over the
preceding 3 months.
2. Those who are older, female,
more educated, married or
Subjects and methods
divorced, or with other health
problems are more likely
This cross-sectional, population-based, observational study was conducted from
to develop these chronic
February 2007 to September 2008. A random sample of 5001 Chinese adults
aged ≥18 years was recruited to complete a structured telephone interview.
Chronic pain was first identified using two questions: "Are you currently
troubled by physical pain or discomfort, either al the time or on and off?" and
"Have you had this pain or discomfort for more than 3 months?"1 Subjects
answering yes to both questions were then asked about the severity, site, and
duration of their pain. The severity of current pain and pain over the previous
6 months was assessed using the Chronic Pain Grade questionnaire2 and was
classified into five grades: grade zero (pain free), grade I (low disability, low
intensity), grade II (low disability, high intensity), grade III (high disability,
moderately limiting), and grade IV (high disability, severely limiting). According
to the International Association for the Study of Pain in 1986,1 chronic pain is
defined as pain that has persisted for at least 3 months. We therefore changed the
time frame of the questionnaire items to 3 months.
The Pit sburgh Sleep Quality Index3 was used to assess chronic insomnia.
It evaluates multiple dimensions of sleep over a 1-month period.4,5 There are
Hong Kong Med J 2012;18(Suppl 3):S9-12
19 items generating seven components: subjective sleep quality, sleep latency,
sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping
School of Public Health, The University of
Hong Kong
medication, and daytime dysfunction. The sum of the seven component scores
yields one global score of subjective sleep quality ranging from 0 to 21; higher
Department of Applied Social Studies, City
scores indicate poorer subjective sleep quality. A global score of >5 is defined as
University of Hong Kong
having chronic insomnia.3-5
HHSRF project number: 04060591
Chronic fatigue (defined as fatigue for more than 6 months) was assessed
using the Chalder Fatigue Scale,6 which consists of 11 items measuring severity
Principal applicant and corresponding author:
Prof Richard Fielding
of physical and mental fatigue in the past 6 months using two subscales.
School of Public Health, Li Ka Shing Faculty
Responses 1 and 2 are dichotomised as a score of 0, whereas responses 3 and 4
of Medicine, The University of Hong Kong,
are dichotomised as a score of 1. The highest total fatigue score is 11, a cut-off
5/F William MW Mong Block, Faculty
score of ≥8 is defined as having chronic fatigue.6,7
of Medicine Building, 21 Sassoon Road,
Pokfulam, Hong Kong SAR, China
Tel: (852) 2819 9288
Mental health was evaluated with the Hospital Anxiety and Depression
Fax (852) 2855 9528
Scale,8 which assesses emotional wel -being in people with physical il ness,
minimising contamination by physical symptoms. It comprises two subscales,
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 9
Fielding and Wong
one measuring anxiety and another measuring depression.
years, 34.0%; ≥60 years, 46.9%). For chronic fatigue, the
prevalence was 10.7% and it was most common in the age-
Quality of life (QoL) was measured using the 12- group of ≥60 years (14.1%) [Table].
item Short-Form Health Survey (SF-12) that consists of a
physical component score and a mental component score.9,10 The prevalence of these chronic symptoms was higher
among women, with chronic insomnia being the most
Health care utilisation was assessed using the Thematic common (43.1%), fol owed by chronic pain (39.9%), and
Household Survey 2002,11 which comprises a series of chronic fatigue (13.1%). The prevalence of only one of the
household surveys conducted by the Census and Statistics chronic symptoms was 13.3% and was similar between
Department to col ect statistics on the health status of local males (13.6%) and females (13.0%). The prevalence of any
residents and pat erns of doctor consultation, hospitalisation, two of the chronic symptoms (comorbidity) was 13.8% and
dental consultation, the provision of medical benefits was most common in the middle-aged groups (40-49 years,
by employers/companies, and the coverage of medical 15.7%; 50-59 years, 16.1%) and among females (15.8%).
insurance purchased by individuals. In the present study, The prevalence of al three chronic symptoms (multiple
questions pertaining to doctor consultation, whether having comorbidities) was 4.3% and was more common in females
chronic or long-term disease, and types of diseases were (5.7%) than males (2.6%), and most common in the age-
group of 40 to 49 years (5.0%).
Sociodemographic data was gathered using questions on Factors associated with increased odds of chronic
gender, age, education, marital status, religious affiliations, pain included female gender, older age, being divorced/
income, and employment status. Questions pertaining to separated, higher education level, working part-time,
lifestyle (tobacco use, alcohol consumption, and physical having had chronic health problems, poor mental health,
activity) were modified from the Thematic Household and lower QoL score. Students and those taking regular
Survey to suit the needs of telephone interviewing. exercise had lower odds of chronic pain. Those having
Questions on smoking status, drinking, and exercise habits chronic insomnia were more likely to be female, practising
were also included.
Buddhism/Daoism/ancestor worship, having had chronic
health problems, poor mental health, and lower mental QoL
score. Compared to those with no religion, respondents who
were Catholic were less likely to report chronic insomnia.
Of the 5001 respondents, 55% were women; 70.2% had no Factors associated with increased odds of chronic fatigue
religious affiliation; and 65% reported a monthly household included younger age, being retirees or housewives, having
income below HK$25 000. In terms of marital status, had chronic health problems, poor mental health, and lower
education, and employment, 34.1% had never married QoL score. Compared to those who did not exercise, those
whereas 59.9% were married/cohabited; 19% had completed who exercised three to five times a week were less likely to
tertiary education whereas 45% had at ained secondary report chronic fatigue.
education; and 47.2% were in ful -time employment. Those
aged 40 to 49 years constituted the largest proportion of Factors significantly associated with increased odds of
having any of the two chronic symptoms included female
gender, older age, Christian, higher education level, having
For chronic pain, the prevalence was 34.2% and it was had chronic health problems, poor mental health, and lower
most common in the age-group of 40 to 49 years (41.7%). QoL score. Compared to those who did not exercise, those
For chronic insomnia, the prevalence was 39.4% and it was who exercised one to two times per week had lower odds
least common in the youngest and oldest age-groups (18-29 of having any of the two symptoms. Females, older age,
Table. Prevalence of chronic pain, insomnia, and fatigue by age and gender*
Only one symptom
Entire sample 34.19 (33.26-35.13) 39.42 (38.34-40.50) 10.72 (10.43-11.00) 13.30 (12.94-13.65) 13.84 (13.47-14.21) 4.30 (4.19-4.40)
22.68 (22.07-23.29)
34.0 (33.07-34.93)
11.62 (11.31-11.93) 11.04 (10.75-11.33) 3.17 (3.10-3.24)
33.84 (32.91-34.76) 73.49 (71.47-75.51)
12.33 (12.00-12.66) 14.52 (14.13-14.91) 3.84 (3.74-3.93)
41.66 (40.52-42.80) 72.12 (70.14-74.11) 10.90 (10.61 -11.18) 14.67 (14.28-15.06) 15.67 (15.25-16.10) 5.03 (4.90-5.15)
39.98 (38.88-41.07) 68.46 (70.34-66.58) 10.79 (10.50-11.07) 15.36 (14.95-15.77) 16.06 (15.63-16.49) 4.81 (4.69-4.93)
37.11 (36.09-38.12) 46.92 (45.63-48.21) 14.13 (13.75-14.51) 13.05 (12.71-13.40) 13.48 (13.12-13.84) 4.75 (4.63-4.86)
28.26 (27.49-29.02) 35.12 (34.16-36.08)
13.64 (13.28-14.00) 11.43 (11.12-11.73) 2.61 (2.56-2.67)
39.85 (38.76-40.94) 43.08 (41.90-44.26) 13.09 (12.74-13.44) 13.01 (12.67-13.36) 15.82 (15.40-16.25) 5.69 (5.54-5.83)
* Data are presented as % (95% CI)
10 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Prevalence of chronic pain, fatigue, and insomnia in Hong Kong
being married, divorced or separated, having had chronic had chronic health problems, and those who lacked regular
health problems, poor mental health, and lower QoL score exercise had higher odds of comorbidities. These findings
were more factors conferring increased odds of having all were in agreement with those in the UK study.7 In addition,
three chronic symptoms. Compared to those with a monthly poor mental health and lower QoL score were associated
household income below HK$15 000, those with monthly with the presence of multiple chronic symptoms.
household incomes ranging from HK$40 000 to HK$59 999
had lower odds of having al three chronic symptoms.
After control ing for gender, age, and chronic health
problems, more severity in chronic pain, insomnia, and
Regarding health care utilisation for those with chronic fatigue was associated with greater use of health care
pain, insomnia, and fatigue, 47%, 49%, and 55.5%, services, which is consistent with previous studies in the
respectively, had visited at least one type of western West.2,14,17-19 Lower utilisation rates in the public sector by
medicine practitioner, and 31%, 30.2%, and 32.6%, those with chronic pain or fatigue may be due to difficulties
respectively, had consulted at least one type of therapist, in accessing public services and the lack of pain clinics in
with Chinese herbal medicine practitioner being the most Hong Kong. Chinese herbal medicine was the most popular
common (17.6%, 17.6%, and 19.8%, respectively). The type of alternative therapy for those with chronic symptoms,
use of self-medication was high (49.5%, 43.4%, and and about 25% of the respondents had consumed over-the-
45.2%, respectively), whereas 25.4%, 24.6%, and 24.4%, counter western preparations. Self-medication is cheaper
respectively, had consumed over-the-counter western and is the first resort for those who do not view their
problems as life-threatening.
Older age and having had chronic health problems
Acknowledgement
were significantly associated with one, two, and al levels
of health care utilisation (al P<0.05). Higher pain score This study was supported by the Health and Health Services
was significantly associated with al three levels of health Research Fund, Food and Health Bureau, Hong Kong SAR
care utilisation (al P<0.001). Higher insomnia and fatigues Government (#04060591).
scores were associated with two and al levels of health care
utilisation (P<0.05). The number of symptoms, lifestyle,
References
mental health, and QoL score were not associated with
levels of health care utilisation.
1. Classification of chronic pain. Descriptions of chronic pain
syndromes and definitions of pain terms. Prepared by the International
Association for the Study of Pain, Subcommittee on Taxonomy. Pain
Based on our sample, the estimated point prevalence 2. Von Korff M, Dworkin SF, Le Resche L. Graded chronic pain status:
an epidemiologic evaluation. Pain 1990;40:279-91.
of chronic pain, insomnia, and fatigue in the Hong 3. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the
Kong general population are 28.6%, 32.5%, and 8.8%,
Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in
respectively, which corresponds to 0.6 to 1.8 mil ion middle-
primary insomnia and control subjects. Qual Life Res 2005;14:1943-
aged women. Our estimates for chronic pain and insomnia
are comparable to those reported in western populations (2- 4. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ.
The Pittsburgh Sleep Quality Index: a new instrument for psychiatric
45% for chronic pain, 10-48% for chronic insomnia),3,8-10
practice and research. Psychiatry Res 1989;28:193-213.
whereas our estimate for chronic fatigue is much lower than 5. Buysse DJ, Reynolds CF 3rd, Monk TH, Hoch CC, Yeager AL,
that reported in western populations (23.6%).12-16
Kupfer DJ. Quantification of subjective sleep quality in healthy
elderly men and women using the Pittsburgh Sleep Quality Index
(PSQI). Sleep 1991;14:331-8.
In our sample, the prevalence of multiple chronic 6. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a
symptoms was high. The estimated point prevalence of
fatigue scale. J Psychosom Res 1993;37:147-53.
comorbidity in the Hong Kong general population is 11.4%, 7. Aggarwal VR, McBeth J, Zakrzewska JM, Lunt M, Macfarlane
which represents about 0.6 mil ion adults. The prevalence
GJ. The epidemiology of chronic syndromes that are frequently
of comorbidity was higher in the middle-aged group and
unexplained: do they have common associated factors? Int J
among women. Our estimate for comorbidity is higher than 8. Zigmond AS, Snaith RP. The hospital anxiety and depression scale.
that in a UK study reporting 6% for only one symptom and
Acta Psychiatr Scand 1983;67:361-70.
2% for comorbidity.7
9. Loge JH, Kaasa S, Hjermstad MJ, Kvien TK. Translation and
performance of the Norwegian SF-36 Health Survey in patients with
In our sample, the presence of chronic or long-term health
rheumatoid arthritis. I. Data quality, scaling assumptions, reliability,
and construct validity. J Clin Epidemiol 1998;51:1069-76.
problems was associated with the three chronic symptoms, 10. Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health
suggesting involvement of other physical il nesses. There
Survey: construction of scales and preliminary tests of reliability and
was also an age-related trend. Lack of regular exercise was
validity. Med Care 1996;34:220-33.
associated with chronic pain and fatigue, reflecting both 11. Department of Census and Statistics. Thematic Household Survey.
reverse causality and inadequacy of the activity assessment
Hong Kong: Census and Statistics Department; 2003.
12. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances
questions for pain. Women, older age-groups, those having
and psychiatric disorders. An opportunity for prevention? JAMA
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 11
Fielding and Wong
Prevalence of chronic benign pain disorder among adults: a review of
13. Kroenke K, Price RK. Symptoms in the community. Prevalence,
the literature. Pain 1998;77:231-9.
classification, and psychiatric comorbidity. Arch Intern Med
17. Eriksen J, Jensen MK, Sjogren P, Ekholm O, Rasmussen NK.
Epidemiology of chronic non-malignant pain in Denmark. Pain
14. Kuppermann M, Lubeck DP, Mazonson PD, et al. Sleep problems
and their correlates in a working population. J Gen Intern Med
18. Hickie I, Hadzi-Pavlovic D, Ricci C. Reviving the diagnosis of
neurasthenia. Psychol Med 1997;27:989-94.
15. Mellinger GD, Balter MB, Uhlenhuth EH. Insomnia and its treatment.
19. Von Korff M, Wagner EH, Dworkin SF, Saunders KW. Chronic pain
Prevalence and correlates. Arch Gen Psychiatry 1985;42:225-32.
and use of ambulatory health care. Psychosom Med 1991;53:61-
16. Verhaak PF, Kerssens JJ, Dekker J, Sorbi MJ, Bensing JM.
12 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
HEALTH AND HEALTH SERVICES RESEARCH FUND
TW Chiu 趙帶榮
SL Leung 梁兆麟
Neck pain in Hong Kong: a telephone
survey on consequences and health
Key Messages
1. The prevalence of neck pain
in the past 12 months in our
sample was 64.6%. Of those
with neck pain, 37.8% had
Neck pain is common among Hong Kong people.1 Nonetheless, information on
moderate to severe pain;
the health service utilisation by people with neck pain, and the consequences
13.7% had to limit their social
and cost of neck pain management is lacking. Without objective population
activities; and 18.9% had to
data, patient-centred clinical studies on the efficacy of various therapeutic or
limit their work.
rehabilitation programmes and planning of budgets and resources al ocation for
management of neck pain are based on estimates of impact.
and administrators were at
significantly higher risk of
This study aimed to (1) investigate the consequences of neck pain in terms
having neck pain, compared
of disability and rate of absenteeism from work, (2) describe the health service
with housewives or those who
utilisation pat ern of neck pain sufferers in Hong Kong, and (3) analyse factors
were unemployed or retired.
associated with neck pain and health services utilisation in neck pain sufferers.
3. Of the neck pain sufferers,
service practitioners: medical
consultation in a public
This study was conducted from October 2007 to September 2009. A regional y
or private clinic was most
representative telephone survey using a two-stage randomisation process (of
common (9.2%), followed by
the telephone numbers and the respondents in the households) was carried out.
physiotherapy (4.9%). For self-
The inclusion criteria were Hong Kong residents older than 15 years and ability
care treatment, massage was
to communicate in Cantonese. Verbal consent was obtained before starting the
most preferred (83.3%).
4. Physiotherapy was regarded as
the most effective treatment;
60.7% of those receiving
Of 6754 telephone numbers dial ed, 4640 subjects were selected and successful y
complete improvement. Self-
interviewed. The response rate was 68.7%. The mean duration of the interviews
massage was less effective;
(for respondents who met the definition of neck pain) was 15.7 (standard
59.5% of those who self-
deviation, 3.4; range, 7-39) minutes.
massaged had an improvement
of half or less.
Of the 4640 respondents, 2997 (64.6%) reported having neck pain in the
previous 12 months. In 166 (5.5%) neck pain sufferers, the neck pain was
confirmed by a physician as being work-related. The most common cause (as
speculated by the respondents) was poor sleeping posture (25.6%), fol owed
by work (22.3%) and others (18.4%) [Table 1]. The pain was mild in 59.1%
Hong Kong Med J 2012;18(Suppl 3):S13-5
and moderate to severe in 37.8%; 13.7% had to reduce their social activities;
18.9% had to limit their work; 11.6% reported that neck pain disturbed their
Department of Rehabilitation Sciences, The
daily activities; and 3.6% applied for sick leave owing to neck pain during the
Hong Kong Polytechnic University
TW Chiu, SL Leung
past 12 months. The mean duration of disturbance in 271 subjects was 65.5 days,
whereas the mean total sick leave duration for 100 subjects was 19.4 days.
Females had a significantly higher prevalence than males (68.1% vs 59.5%,
HHSRF project number: 05060261
P<0.001). Managers, professionals, and administrators had the highest prevalence
Principal applicant and corresponding author:
(81.6%), whereas 65.1% of those who were unemployed and retired had neck pain.
Department of Rehabilitation Sciences, The
Regarding utilisation of health services in the past 12 months, 25.2% of those
Hong Kong Polytechnic University, Hung
Hom, Hong Kong SAR, China
with neck pain consulted health service practitioners in the past 12 months:
Tel: (852) 2766 6709
medical consultation in a public or private clinic was most common (9.2%),
Fax: (852) 2330 8656
fol owed by physiotherapy (4.9%). For self-care treatment, massage was most
preferred (83.3%) [Table 2].
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 13
Table 1. Cause of neck pain and severity
A total of 2431 subjects with neck pain identified the
No. (%) of subjects
treatment they considered most effective for neck pain
al eviation; 86.6% believed that their neck pain improved
fol owing treatment; 50.1% considered that the neck
Cause of neck pain (as speculated by
pain reduced completely or by more than half (Table 2).
Physiotherapy was regarded as the most effective treatment;
60.7% of those receiving physiotherapy achieved complete
improvement. Massage was the most preferred self-care
treatment, but 59.5% of those who self-massaged had an
improvement of half or less.
Mentally unstable
Poor sleeping posture
Height of pillow not appropriate
For the worldwide adult population (age 17-70 years),
Severity of recent episode
the 12-month prevalence of neck pain ranges from 16.7%
to 75.1% (mean, 37.2%).2 In this study, the prevalence
was 64.6%, which is higher than the 53.6% reported
in our previous study in 2006.1 The percentage of neck
pain sufferers having moderate-to-severe neck pain was
Social activities
also higher (37.8% vs 15%1); 13.7% (compared to 4.8%
Normal, without extra pain
Normal, but with extra pain
in 20061) had to reduce their social activities; and 4%
(compared to 0.3% in 20061) had to stay at home or stop
their social activities. Neck pain caused a mean disturbance
Completely stopped
of 65.5 days in the past year; 18.9% of neck pain sufferers
Job or household work
(compared to 3.1% in 20061) had to limit their work; and
3.6% had to apply for sick leave (mean, 19.4 days). These
Able to perform normal tasks with pain
Shorten the normal work/job by <50%
results suggest that the severity and impact of neck pain in
Shorten the normal work/job by >50%
the general adult population in Hong Kong is higher than
Can't work at all
that in 2006.
No response/refused to answer
Table 2. Pattern of health services utilisation and self-care, choice of most effective treatment, and degree of improvement
Self-rated improvement in neck pain after treatment
treatment (n=2431) Less than half
Health service provider
Chinese massage therapy
Self-care treatment*
Ointment and medicine plaster
* More than one item may be chosen; items may not be exclusively for treating neck pain
14 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Neck pain in Hong Kong
Managers, professionals and administrators were at from 2.8% in 2006.1 Nonetheless, it is inappropriate to use
significantly higher risk of having neck pain, likely owing the results of this observational study to assess the efficacy
to highly competitive working environments, excessive of various treatments for neck pain. Randomised control ed
stress at work, and long working hours. High levels of trials are warranted.
stress and physical and psychological workplace factors
are predictors of neck pain among workers in industrial and
Limitations
service sectors.3
Despite the high telephone coverage rate in Hong Kong,
In our study, 25.2% of neck pain sufferers (compared to non-coverage bias may stil occur. Application of visual
16.9% in 20061) consulted medical or health professionals. aids to depict the topographical location of neck pain was
Of them, 9.2% (compared to 15.7% in 20061) visited a not feasible. The self-reporting nature of this survey may
medical doctor and 4.9% (compared to 1.7% in 20061) have recal bias.
sought help from physiotherapists. There is a increasing
trend for complementary methods such as Chinese
Acknowledgement
massage therapy (3.5%) or acupuncture (2.7%), compared
to the study in 2006.1 This is comparable to a survey in This study was supported by the Health and Health Services
the United States4 reporting that one in three Americans Research Fund, Food and Health Bureau, Hong Kong SAR
with back or neck pain consulted complementary health Government (#05060261).
professionals. Utilisation of health care resources for neck
pain has increased. In our study, 60.7% and 50.0% of neck
References
pain sufferers reported complete improvement of neck
pain fol owing physiotherapy and medical consultation in 1. Chiu TT, Leung AS. Neck pain in Hong Kong: a telephone survey
private clinics, respectively. This is contrary to the survey in
on prevalence, consequences, and risk groups. Spine (Phila Pa 1976)
the United States4 that reported low perceived effectiveness
of conventional therapies.
2. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the
world population: a systematic critical review of the literature. Eur
Spine J 2006;15:834-48.
Massage (83.3%) and general exercises (52.6%) were 3. Andersen JH, Kaergaard A, Mikkelsen S, et al. Risk factors in the onset
the two most preferred modes of self-care treatment for neck
of neck/shoulder pain in a prospective study of workers in industrial
pain, but their effectiveness was low. Self-medication with
and service companies. Occup Environ Med 2003;60:649-54.
4. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS.
western or Chinese medicine achieved a high percentage
Patterns and perceptions of care for treatment of back and neck pain:
of complete improvement, and their use increased to 13%
results of a national survey. Spine (Phila Pa 1976) 2003;28:292-8.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 15
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
JKL Chan 陳家駱
P Cheung 張寶燕
Impact of SARS-coronavirus-encoded
proteins on cel ular signal ing
pathways and cytokine/chemokine
Key Messages
1. Although GFP-tagged ORF8
and ORF3 potently activate the
JNK and p38 MAPK pathways,
expression of non-tagged
SARS-CoV-encoded ORF8 or
Severe acute respiratory syndrome coronavirus (SARS-CoV) was responsible
ORF3 has no obvious effect.
for the global SARS pandemic in 2003.1,2 Although al CoVs have similar
2 Although both GFP-tagged
microscopic appearance, gene products, and genomic organisation, SARS-
ORF8 and ORF3 induce cell
CoV is unique in that it is associated with high mortality rates in humans.
death, expression of non-
Spike, membrane, envelope, and nucleocapsid proteins as wel as replicase are
tagged ORF8 or ORF3 has no
commonly conserved among al CoVs. The genome of SARS-CoV also encodes
obvious effect on cell survival.
nine other novel open-reading frames (ORFs) with unknown functions (Fig 1).1,2
3 Addition of an epitope tag to a
protein of interest, a common
Various viruses exert their pathogenic effects through interaction of their
way to study novel proteins
viral proteins with distinct cel ular targets. We hypothesised that the severe
in the absence of suitable
inflammation and high mortality caused by SARS-CoV are contributed in part by
antibodies, may generate
these novel ORFs. Therefore, we aimed to evaluate the functions of these novel
unexpected artefacts. Caution
ORFs by overexpressing them in human cel lines.
should be taken with any results
derived from epitope-tagged
Mitogen-activated protein kinases (MAPK) are important cel ular signal ing
molecules involved in cel growth, differentiation, and apoptosis under both
4 When studying a novel protein,
normal and pathological conditions. Three major classes of MAPKs, namely
it is essential to prepare
extracel ular signal-regulated kinases, cJun N-terminal kinases (JNKs), and p38
suitable antibodies to facilitate
MAPKs, have been extensively characterised in the past 15 years. Many viral
detection and purification (eg
proteins are known to activate these MAPKs to exert their cytotoxic effects and
by immunoprecipitation) of the
trigger host inflammatory responses. For example, the Tax protein of human
native or endogenous proteins.
T-cel leukaemia virus type 1 and the latent membrane protein 1 (LMP1) of the
Epstein-Barr virus potently activate the JNK pathway. We hypothesised that the
novel ORFs of SARS-CoV may trigger inflammation and promote apoptosis of
host cel s through activation of MAPKs, especial y the JNK and p38 MAPKs,
which are known to be activated by pro-inflammatory and apoptotic stimuli.
Hong Kong Med J 2012;18(Suppl 3):S16-9
This study was conducted from September 2004 to December 2006. To amplify
the novel SARS ORFs from the SARS-CoV genome and to insert them into two
Department of Biochemistry, Hong Kong
sets of expression vectors (Flag-tagged pcDNA3 and eGFP-tagged pEGFP-C1),
University of Science and Technology
two sets of polymerase chain reaction primers were respectively designed:
JKL Chan, P Cheung, Z Wu
one containing the Nhe I (or Xba I for ORFs3 and 14)/Not I sites and another
Centre for Emerging Infectious Diseases,
The Chinese University of Hong Kong
containing the Bgl II/Sal I sites. Al constructs were verified by restriction
enzyme digestion and sequencing.
RFCID project number: 01030802
Al DNA constructs were transiently transfected into HEK293 cel s using
Principal applicant and corresponding author:
Lipofectamine Plus reagents (Invitrogen) fol owing the manufacturer's
instructions. Fluorescent images of live HEK293 cel s containing green
Department of Biochemistry, Hong Kong
fluorescence protein (GFP) fusion proteins were acquired by an Olympus IX70
University of Science and Technology, Clear
fluorescent microscope linked to a charge-coupled device digital camera (Spot
Water Bay, Kowloon, Hong Kong SAR,
RT, Diagnostic Instruments Inc, MI, USA).
Tel: (852) 2358 8704
Fax: (852) 2358 1552
HEK293 cel s were co-transfected with HA-JNK2 together with individual
Email:
[email protected]
viral ORFs. After 24 hours of transfection, cel s were harvested, lysed, and
16 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Impact of SARS-coronavirus-encoded proteins
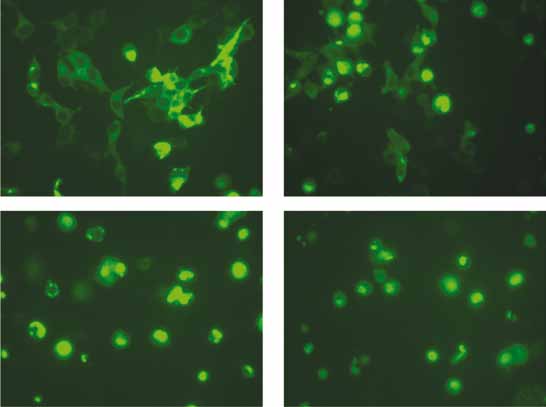
Fig 1. Expression of GFP-ORF8 in HEK293 cells results in significant cell death
HEK293 cells are transiently transfected with a construct encoding GFP-ORF8. At different time points after transfection, fluorescent
images are taken using an Olympus IX70 fluorescent microscope linked to a charge-coupled device digital camera
the soluble whole cel lysates were prepared. After Effect of GFP-ORFs on cell survival
normalisation by Western blot ing, an equal amount of After transfecting GFP-ORFs into HEK293 cel s, the
HA-JNK was immunoprecipitated from cel lysates using behaviour of the GFP-positive cel s was monitored by
anti-HA antibodies. The immunoprecipitates were then fluorescent microscopy every 12 to 24 hours for up to 4
subjected to kinase assays using either GST-cJun(1-79) or days. Several GFP-ORFs, especial y GFP-ORF8, caused
GST-ATF2 (1-92) as substrates.
obvious cel death. After 24 hours of transfection into
HEK293 cel s, GFP-ORF8-positive cel s started to round
A segment of ORF8 gene encoding aa17-94 was up and then detached from culture plates (Fig 1). By 48
subcloned into pET32M expression vector to generate hours, most of the GFP-positive cel s had died. This was
the recombinant His-thioredoxin-ORF8 fusion protein in consistent with other reports.3,4 Similarly, GFP-ORF3,
bacteria. The proteins were injected into rabbits to generate GFP-ORF9, and ORF14 also promoted cel death.
polyclonal antibodies according to standard procedures.
GFP-tagged ORF8 activates both JNK and p38
Based on the finding that GFP-ORF8 promoted cel death,
Subcellular localisation of novel ORFs from SARS-
we tested whether GFP-ORF8 could activate JNK and p38
MAPK (both of which are often activated by pro-apoptotic
As antibodies against the novel ORFs from SARS-CoV stimuli). The HEK293 cel s were co-transfected with GFP-
were not available, an enhanced GFP inframe was first ORF8 together with either HA-JNK2 or HA-p38α. EBV-
fused to the N-terminus of al nine ORFs. After transfecting encoded LMP1 was used as a positive control. In immune-
individual fusion constructs into HEK293 cel s, the complex kinase assays, GFP-ORF8 potently activated both
subcel ular localisation pat erns of these nine ORFs were JNK and p38 as wel as LMP1 (Fig 2).
classified using live cel imaging into three categories: GFP-
ORFs3, 7, 8, 9, and 14 (which were mainly cytoplasmic); There is a 15-aa leader peptide at the N-terminus of
GFP-ORFs10, 11, and 13 (which were evenly distributed in ORF8, which might correct targeting of the viral protein to
both the cytoplasm and nucleus); and GFP-ORF4 (which the endoplasmic reticulum and Golgi networks.5 To make
was mainly nuclear).
sure that the effects seen above were not due to inappropriate
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 17

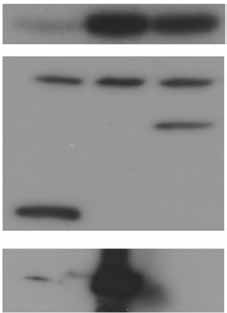
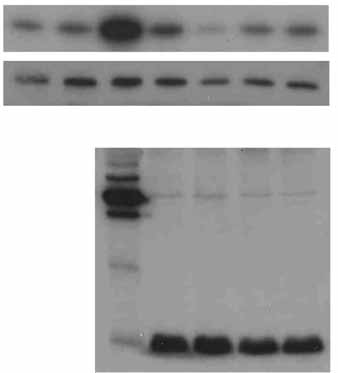
Fig 2. Activation of JNK and p38 MAPK by GFP-ORF8
HEK293 cells are co-transfected with GFP-ORF8 together with either HA-JNK2 or HA-p38α. HA-tagged kinases are immunoprecipitated
from cell lysates and subjected to kinase assays
positioning of the GFP tag in the fusion protein, another
expression construct (ORF8-GFP) was generated with
GFP-fused inframe to the C-terminus of ORF8. When
the construct encoding ORF8-GFP was introduced into
HEK293 cel s, ORF8-GFP was as efficient as GFP-ORF8
(ie the N-terminal y tagged ORF8) in promoting cel death.
Furthermore, when co-transfected together with HA-JNK2
or HA-p38α into HEK293 cel s, ORF8-GFP potently
activated both JNK and p38 as wel as GFP-ORF8.
Non-tagged ORF8 did not cause cell death and
activate JNK and p38
To further exclude the possibility that the effects of ORF8
fusion proteins seen above were caused by inappropriate
fusion of the GFP tag, an expression construct encoding the
native ORF8 was generated, without any additional tag at
either end of ORF8. To ensure that the ORF8 protein was
actual y expressed from the construct, polyclonal antibodies
against ORF8 were generated using recombinant ORF8
protein spanning aa 17-84. The antibodies we used were
able to detect ORF8 either as a GFP-ORF8 fusion protein Fig 3. ORF8 without tag does not activate JNK
or a non-tagged protein (Fig 3). When transfected into HEK293 cells are co-transfected with constructs encoding HA-
JNK2 and non-tagged ORF8. HA-JNK is immunoprecipitated
HEK293 cel s, the non-tagged ORF8 did not cause obvious from cell lysates and subjected to protein kinase assays. The
cel death. In addition, although GFP-ORF8 potently expression of ORF is detected by our locally produced antibodies
activated JNK, the non-tagged ORF8 failed to do so (Fig 3).
Similarly, the non-tagged ORF8 also failed to activate p38.
of live cel s, instant knowledge of subcel ular localisation
pat erns, and tracking of the fate of GFP-positive cel s
To study the cel ular function of novel proteins in the over a long period of time. Although protein tagging is a
absence of suitable antibodies, it has been a widely adopted fast and useful technique (especial y for proteins without
practice to fuse a unique tag (eg HA, FLAG, Myc, etc) to suitable antibodies), addition of a tag to a protein can create
either end of the protein of interest. This facilitates detection artefacts due to changes in protein localisation and folding,
of the protein in cel s and cel lysates and in isolation of the interference or disruption of interaction of the protein with
protein of interest by immunoprecipitation. In recent years, other partners, etc. Therefore, caution is necessary for
GFP has become a very popular tag, as it enables imaging findings derived from tagged proteins.
18 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Impact of SARS-coronavirus-encoded proteins
Owing to the high mortality rate caused by SARS-CoV, and p38 MAPK pathways. We believe that results in
it is essential to understand the molecular mechanisms several reports on ORF8 and ORF3 were most likely due
underlying the pathogenesis. We undertook the project at to artefacts generated by inappropriate fusion of an epitope
a time when many key reagents (including the antibodies tag at either end of the viral proteins.3,4 Therefore, caution
againt ORF8) were not available. GFP-tagged ORF8 was should be exercised in interpreting results derived from
found to potently induce cel death, which was consistent epitope-tagged proteins. Suitable antibodies to the protein
with other reports.3,4 In addition, GFP-tagged ORF8 of interest should be prepared to facilitate the study of the
strongly activated the JNK and p38 MAPK pathways in host native proteins.
cel s. Non-tagged ORF failed to induce these changes; this
suggested that artefacts were generated in the GFP fusion Acknowledgement
proteins. Before obtaining the ORF8 antibody, a segment
of ORF8 gene encoding aa 17-94 was used as the bait in This study was supported by the Research Fund for the
the yeast two-hybrid screening. Several interesting clones Control of Infectious Diseases, Food and Health Bureau,
were found. Owing to the lack of a suitable biological Hong Kong SAR Government (#01030802).
assay for the native ORF8, these clones were not further
References
In addition to ORF8, ORF3 (also known as ORF3a), 1. Rota P, Oberste MS, Monroe SS, et al. Characterization of a novel
coronavirus associated with severe acute respiratory syndrome.
another novel ORF that was found to be expressed in SARS-
Science 2003;300:1394-9.
CoV-infected cel s was also extensively studied. Similarly, 2. Marra MA, Jones SJ, Astell CR, et al. The genome sequence of the
GFP-ORF3 induced cel death and activated both JNK and
SARS-associated coronavirus. Science 2003;300:1399-404.
p38 in host cel s. In contrast, the non-tagged ORF3 failed to 3. Tan YJ, Fielding BC, Goh PY, et al. Overexpression of 7a, a protein
induce cel death and activate JNK and p38 as wel as IkB
specifically encoded by the severe acute respiratory syndrome
coronavirus, induces apoptosis via a caspase-dependent pathway. J
4. Yuan X, Wu J, Shan Y, et al. SARS coronavirus 7a protein blocks cell
cycle progression at G0/G1 phase via the cyclin D3/pRb pathway.
The native (non-tagged) ORF8 and ORF3 did not 5. Fielding BC, Tan YJ, Shuo S, et al. Characterization of a unique
group-specific protein (U122) of the severe acute respiratory
significantly induce cel death, nor did they activate JNK
syndrome coronavirus. J Virol 2004;78:7311-8.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 19
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
SW Tang 鄧兆華
Neuroprotection in steroid therapy: a
TMC Lee 李湄珍
rodent model
Key Messages
1. Chronic steroid therapy causes
disturbance in cell proliferation
of the hippocampus and the
subventricular zone. This may
Corticosteroid decreases neural cel production in the hippocampus,1 whereas
be the underlying cause of
antidepressants induce neurogenesis.2 The hippocampus is a brain region for
altered memory and cognitive
memory formation. Decreased production of neurons in this region has a negative
impact on cognitive function. We assessed the hypothesis that the neuro-damaging
2. Co-administration of paroxetine
effect of high-dose corticosteroid on the hippocampus and subventricular zone
(a class of antidepressants)
(SVZ) could be reversed by administration of paroxetine—a selective serotonin
during steroid therapy could
reuptake inhibitor for treatment of depressive disorders. A rodent model was
counteract the destruction.
used to test the effect of paroxetine, corticosterone, and co-treatment of these two
Modification of the current
drugs on neurogenesis of the hippocampus and SVZ. In patients receiving steroid
steroid therapy regimen may be
therapy, the neuroprotective effect of paroxetine suggests that administration
of antidepressant could prevent deterioration of neuron production. This study
aimed to investigate drug interactions of paroxetine, lithium, and corticosterone
on the hippocampus and SVZ in terms of cel proliferation, dendritic morphology,
neuronal survival, and molecular mechamisms, and whether selective serotonin
reuptake inhibitor and lithium could exert protection against corticosterone-
induced neuron damage on the hippocampus and SVZ.
This study was conducted from January 2005 to December 2006. Six groups
of rats (n=4-5 for each group) were divided into: (1) 14 days of corticosterone
injections (40 mg/kg, subcutaneously), (2) 14 days of paroxetine injections (10
mg/kg, intraperitoneal y), (3) 14 days of both corticosterone and paroxetine
injections (same dosage as above), and (4) 14 days of vehicle injections.
To study the effect of lithium and corticosterone on dendritic morphology, the
rats were divided into: (1) 14 days of lithium treatment (85 μg/kg, n=6), and (2)
14 days of lithium and corticosterone treatment (same dosage as above, n=6).
Proliferative cel s in the hippocampus and SVZ were label ed by
bromodeoxyuridine (BrdU) injection (50 mg/kg) during the final 3 days of
Hong Kong Med J 2012;18(Suppl 3):S20-3
treatment. After 14 days of treatment, rats were sacrificed by decapitation, and
their brains were processed for BrdU immunohistochemistry or Golgi staining.
The University of Hong Kong:
Department of Anatomy
During the treatment period, another set of experimental rats was sacrificed and
their hippocampi were dissected for quantitative polymerase chain reaction.
Department of Psychiatry
For the differentiation and neurogenesis study, the rats were divided into 4
groups as described above, with each group containing 6 rats. The rats were
al owed to survive for 3 weeks after completion of the 14 days' treatment. The
RFCID project number: 01030872
total number of rats used was 135.
Principal applicant and corresponding author:
BrdU immunohistochemistry
Department of Anatomy, The University of
Frozen slices of the hippocampus and SVZ were slide-mounted and boiled in
Hong Kong, 1/F Laboratory Block, Li Ka
citric acid (pH=6.0) for 10 mins, fol owed by PBS rinses. The brain sections
Shing Faculty of Medicine, 21 Sassoon Road,
Pok Fu Lam, Hong Kong SAR, China
were incubated in 1M HCI (37ºC, 30 mins) and then boric acid buffer (pH=8.5,
Tel: (852) 2819 9216
10 mins). After blocking with 5% normal goat serum in 0.01% Triton X-100,
Fax: (852) 2817 0857
sections were incubated overnight with anti-mouse BrdU (1:400, Roche) at 4ºC.
Sections were then incubated for 1 hr with secondary antibody (biotinylated goat
20 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Neuroprotection in steroid therapy
anti-mouse; Vector Laboratories), fol owed by amplification were prepared from snap-frozen rat hippocampi. For each
with an avidin-biotin complex (Vector Laboratories). rat, 50 μg of protein extract was used for assay. ELISA was
Cel s were then visualised with diaminobenzidine. For the carried out according to the manufacturer's protocol.
neurogenesis study, co-immunostaining with rat anti-BrdU
antibody (1:1000, abcam) and mouse anti-NeuN (1:1000, Results
Chemicon) were used as primary antibody. Secondary
antibodies were goat anti-mouse and rat (Alexor fluor 488 Adrenal gland atrophy caused by subchronic
and 563, Molecular Probes). The chemical supplier was corticosterone treatment
Sigma-Aldrich unless otherwise indicated.
After 14 days of treatment, the adrenal glands were dissected
and weighed. Respectively in the control, corticosterone,
co-treatment, and paroxetine groups, the mean adrenal
Golgi staining was carried out using the FD Rapid weights (in g) were 27.63±4.85, 6.20±2.78, 10.633±1.46,
GolgiStain Kit according to the manufacturer's protocol. In and 45.47±14.15. Adrenal weights of the rats in the
brief, the brains of the treated rats were immersed in the corticosterone and co-treatment groups decreased, which
impregnation solution for 2 weeks, after which the tissue indicated hypercortisolaemia induction and chemical y
was cut into 50-micron-thick sections and stained.
induced lesions. This confirmed that the rats were subjected
to chronic exposure of high-dose corticosterone during the
Quantitative polymerase chain reaction
treatment period.
Hippocampi of the rats in the three treatment groups
(corticosterone, paroxetine, and co-treatment) were taken Hippocampal neurogenesis after corticosterone and
out at different time points: 4 hours, 2 days, 4 days, 7 days, paroxetine treatment
and 14 days after treatment. Hippocampal tissues were In the cel proliferation assay, the number of proliferating
dissected and stored at -70ºC until use. Hippocampal RNA cel s was identified by immunohistochemical detection of
was extracted with Trizol reagent (Invitrogen) according BrdU within the nuclei of actively dividing cel s. The BrdU-
to the manufacturer's protocol. Gene expression of brain- positive nuclei were clustered in the subgranular layer and
derived neurotrophic factor (BDNF) and cAMP response hilus and exhibited irregular shape. In the experiment, only
element-binding protein (CREB) among different groups subgranular layer cel s were counted. Compared to the
of rats at different time points were measured by the controls, corticosterone significantly decreased the number
iCycler iQ™ Multi-Color RT-PCR System. The primer of BrdU-label ed cel s in the dentate gyrus (2470.00±31.56
sequences and probe for amplification of BDNF were: vs 1677.38±146.97, P<0.05). Chronic treatment with
5'-CTGACACTTTTGAGCACGTGATC-3' (forward), paroxetine significantly increased BrdU-label ed cel s
and (13255.71±83.98, P<0.001) in the subgranular and granule
5'-CATCCAGCAGCTCTTC-3' (probe). The primer cel layer, compared to the corticosterone or vehicle-alone
sequences of GAPDH (as internal controls) were: group. The number of BrdU-positive cel s in the co-treatment
(forward), group (2204.48±90.40) was not significantly different from
5'-CCGTTCAGCTCTGGGATGAC-3' (reverse), and 5'- the vehicle-treated controls. For neuronal differentiation, no
difference in the percentage of BrdU-label ed cel s showing
NeuN expression was noted among the four groups.
Data quantification and statistical analysis
This indicated that subchronic corticosterone treatment
BrdU-positive cel s on every 12th unilateral section decreased hippocampal neurogenesis, whereas co-treatment
through the whole dentate gyrus were counted at ×1000 with paroxetine increased the effect to a level similar to
magnification, with the aid of the Stereo Investigator controls. In short, antidepressant therapy may be effective
software. BrdU-positive cel s in the dentate gyrus were in preventing neurological damage caused by subchronic or
counted from 2400 to 3600 μm posterior to Bregma. In chronic steroid therapy.
SVZ, BrdU cel s were counted from 1800 to 0 μm anterior
to Bregma. The number of BrdU-label ed cel s per dentate Morphological analysis by Golgi staining
gyrus was then multiplied by 24 to estimate the total Brain tissues were subjected to Golgi staining to study
number of BrdU-positive cel s through the dentate gyrus. morphological changes (dendritic trees and spines) of
The number of BrdU-positive cel s in the hippocampal hippocampal neurons after treatment. In the corticosterone,
subgranular zone in each group was defined as a percentage lithium, and co-treatment groups, at least five neurons were
of control (vehicle). For SVZ sections, the cel number was traced using the Neurolucida software, and the data were
expressed as the number of cel s per section.
analysed using the NeuroExplorer software. The number of
neuronal nodes (ie the number of dendritic tree branches) in
Brain-derived neurotrophic factor enzyme-linked
the corticosterone group was significantly lower than in the
lithium and co-treatment groups (13.5±4.36 vs 32±6.00 vs
BDNF enzyme-linked immunosorbent assay (ELISA) 33.63±12.00, P<0.05). The mean dendritic length of each
kits (Chemicon) were used to assess hippocampal BDNF neuron (in μm) in the corticosterone group was significantly
protein level after 14 days of treatment. Protein extracts smal er than in the other two groups (410.0±49.7 vs
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 21
1762.6±182.4 vs 2068.6±782.9, P<0.05). This indicated thus the serotonergic pathways.3 Lithium could reverse the
that corticosterone decreased dendritic length and the adverse effect of corticosterone on the dendritic complexity
number of dendrite branches, whereas corticosterone plus of the hippocampal CA3 region. Administration of lithium
lithium could reverse the changes.
during steroid therapy may prevent the undesirable effect
of high-dose steroid, but further investigation is needed to
Effect of drug treatment on hippocampal cell death
determine its behavioural consequence. The intracel ular
Cel death in the hippocampus was assessed by Nissl mechanisms responsible for the neurogenic effect remain
staining. No cel s with pyknotic appearance (ie undergoing unclear, but are likely to involve more than one intracel ular
apoptotic cel death) were detected with cresyl-violet pathway. Previous studies have suggested a major role of
staining in any treatment group. This indicated that the cAMP-CREB cascade4 in the process, and that BDNF
subchronic corticosteroid treatment was unlikely to cause may be essential for neurogenesis. In our study, the ELISA
neurological damage by increasing hippocampal cel death, data showed increased levels of BDNF in paroxetine-
and that antidepressants may not exert their therapeutic treated rats.
effect by protecting neurons from apoptosis.
Quantification of change of brain-derived
neurotrophic factor and cAMP response to element-
Paroxetine, a potent selective serotonin reuptake inhibitor,
binding protein after drug treatments
could reverse the adverse effect of corticosteroid on
The quantitative polymerase chain reaction was used for hippocampal and SVZ neurons. Paroxetine could induce
detecting alteration of BDNF and CREB levels in the cel proliferation in both neurogenic regions and restore the
hippocampus. In contrast to expectation, BDNF gene number of hippocampal proliferative cel s in corticosteroid-
expression levels in al treatment groups decreased but not treated rats. Dendritic morphology study revealed that
significantly across the treatment period when compared to lithium may be beneficial for dendritic arborisation under
the stress condition created by corticosterone treatment.
Future studies may investigate the behavioural consequence
Brain-derived neurotrophic factor protein expression of altered neurogenesis and dendritic morphology. Also, the
by enzyme-linked immunosorbent assay
molecular interaction between BDNF and CREB is worth
The BDNF level in the hippocampus decreased significantly studying. Understanding the molecular mechanisms in
in corticosterone-treated rats than in vehicle-treated rats the neuroprotection of antidepressants may help patients
(66.88±4.22 vs 90.2±6.63 ng/mL, P<0.05, ANOVA with undergoing steroid therapy in preventing cognitive
LSD post-hoc test). Co-treatment with corticosterone and deterioration.
paroxetine (87.73±6.65 ng/mL, P>0.05) prevented the effect
of decreased BDNF expression, compared to controls. No Acknowledgements
significant difference was noted between the vehicle group
and paroxetine-treated group (90.2±6.63 vs 99.07±8.42 ng/ This study was supported by the Research Fund for the
mL, P>0.05).
Control of Infectious Diseases, Food and Health Bureau,
Hong Kong SAR Government (#01030872). We thank Ms
Effect of corticosteroid and paroxetine on
Fanny YM Kam, Phil is WF Kau, and Sonata SY Yau for
providing technical assistance, and the Departments of
Similar to the findings for hippocampus cel proliferation, Anatomy, Psychiatry and Psychology of the University of
corticosterone treatment significantly reduced the number Hong Kong for providing space and equipment.
of BrdU-positive cel s in SVZ, whereas paroxetine The results of this study have been published in:
treatment significantly increased the number. Respectively 1. Qiu G, Helmeste DM, Lau WM, Lee TM, Tang SW, So
in the control, corticosterone, paroxetine, and co-treatment
KF. Modulation by paroxetine of suppressive effect of
groups, the numbers of BrdU-positive cel s in SVZ were
corticosterone on adult hippocampal cel proliferation.
324.0±33.3, 264.1±28.1, 434.9±36.2, and 330.9±23.2 cel s/
Neurosci Bul 2007;23:3.
section (P<0.05 for control vs corticosterone and control vs 2. Lau WM, Qiu G, Helmeste DM, Lee TM, Tang SW, So
KF. Corticosteroid decreases subventricular zone cell
Discussion
proliferation, which could be reversed by paroxetine.
Restor neurol neurosci 2007;25:17-23.
Using the cel birth-dating technique (BrdU label ing), the
numbers of proliferative cel s in the hippocampus and SVZ References
were noted to increase with paroxetine treatment. However, 1. Hellsten J, Wennstrom M, Mohapel P, Ekdahl CT, Bengzon J,
no pyknotic cel s were observed in the hippocampus in any
Tingstrom A. Electroconvulsive seizures increase hippocampal
of the treatment groups, indicating that the drugs had no
neurogenesis after chronic corticosterone treatment. Eur J Neurosci
significant effect on cel survival in our treatment paradigm.
The neurogenesis-promoting effect of antidepressants may 2. Malberg JE, Eisch AJ, Nestler EJ, Duman RS. Chronic antidepressant
treatment increases neurogenesis in adult rat hippocampus. J Neurosci
be due to their influence on the serotonergic system and
22 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Neuroprotection in steroid therapy
3. Jacobs BL, Tanapat P, Reeves AJ, Gould E. Serotonin stimulates the
4. Coppell AL, Pei Q, Zetterstrom TS. Bi-phasic change in BDNF
production of new hippocampal granule neurons via the 5-HT1A
gene expression following antidepressant drug treatment.
receptor in the adult rat. Soc Neurosci Abstr 1998;24:199.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 23
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
YK Wing 榮潤國
CM Leung 梁志明
Mental health impact of severe acute
respiratory syndrome: a prospective
Key Messages
1. Psychiatric disorders and
chronic fatigue were common
among severe acute respiratory
syndrome (SARS) survivors
even after 3 years, and were
The severe acute respiratory syndrome (SARS) epidemic struck Hong Kong in
2003. Varying rates of mental health morbidity were reported during the acute
2. Factors associated with the
and early discharge period.1 The impact of SARS did not end with the resolution
post-SARS experience and
of the infection. During the rehabilitation period, many patients had to face
psychosocial difficulties including stigmatisation, grief reactions, unemployment,
functional impairment, and medical co-morbidities. Despite improvements in
frequent recall, medicolegal
physical condition, the stress and psychiatric symptoms persisted even after 1
issues, and working status)
year.2-4 Chronic fatigue was common among SARS survivors.5 There seemed to
were likely to be related to
be a reciprocal association between fatigue problems and psychiatric disorders.
long-term psychiatric disorders
Dysregulation in endocrine functions, especial y of the hypothalamo-pituitary-
and fatigue.
adrenal (HPA) axis, was common in those with psychiatric disorders and chronic
3. A proportion of SARS
fatigue syndrome (CFS).6 This study aimed to investigate the prevalence and
survivors may have partial
associated risk factors for psychiatric disorders and CFS in SARS survivors, and
insufficient adrenal responses,
the association between HPA status and CFS.
but the hypothalamo-pituitary-
adrenal status was not related
to the psychiatric and fatigue
Data were col ected from December 2005 to July 2007 in the Prince of Wales
Hospital. A total of 369 Chinese SARS survivors in the New Territories East
Cluster hospitals were invited to participate. Patients who were not of Chinese
ethnicity and those who had medical il nesses unrelated to SARS were excluded.
Personalised let ers introducing the research aim and method were sent, fol owed
by invitation by telephone. For those who could not be contacted or who declined
to participate in face-to-face interviews, questionnaires were sent out to them.
Subjects were assessed by psychiatrists using the Chinese bilingual version of
the Semi-Structured Clinical Interview (SCID-II). They also completed a series
of psychometric inventories, including the Chinese versions of the Hospital
Anxiety and Depression Scale, revised version of the Impact of Event Scale,
the Global Assessment of Functioning Scale, the Quality of Life Scale, and a
self-reported questionnaire enquiring demographics and subjective experiences
of patients after the SARS infection. In addition, the length of hospitalisation,
history of hypoxia and oxygen supplementation, intensive care unit admission,
duration and dosage of steroid and ribavirin treatment, and presence of physical
Hong Kong Med J 2012;18(Suppl 3):S24-7
comorbidity were col ected after a case-note review supplemented by the
computerised medical information system.
Department of Psychiatry, The Chinese
University of Hong Kong
YK Wing, CM Leung
For the second part of the case-control study, a proportion of the SARS
survivors were invited to undergo endocrine assessment of HPA axis function.
RFCID project number: 03040062
Three consecutive morning salivary cortisol levels and a low-dose short synacthen
Principal applicant and corresponding author:
test (LDSST) were measured. Controls were recruited from the community; they
had no major physical, sleep, or psychiatric disorders. Their fatigue status and 3
Department of Psychiatry, Shatin Hospital,
days of morning salivary cortisol levels were also assessed.
The Chinese University of Hong Kong, 33
Ah Kong Kok Street, Shatin, NT, Hong Kong
Tel: (852) 2636 7748
Fax: (852) 2647 5321
Of the 369 eligible subjects, 233 (63.1%) responded after a mean post-SARS
duration of 39 months. Among these subjects, 181 underwent interviews with
24 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Mental health impact of severe acute respiratory syndrome
SCID-II for assessment of any psychiatric morbidity. Of and background of psychiatric disorder. The HPA axis
whom, 90 were diagnosed with psychiatric illnesses and function (both LDSST and morning salivary cortisol level)
77 were having active psychiatric illnesses at the time was similar in those with and without psychiatric disorders
of interview (Table). The commonest disorders were and/or CFS.
major depressive disorder, post-traumatic stress disorder,
somatoform pain disorder, and panic disorder. Although Discussion
fatigue was a common symptom, only 24 to 40% of
the patients fulfilled various CFS criteria. Those with Nearly half of the SARS survivors had one or more
psychiatric disorders and/or CFS had poorer quality of psychiatric disorders in their lifetime; most stil had
life, more subjective impairments in various functional the disorder, despite more than 3 years since the SARS
aspects, and scored more poorly on all psychometric scales epidemic. Chronic fatigue was common among SARS
survivors. Although both psychiatric disorders and CFS
were closely associated, a proportion of patients developed
In the multivariate analysis, the perception of CFS in the absence of co-morbid psychiatric disorders.
stigmatisation and recal of SARS memories were Both CFS and psychiatric disorders were associated with a
associated with both lifetime and current psychiatric variety of functional impairments.
disorder. In addition, chronic fatigue and working status also
predisposed to the risk of lifetime psychiatric disorder. In SARS was not simply an infection but a disastrous
contrast, the presence of physical il ness at baseline seemed experience for these patients. Indeed, SARS survivors
to protect against the development of psychiatric problems. shared similar psychopathologies with other disaster
The presence of CFS was influenced by medicolegal issues survivors who reported varying rates of post raumatic
(application for SARS fund and involvement in litigation stress disorder (30-40%), depression (25%), and fatigue
process), perceived stigmatisation, worries over avian flu, symptoms (50%).7
Table. Comparison of SARS survivors with or without psychiatric disorder
No psychiatric il ness
Psychiatric illness
Current psychiatric
(lifetime or current)
Mean±SD age (years)
Health care worker at 2003 (% of subjects)
Working at follow-up (% of subjects)
Self-reported questionnaire (% of subjects)
Single/divorced/widowed
Involvement in lawsuit
Worry about avian flu
Never/a little bit
Recall of SARS memories
Mean±SD total Hospital Anxiety and Depression Scale score
Mean±SD total revised Impact of Event Scale score
Chronic fatigue (% of subjects)
Chronic fatigue syndrome (% of subjects)
Mean±SD Global Assessment of Functioning Scale score
Mean±SD World Health Organization Quality of Life Scale
Psychological score
Environmental score
Working ability†
Housework ability†
Social activities†
Leisure activities†
Intimate relationship†
* P<0.05, non-parametric Mann-Whitney U test† Higher scores indicate more subjective impairment; non-case was compared separately with lifetime or current psychiatric case
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 25
Owing to the infectious nature of SARS, the survivors SARS survivors.
and their family members may have been stigmatised
as hazardous with potential for cross-infection.8 The The SARS group was not significantly different from
disabling symptoms (such as fatigue and non-specific pain), the controls in terms of the morning salivary cortisol
functional decline, and lengthy litigation processes may level; subgroup analysis of SARS survivors in terms of
have further increased others' scepticism and stigmatisation. the presence of CFS and psychiatric disorders did not
The perception of stigmatisation was the most consistent yield any significant difference. Similarly, the LDSST
aetiological factor for the development of psychiatric could not differentiate the SARS survivors with or without
disorders and CFS. It may also be amplified by the negative psychiatric and/or fatigue disorders, albeit there was a
cognitive distortion and interpersonal sensitivity commonly proportion of patients who might be considered to have
seen in psychiatric disorders.
partial y insufficient adrenal response to LDSST. Most of
mental y il SARS survivors declined further psychiatric
The SARS epidemic has heightened the perception management, as they worried about ‘double stigmatisation'.
of the risk posed by other potential infectious epidemics
(such as avian flu). Constant alertness to the potential The response rate of 63% was modest, but it was achieved
threats of novel infections may have perpetuated SARS after intensive recruitment strategy and careful explanation
survivors' traumatic experience. Recal of SARS memories and reassurance of confidentiality. The participants could be
and concern about avian flu were predictors of psychiatric regarded as representative of the SARS population of the
disorders and CFS.
New Territories East Cluster hospitals. Not al participants
completed a ful set of assessments. Nonetheless, over 80%
The protective role of physical il ness (at baseline) of them consented to a face-to-face psychiatric interview. In
against the development of psychiatric disorders in this addition, a number of subjects agreed to undergo endocrine
SARS cohort was intriguing. In most studies, the presence measurement. Future study should integrate both mental
of underlying physical il ness usual y predisposes to the and physical complications in assessing the long-term
risk of psychiatric disorder. However, in our SARS cohort, outcome of SARS survivors.
most of the psychiatric disorders occurred after SARS
at acks and in healthy subjects, including health care Conclusions
workers. Those with physical il ness may have had bet er
mental preparation for handling deterioration in health, but Psychiatric disorders and chronic fatigue were highly
there was a selection bias, in which those with serious and prevalent among SARS survivors even after 3 years. They
multiple medical il nesses may have died from the SARS further impaired SARS survivors in various psychosocial
areas. Although relative adrenal insufficiency was noted in
some patients, this did not appear to influence the emergence
Working status seemed to be associated with the of psychiatric disorders or chronic fatigue.
presence of psychiatric disorder. The relationship could be
bidirectional in that unemployment or retirement may have Acknowledgements
resulted in or from psychiatric disorder. Being a health care
worker was associated with a higher risk of post raumatic This study was supported by the Research Fund for the
stress disorder.9 Ongoing adverse experiences during the Control of Infectious Diseases, Food and Health Bureau,
SARS epidemic, the sudden change of status from being a Hong Kong SAR Government (#03040062). Results of
health care worker to patient, and the proximity and similarity this study have been published in ful in: Lam MH, Wing
between their usual working area and ward environment YK, Yu MW, et al. Mental morbidities and chronic fatigue
may have increased their risk of re-experiencing the trauma. in severe acute respiratory syndrome survivors: long-term
fol ow-up. Arch Intern Med 2009;169:2142-7. We dedicate
The association of SARS fund application and litigation this report to al SARS patients. The project could not have
with chronic fatigue needs careful interpretation. Patients succeeded without their cooperation and participation.
with more functional impairments (which may reflect long-
term dysfunction) are more likely to succeed in applying References
to the SARS fund. A large proportion of SARS patients
reported litigation against the health authority and/or 1. Wing YK, Ho SM. Psychiatric morbidity in severe acute respiratory
employers. Those with more fatigue and prominent mental
syndrome (SARS) patients during acute and early recovery stage.
dysfunction might have negative at itude toward the health
In: Chan JC, Taam Wong VC, editors. Challenges of severe acute
respiratory syndrome. Hong Kong: Saunders Elsevier; 2004:525-45.
authority. In addition, the lengthy litigation process might 2. Lam MH, Wing YK, Yu MW, et al. Mental morbidities and chronic
perpetuate their mental anguish. The phenomenon known
fatigue in severe acute respiratory syndrome survivors: long-term
as ‘compensation neurosis' remains a controversial issue.10
follow-up. Arch Intern Med 2009;169:2142-7.
As the litigation process was stil ongoing at the time of this 3. Lee AM, Wong JG, McAlonan GM, et al. Stress and psychological
study, longer-term studies are required to delineate the role
distress among SARS survivors 1 year after the outbreak. Can J
of compensation and litigation in the psychopathology of 4. Tansey CM, Louie M, Loeb M, et al. One-year outcomes and health
26 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Mental health impact of severe acute respiratory syndrome
care utilization in survivors of severe acute respiratory syndrome.
Arch Intern Med 2007;167:1312-20.
8. Lee S, Chan LY, Chau AM, Kwok KP, Kleinman A. The experience of
5. Moldofsky H, Patcal J. Chronic widespread musculoskeletal pain,
SARS-related stigma at Amoy Gardens. Soc Sci Med 2005;61:2038-
fatigue, depression and disordered sleep in chronic post-SARS
syndrome; a case-controlled study. BMC Neurol 2011;11:37.
9. Wu KK, Chan SK, Ma TM. Posttraumatic stress, anxiety, and
6. Cleare AJ. The HPA axis and the genesis of chronic fatigue syndrome.
depression in survivors of severe acute respiratory syndrome (SARS).
Trends Endocrinol Metab 2004;15:55-9.
J Trauma Stress 2005;18:39-42.
7. Van der Velden PG, Grievink L, Kleber RJ, et al. Post-disaster mental
10. Dworkin RH, Handlin DS, Richlin DM, Brand L, Vannucci C.
health problems and the utilization of mental health services: a
Unraveling the effects of compensation, litigation, and employment
four-year longitudinal comparative study. Adm Policy Ment Health
on treatment response in chronic pain. Pain 1985;23:49-59.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 27
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
JSM Peiris 裴偉士
Role of dendritic cel s in SARS
HKW Law 羅嘉慧
Key Messages
1. Severe
syndrome coronavirus (SARS-
CoV) entered and replicated
In 2003, the severe acute respiratory syndrome coronavirus (SARS-CoV)
in monocyte-derived dendritic
caused severe, rapidly progressive atypical pneumonia with fever, myalgia,
cells (DCs), but virus
and diarrhoea.1,2 Viruses were detected in the respiratory tract, stool, and urine
replication was incomplete. In
of patients indicating that SARS was a systemic disease. White pulp atrophy
addition, SARS-CoV did not
was noted in the spleen, and lymphoid depletion was noted in lymph nodes.
induce apoptosis or maturation
Lymphopaenia and increasing viral load in the first 10 days of disease strongly
of infected DCs.
suggested an evasion of the immune system by SARS-CoV.3,4
2. SARS-CoV infected DCs
showed low expression of
Based on the function of dendritic cel s (DCs) in immune surveil ance,
antiviral cytokines (IFN-α,
priming, and tolerance, DCs play an important role in the immunopathology of
IFN-β, IFN-γ, and IL-12p40),
SARS. These cel s are professional antigen-presenting cel s linking innate and
moderate up-regulation of
adaptive immunity. Immature DCs reside in the respiratory tract for immune
surveil ance and respond dynamical y to local tissue inflammation in the airways
(TNF-α and IL-6), and
and the distal lung. They express a wide range of c-type lectin receptors and
significant up-regulation of
Tol -like receptors (TLRs) for recognition of conserved pathogen pat erns and
(MIP-1α, RANTES, IP-10, and
induction of subsequent immune responses.
3. SARS-CoV did not modulate
Some TLRs are expressed on the cel surface (TLR-1, TLR-2, TLR-4, TLR-
gene expression of Toll-like
5, TLR-6, TLR-10), whereas others are expressed in intracel ular compartments
receptors (TLR-1 to 10) but
(TLR-3, TLR-7, TLR-8, TLR-9). They are differential y expressed in different
induced significant up-regulation
DC subsets and are modulated in response to a variety of stimuli. Viral proteins
of chemokine receptors (CCR-
bind to TLR-2 or TLR-4; single stranded RNA binds to TLR-7 and TLR-8;
1, CCR-3, CCR-5).
double stranded RNA binds to TLR-3; and viral DNA binds to TLR-9. The
4. SARS-CoV induced high
binding of ligands to TLRs triggers the downstream signal ing pathways that
expression of TRAIL but not
are involved in the cytokine release during primary induction of inflammation
FasL gene expression in DCs.
and secondary activation of anti-inflammatory mechanisms. Cross talks between
5. The characteristic phenotype
TLRs are common, and the formation of TLR heterodimers al ows a higher level
of SARS-CoV infected DCs
of complexity in ligand-receptor binding and subsequent signal ing.
suggested some possible
Migration of DCs from peripheral tissues to lymph nodes is essential
escape and amplification of
for antigen presentation and triggering of adaptive immune responses. The
immunopathology in SARS.
trafficking of DCs is regulated by chemokines in their microenvironment and
their expression of chemokine receptors (CCRs). Differential expressions of
CCRs are observed during DC maturation, and some viruses (such as herpes
Hong Kong Med J 2012;18(Suppl 3):S28-30
simplex virus) can block CCR expressions on DCs to alter their migratory
The University of Hong Kong:
Department of Paediatrics and Adolescent
Chemokines can be classified as homeostatic (constitutively expressed)
Department of Microbiology
or inflammatory (induced/augmented) according to their immune functions.
Respiratory viruses commonly induce inflammatory chemokines (such as MIP-
1α/CCL3, RANTES/CCL-5, IP-10/CXCL10, and MCP-1/CCL2) in local tissues
RFCID project number: 03040772
and DCs. There are redundancies in the interactions between chemokines and
Principal applicant and corresponding author:
CCRs, as many different ligands bind the same receptor and many receptors bind
the same ligand. For example, RANTES binds to CCR-1, CCR-3 and CCR-5,
Department of Paediatrics and Adolescent
whereas MIP-1α binds to CCR-1 and CCR-5.
Medicine, Queen Mary Hospital, Li Ka Shing
Faculty of Medicine, The University of Hong
Kong, Pokfulam, Hong Kong SAR, China
Death receptors and their ligands also play important roles in innate and
Tel: (852) 2855 4482
adaptive immune responses by regulating cel death and survival. Wel -
Fax: (852) 2855 1523
characterised death receptor ligands include TNF-α, FasL, and TRAIL/Apo2L.
Several viruses (including measles virus, human immunodeficiency virus,
28 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Role of dendritic cel s in SARS coronavirus infection
cytomegalovirus, and herpes simplex virus) have been
to be substantiated by increasing the sample size
shown to induce TRAIL expression on DCs. These ‘kil er
and comparing the gene expression by real-time
DCs' may be involved in the kil ing of virus-infected cel s
quantitative PCR.
or bystander lymphocytes and natural kil er cel s. Therefore,
we aimed to determine if the expression of death receptor Results
ligands on DCs can also be modulated by SARS-CoV.
As evident by electron microscopy and immunofluorescence
Clinical y, manifestation of SARS was less severe in staining, SARS-CoV could enter both immature and
children than adults. We hypothesised that the developmental mature human monocyte-derived DCs. Viral replication
status of the host immune system may affect the severity of in DCs was suggested by the detection of negative strands
acute respiratory diseases. We compared the effect of SARS- of SARS-CoV RNA. However, there was no increase in
CoV on adult and cord blood DCs. SARS-CoV could enter viral RNA over time. Using cytopathic assays, SARS-CoV
DCs and alter their expression of cytokines, chemokines, was not detected in DCs and cel culture supernatant. This
TLRs, CCRs, and DLRs. There were possible mechanisms confirmed that virus replication was incomplete. SARS-
of immune escape and amplification of immunopathology CoV did not induce apoptosis or maturation of DCs. SARS-
CoV-infected DCs showed low expression of antiviral
cytokines (IFN-α, IFN-β, IFN-γ, and IL-12p40), moderate
up-regulation of proinflammatory cytokines (TNF-α
and IL-6), and significant up-regulation of inflammatory
This study was conducted from August 2005 to July 2007. chemokines (MIP-1α, RANTES, IP-10, and MCP-1).5
We studied the effects of SARS-CoV on human monocyte- SARS-CoV did not modulate Tol -like receptors (TLR-1 to
derived DC maturation, apoptosis, cytokines/chemokines 10) gene expression, but induced significant up-regulation of
expression, receptors expression, and death receptor ligands chemokine receptors (CCR-1, CCR-3, CCR-5). There was
expression by flow cytometry and real time quantitative strong induction of TRAIL but not FasL gene expressions
polymerase chain reaction (PCR).5,6
in SARS-CoV-infected DCs.
Real-time quantitative PCR was used to analyse some Discussion
immune-related genes based on the advantages that:
(1) Less DCs are needed for total RNA extraction (0.25- The role of immune evasion in the severity and
0.5x106 DCs per sample for real-time quantitative immunopathology of SARS has been supported.2-4 In this
PCR versus 2-5x106 DCs per sample for microarray study, DCs, which are the key antigen-presenting cel s,
played crucial roles in anti-viral immune responses and
(2) Point 1 above translated to the requirement of less may have involved in some immune escape mechanisms
SARS-CoV for infection. This is important for the specific for SARS-CoV (Table). Particularly, up-
researchers' safety when performing the experiments.
regulation of chemokines and death receptor ligands may
(3) Even with the microarray data, the findings need have contributed to infiltration of cel s into the lungs
Table. Possible mechanism of immune evasion in SARS patients
Observations from this study5,6
Possible mechanism of immune
Reported pathology in SARS
SARS-CoV can enter DCs
Use DCs as vehicle or ‘Trojan
Dissemination of virus to multiple
Viral replication
SARS-CoV replication is incomplete -
Dendritic cell (DC) survival
SARS-CoV did not induce DCs
SARS-CoV did not induce
Escape from adaptive immune
Low antibody production in the first
response; induction of regulatory
DC and regulatory T cells
Anti-viral cytokines
Low interferons and IL-12
Block anti-viral responses
Low antibody production in the first
Proinflammatory cytokines Moderate expression of TNF-α and -
Inflammatory chemokines
MIP-1α, RANTES, IP-10, and Increased cell trafficking and DC
mononuclear inflammatory cell
infiltration in lungs
Toll-like receptors
Chemokine receptors
CCR-1 & CCR-5; CCR-3; no Increase DC trafficking; suppress
Reduced immune responses
activated T cells or induce
regulatory T cells
Death receptor ligands
Low FasL; strongly up-regulated
Killing cells at the site of infection
Lymphopaenia; white pulp atrophy
and in lymphoid organs
in spleen and lymphoid depletion in
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 29
and lymphopaenia, respectively. Further studies into the Conclusions
mechanisms of newly emerged viruses to evade the innate
immune responses are necessary.
Dendritic cel s played an important role in the pathogenesis
of SARS. The lack of antiviral cytokine response, intense
There was significant induction of RANTES and its chemokine up-regulation, induction of CCR expression
expression of corresponding receptors CCR-1, CCR-3, and and strong expression of TRAIL observed in SARS-CoV-
CCR-5 mRNA in SARS-CoV-infected DCs. Our previous infected DCs suggested possible mechanisms of immune
gene association study has shown a higher death rate in escape and amplification of immunopathology in SARS.3
SARS patients who have inherited the high-production
gene al ele of RANTES.7 Further investigations into the Acknowledgements
therapeutic strategies that can reduce RANTES production
are warranted.
This study was supported by the Research Fund for the
Control of Infectious Diseases, Food and Health Bureau,
The up-regulation of TRAIL gene expression in both Hong Kong SAR Government (#03040772) as wel as
adult and cord blood DCs after SARS-CoV infection by the Outstanding Researcher Awards and by the Public
represented a kil er DC phenotype. This up-regulation Health Research Grant (AI95357) from the National
is similar to our observation in macrophages infected by Institute of Al ergy and Infectious Diseases, USA.
avian influenza virus. Further investigation is needed to
confirm the cytotoxic function of SARS-CoV-infected DCs References
on immune cel s, and to help design therapeutic strategies
that reduce TRAIL gene expression, neutralise TRAIL, 1. Peiris JS, Lai ST, Poon LL, et al. Coronavirus as a possible cause of
or block signal ing of TRAIL receptors, so as to reduce
severe acute respiratory syndrome. Lancet 2003;361:1319-25.
2. Guo Y, Korteweg C, McNutt MA, Gu J. Pathogenetic mechanisms of
severe acute respiratory syndrome. Virus Res 2008;133:4-12.
3. Frieman M, Heise M, Baric R. SARS coronavirus and innate
Comparing adult and cord blood DCs, both the
immunity. Virus Res 2008;133:101-12.
basal and SAR-CoV-induced gene expression levels of 4. Chen J, Subbarao K. The immunobiology of SARS. Annu Rev
chemokines and CCR genes were significantly higher in
the lat er. Based on the function of chemokines on cell 5. Law HK, Cheung CY, Ng HY, et al. Chemokine up-regulation in
trafficking, more severe infiltration of cel s into the lungs
SARS-coronavirus-infected, monocyte-derived human dendritic
cells. Blood 2005;106:2366-74.
was expected in children. On the contrary, SARS was less 6. Law HK, Cheung CY, Sia SF, Chan YO, Peiris JS, Lau YL. Toll-like
severe in children than adults. The age-dependency of SARS
receptors, chemokine receptors and death receptor ligands responses
severity merits further studies to elucidate the underlying
in SARS coronavirus infected human monocyte derived dendritic
mechanisms. As the information on the chemokine and
cells. BMC Immunol 2009;10:35.
CCR expression and function in children is scanty, further 7. Ng MW, Zhou G, Chong WP, et al. The association of RANTES
polymorphism with severe acute respiratory syndrome in Hong Kong
studies are warranted.
and Beijing Chinese. BMC Infect Dis 2007;7:50.
30 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
BMY Cheung 張文勇
LS Chan 陳龍生
Detection of body temperature with
infrared thermography: accuracy in
CR Kumana 顧崇仁
detection of fever
Key Messages
1. Infrared thermography (IRT)
for detecting body temperature
is less accurate in women,
Since the outbreak of severe acute respiratory syndrome, infrared thermography
elderly people, and those with
(IRT) systems have been deployed at the airport and border crossings in Hong
Kong for screening travel ers. However, its use to identify people with elevated
body temperature is limited. In a pilot study of 176 subjects,1 temperatures
measured by IRT might be used as a proxy for core temperature, but they are
affected by a variety of factors, such as the part of the face measured. We aimed
temperatures obtained from
to investigate the effectiveness of IRT to identify people with fever.
frontal and lateral of the face,
and the forehead.
3. Among the three areas, the
forehead IRT temperature
This study was conducted from September 2005 to August 2006. The protocol
showed the largest discrepancy
was approved by the Institutional Review Board of the Hong Kong West
and poorest correlation with the
Cluster of hospitals. Unselected patients at ending the accident and emergency
core temperature.
department of the Queen Mary Hospital were invited to participate. Patients on
4. If IRT is used, the lateral
stretchers or needing immediate emergency treatment were excluded. Verbal
maximum temperature of the
informed consent was obtained from each subject.
face should be used. A cut-off
temperature of 36ºC gives 77%
The core temperature was defined as either the oral or aural temperature,
sensitivity and 74% specificity.
or whichever was higher if both were available. At ports and border crossings,
5. Owing to its weak correlation
the maximum IRT temperatures obtained from the frontal (Areamax) or lateral
with the core temperature, IRT
(Latmax) of the face or the forehead temperature were used as proxies for the
should not replace direct body
core temperature. Ambient temperature, barometric pressure, and humidity were
temperature measurement in
also recorded. The degree of clothing and the time of measurement were noted.
For the study of the effect of distance on IRT readings, temperatures of 31
healthy (afebrile) volunteers were measured in a control ed laboratory set ing
with the subjects standing at 1, 2, 3, 4 and 5 m from the IRT camera.
The software program ThermaCAM Researcher was used to extract from
the IRT temperatures of designated parts of the face. Data analysis was stratified
by age and gender. Pearson correlation coefficients between IRT temperatures
Hong Kong Med J 2012;18(Suppl 3):S31-4
and oral/tympanic temperature were determined. The 95% confidence limits
of agreement of IRT measurements with the reference method were calculated
The University of Hong Kong:
according to the method of Bland and Altman.2 The standard error of the 95%
Department of Medicine
limit of agreement is approximately √(3s2/n), where s is the standard deviation of
BMY Cheung, CR Kumana
the differences between measurements by the two methods, and n is the sample
Department of Earth Sciences
size.2 The receiver operator characteristics were determined by plot ing the
Department of Statistics and Actuarial
sensitivity against 1-specificity. The sensitivity, specificity, false-positive, and
false-negative rates of IRT were calculated. Likelihood ratios, which describe
the odds of get ing a positive or negative test result, were calculated from the
RFCID project number: 03040232
sensitivity and specificity.
Principal Investigator and corresponding author:
Prof Bernard MY Cheung
Department of Medicine, Queen Mary
Hospital, Hong Kong SAR, China
A total of 747 men and 770 women consented to participate; 215 of them had
Tel: (852) 2255 4347
a core temperature of ≥37.5ºC and were considered to have fever. The forehead
Fax: (852) 2818 6474
IRT temperature showed the largest discrepancy from the core temperature and
Email: [email protected]
was on average 3.1ºC lower. The Latmax yielded the best correlation with the
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 31
core temperature (r=0.441), whereas the forehead IRT years). The best correlation of IRT temperatures with
temperature yielded the poorest correlation (r=0.361) core temperature was seen in children (aged 3-18 years),
fol owed by infants (aged 1-2 years). Male subjects showed
bet er correlation between IRT and core temperatures. The
In al subgroups examined, forehead IRT temperature respective correlation coefficients for the three variables of
was consistently lower than Latmax or Areamax (Fig 1). The Areamax, Latmax, and Forehead were 0.496, 0.5, and 0.404
difference between core and IRT temperature was greatest for males, and 0.369, 0.385, and 0.323 for females (Table
in febrile subjects; the forehead IRT temperature was on 1). A bet er correlation was observed in subjects with a core
average 3.0ºC and 3.7ºC lower than the core temperature in temperature of ≥37.5ºC. For subjects with a normal body
afebrile and febrile subjects, respectively (Fig 1).
temperature, the correlation coefficients between the IRT
and core temperatures tended to be <0.25.
In the Bland-Altman plots of the difference between the
IRT and core temperatures against the mean of the IRT and Ambient temperature had a minor effect on IRT values.
core temperature, IRT temperatures were on average lower Each 1ºC change in ambient temperature changed the IRT
than the core temperature. The difference between IRT and values by 0.196ºC on average.
core temperatures increased as core temperature decreased
The sensitivity, specificity, type-I error, and type-II error
at different IRT temperatures are tabulated in Table 2. At
The subjects were divided into nine age groups (1- 36ºC, the positive and negative likelihood ratios were 3.97
2, 3-6, 7-10, 11-19, 20-29, 30-39, 40-49, 50-65, 66-100 and 0.39 for the Latmax, respectively.
Table 1. Mean infrared thermographic (IRT) temperatures for the frontal (Areamax) and lateral (Latmax) of the face and the
forehead, and correlation coefficients (r) between IRT and core temperatures
Forehead (n=1509)
Mean±SD IRT temperature (ºC)
Mean±SD difference from core temperature (ºC)
Mean±SE lower limit of agreement
Mean±SE upper limit of agreement
r for males
r for females
20-29 30-39 40-49 50-65 66-100 Normal Febrile Normal- Normal- Febrile- Febrile-
years years years years years years years years years
Fig 1. Mean and standard deviation of core and infrared thermography temperatures in different subgroups
32 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Detection of body temperature with infrared thermography
Mean core & IRT temperatures (°C)
Mean core & IRT temperatures (°C)
Mean core & IRT temperatures (°C)
Fig 2. Bland-Altman plots of the difference between core and infrared thermography (IRT) temperatures of the frontal (Areamax)
or lateral (Latmax) of the face or the forehead against the means of core and IRT temperatures
Table 2. Sensitivity and specificity of maximum frontal and lateral infrared thermographic (IRT) temperatures
Cut-off temperature
Maximum frontal IRT temperature
Type-II error, β
False negative rate
False positive rate
Maximum lateral IRT temperature
Type-II error, β
False negative rate
False positive rate
* Total percentage of subjects tested positive
Distance between subject and IRT had a significant The Bland-Altman analysis showed that IRT
effect on IRT readings; IRT temperature decreased linearly temperatures were lower than the core temperature,
with distance (p=0.001). Using 1 m as the reference, the IRT especial y when the core temperature was low. This finding
temperature was 0.35ºC lower at 2 m and 1.1ºC lower at 5 may be useful as it reduces the number of people with a
m. The IRT temperature decreased on average by 0.26ºC normal core temperature being mistaken for having fever.
per meter of distance.
The use of forehead IRT temperature as a proxy for
the body temperature is questionable.6 The forehead IRT
temperature was lowest among the three IRT temperatures
The correlation of IRT temperatures with the core of the face. Its correlation with the core temperature was
temperature was significant but weak (r<0.45). Gender, also lowest. Based on the forehead IRT readings, if 37ºC
age, and core temperature influenced the accuracy of IRT was used as the cut-off temperature for screening, the
temperature as a proxy for body temperature. Females sensitivity was exceedingly low (4%). Reducing the cut-off
showed a poorer correlation between IRT and core temperature to 36ºC and 35ºC increased the sensitivity to
temperatures. It is not possible to rule out if this was due 25% and 52%, respectively. To achieve a sensitivity of about
to cosmetics, as such data were only available on three 79%, the cut-off temperature should be lowered to 34ºC.
This, however, would yield a specificity of 55% and a false
positive rate of 88% (88% of those tested positive would
The IRT system seems more accurate in younger age actual y be afebrile). This would require an unacceptably
groups, especial y children and teenagers.3-5 The core high percentage (47.8%) of subjects to be retested. Thus,
temperatures were higher in children than adults, perhaps the forehead IRT temperatures are not effective in screening
because children with fever were more likely to at end passengers with fever. This casts doubt on the efficacy of
hospital. The core temperatures in the elderly were lower, using a single-point IRT probe to detect passengers with
and their febrile response to infection could be at enuated.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 33
When the maximum frontal IRT temperature was used the forehead IRT temperature differed substantial y from the
as the screening temperature, a cut-off temperature of 36ºC core temperature, and the maximum lateral IRT temperature
would yield a sensitivity of 68% and would result in 22.4% should be used. The reading should also be taken at a
of al subjects to fail the screening. This is much bet er than defined distance from the camera. Overal the sensitivity of
the forehead IRT temperature in terms of sensitivity and IRT in detecting fever is low unless the cut-off temperature
retesting rate. Reducing the cut-off temperature to 35.5ºC is low. When the risk of an epidemic is high and high
would yield a sensitivity of 79% and a specificity of 60%. sensitivity is required, a low cut-off temperature (≤35.5ºC)
However, 86% of those tested positive would actual y be should be chosen, although a large number of people will
afebrile and the percentage of subjects failing the screening require a confirmatory temperature measurement. As IRT is
would increase to 51%.
relatively less accurate on women and older people, more
sampling for aural measurement should be done on these
When the maximum lateral IRT temperature was used individuals.
as the screening temperature, the same cut-off temperature
of 36ºC would yield a sensitivity of 77%, a specificity of Acknowledgements
74%, and a false negative rate of 23%. This would be a
reasonable set ing in terms of sensitivity and false negative This study was supported by the Research Fund for the
rate. However, it would require 29.4% of the subjects to Control of Infectious Diseases, Food and Health Bureau,
be retested. If the percentage of subjects requiring retesting Hong Kong SAR Government (#03040232). We thank Ms
is a constraining factor, raising the cut-off temperature to Jessica Lo (research nurse) and Ms Maggie Chan (research
36.5ºC would reduce the percentage of subjects failing assistant/data analysis).
the screening to 13.5%. However, the sensitivity would
be reduced to 61% and the false negative rate increased to References
39%. This may be unacceptable during an epidemic.
1. Chan LS, Cheung GT, Lauder IJ, Kumana CR, Lauder IJ. Screening
for fever by remote-sensing infrared thermographic camera. J Travel
The distance between the IRT camera and the subject
Med 2004;11:273-9.
is a limiting factor on the efficiency. Although the camera 2. Bland JM, Altman DG. Statistical methods for assessing agreement
can be calibrated for different distances, it is impractical
between two methods of clinical measurement. Lancet 1986;1:307-
at border crossings and airports to do so. One particular
3. Falzon A, Grech V, Caruana B, Magro A, Attard-Montalto S.
mode of operation compares the maximum detected
How reliable is axillary temperature measurement? Acta Paediatr
temperature of travel ers passing in front of the camera
with the temperature inside a control box kept at a constant 4. Craig JV, Lancaster GA, Taylor S, Williamson PR, Smyth RL.
temperature. Errors can arise if the subject and the control
Infrared ear thermometry compared with rectal thermometry in
box are at different distances from the camera.
children: a systematic review. Lancet 2002;360:603-9.
5. Ng DK, Chan CH, Lee RS, Leung LC. Non-contact infrared
thermometry temperature measurement for screening fever in
children. Ann Trop Paediatr 2005;25:267-75.
6. Liu CC, Chang RE, Chang WC. Limitations of forehead infrared
For the application of IRT in screening for travel ers with
body temperature detection for fever screening for severe acute
respiratory syndrome. Infect Control Hosp Epidemiol 2004;25:1109-
elevated body temperature at airports and border crossings,
34 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
CW Yip 葉志偉
Characterisation of animal angiotensin-
converting enzyme 2 receptors and
use of pseudotyped virus to correlate
FCC Leung 梁志清
receptor binding with susceptibility of
Key Messages
1. Comprehensive surveillance
of civets, mice, cats, Golden
Syrian hamsters, and horseshoe
bats is suggested when SARS
or SARS-like CoVs re-emerge
Civets (Paguma larvata) and raccoon dogs (Nyctereutes procyonoides) were
in the human population in the
thought to be the direct zoonotic sources of the severe acute respiratory syndrome
(SARS) epidemic in 2003, because the coronaviruses (CoVs) isolated from these
2. Rabbits and horseshoe bats are
mammals were almost identical to the human SARS-CoV.1 However, these
animal carriers of SARS-CoV.
mammals might not be the natural reservoir of SARS-CoV owing to the lack
3. Investigation of the genetic
of widespread infections. A diverse group of CoVs were identified in various
diversity of CoV in two bat
species of horseshoe bats, which were thus proposed to be the natural reservoir
species (Rhinolophus sinicus
of SARS-CoV.
and Rhinolophus pearsonii)
should provide insights into
In experimental infection, a broad range of animals was demonstrated to
the direct ancestor of human
support in vivo replication of SARS-CoV to different extents. Some of these
species showed observable pathological signs after inoculation, whereas others
showed rapid viral clearance. Based on their ability to support SARS-CoV
replication, they may have potential roles in the transmission of SARS-CoV.
Susceptibility of host cel s to CoVs is mainly determined by spike (S) protein–
induced receptor binding and internalisation. Angiotensin I-converting enzyme
2 (ACE2) is a functional receptor for SARS-CoV, acting as a major determinant
that restricts the tropism and host range.2 In particular, the differences among the
susceptibility of humans, mice, and rats to SARS-CoV have been correlated to
the differential efficiency of interaction between their ACE2 and S protein.3
This study was conducted from January 2007 to December 2008. The ACE2s of
15 different species were prepared. Bagg Albino mouse, Dunkin-Hartley guinea
pig, Sprague-Dawley rat, and New Zealand White rabbit were obtained from the
Laboratory Animal Unit of the University of Hong Kong. Common domestic cat
(Felis domesticus), dog (Canis lupus familiaris), pig (Sus scrofa domestica), and
chicken (Gal us gal us domesticus) were obtained from the Agriculture, Fisheries
Hong Kong Med J 2012;18(Suppl 3):S35-8
and Conservation Department of Hong Kong. Tissues from the smal intestines
of these animals were harvested after terminal anaesthetisation. Fresh small
School of Biological Sciences, The
intestine tissues of the Chinese rufous horseshoe bat (Rhinolophus sinicus) and
University of Hong Kong, Hong Kong SAR,
Japanese house bat (Pipistrel us abramus) were provided by Dr Susanna PK Lau
KKB Li, CW Yip, CC Hon, CY Lam, F Zeng,
from the Department of Microbiology of the University of Hong Kong. Fresh
smal intestine tissues of masked palm civet (Paguma larvata), Golden Syrian
hamster (Mesocricetus auratus), Russian dwarf hamster (Phodopus campbel i),
RFCID project number: 06060672
and long-tailed chinchil a (Chinchil a lanigera) were provided by Prof JD Chen
Principal applicant and corresponding author:
from the South China Agricultural University in Guangzhou, China. Human
Prof Frederick Chi-Ching Leung
intestine cDNA was provided from the Department of Medicine, The University
5N-12, Kadoorie Biological Science
of Hong Kong.
Building, The University of Hong Kong,
Pokfulam, Hong Kong SAR, China
Tel: (852) 2299 0825
The ACE2 of these species was expressed on the surface of the AD293
Fax: (852) 2857 4672
cel line, which is non-susceptible to SARS-CoV. ACE2-expressing cel s were
infected by vesicular stomatitis virus (VSV) pseudotyped with the S protein of
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 35
SARS-CoV (VSV-Sh). The relative expression level of Western blot (Fig 1a). The expression level of each ACE2
ACE2 and the relative susceptibility of ACE2 to VSV-Sh was determined by flow cytometry and was adjusted
were determined by flow cytometry.
by modifying the DNA amount in transfection until a
comparable expression level was obtained (Figs 1a &
Ful -length ACE2-coding sequences were cloned into 1b). The surface localisation of the recombinant human
a mammalian expression vector pCI with a C-terminal V5 ACE2 was demonstrated by flow cytometry analysis on the
epitope-6×His (V5H) tag. These plasmids were transfected transfected cel without permeabilisation (Fig 1c).
and expressed in AD293 cel s. Human ACE1 was also
cloned and expressed as a negative control.
Efficiencies of the ACE2s as receptors for VSV-Sh
were compared based on their relative susceptibility, which
After transfection, ACE2-expressing cel s were is defined as the percentage of VSV-Sh infected cel s
harvested and the membrane fraction in 1% Triton X-100 normalised by the percentage of ACE2-expressing cel s
was separated by sodium dodecyl sulfate-polyacrylamide calculated from three independent experiments (Fig 2). The
gel electrophoresis. The relative molecular sizes of the 15 ACE2s were categorised into groups I to IV according
ACE2s were revealed in Western blot using AP-anti-V5 to their relative susceptibility. Group IV was designated
antibody after deglycosylation. The percentage of cel s as the unsusceptible group with relative susceptibilities
expressing ACE2 was quantified using flow cytometry with not significantly higher (P>0.05) than that of the negative
anti-V5–fluorescein isothiocyanate antibody after fixation control, ie human ACE1 (Fig 2). Group I included the
host species of SARS-CoV, human, and civet. Group II
included mouse, Golden Syrian hamster, cat, and Chinese
The ful -length codon-optimised S gene, excluding rufous horseshoe bat, showing comparable (P>0.05)
its cytoplasmic tail (S ) derived from HKU-39849, was relative susceptibilities, but these were substantial y lower
cloned into a mammalian expression vector pCAGGS. than those of the group I species. Group III included all
VSV-Sh carrying a green-fluorescent protein (GFP) gene other species showing relative susceptibilities that were
was prepared using the pCAGGS-S and VSV-ΔG*-G. significantly lower (P<0.05) than those of group II, but
The transfected cel s were infected by an equal infectious significantly higher (P<0.05) than those of group IV.
unit of VSV-Sh after transfection. The percentage of GFP-
positive cel s was determined using flow cytometry.
From the results of the infection assay, four groups of
ACE2s with differentiated susceptibilities were categorised.
The nucleotide sequence similarities of the ACE2s of the Species from the first 2 groups (including human, civet,
15 species towards human and Chinese rufous horseshoe mouse, cat, Golden Syrian hamster, and horseshoe bat)
bat ACE2s are shown in the Table. The ACE2s among the are expected to support the infection of SARS-CoV.
mammalian species were general y conserved with at least These findings correspond with an in vivo infection study,
85% identity.
implying that the ACE2 receptor is one of the determining
factors for in vivo susceptibility that can be extended to
The ACE2 of the 15 species was expressed as other animal studies in the future. Moreover, the potential y
demonstrated by their relative molecular sizes shown in susceptible animal species should be under comprehensive
Table. Nucleotide sequence similarity of various angiotensin I-converting enzyme 2 (ACE2) compared with human and
Rhinolophus sinicus ACE2, respectively
ACE2 (ranked by relative susceptibility
Length of coding
DNA similarity to
DNA similarity to
GenBank Accession
horseshoe bat (R
sinicus) ACE2 (%)
Golden Syrian hamster
Horseshoe bat (Rhinolophus sinicus)
Japanese house bat
Russian dwarf hamster
36 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012

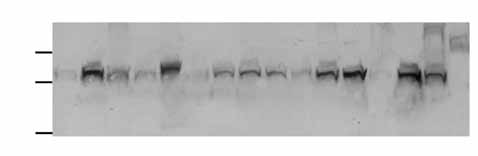
Animal angiotensin-converting enzyme 2 receptors
Japanese house bat
Japanese house bat
Percentage of cels expressing AC
Japanese house bat
Fig 1. Expression of various angiotensin I-converting enzyme 2 (ACE2) in AD293
(a) Membrane fraction of ACE2-expressing cells analysed in Western blot. (b) Percentage of cells expressing various ACE2s detected in
flow cytometry analyses. (c) Cell surface transient expression of human ACE2
Golden Syrian hamster
Japanese house bat
Russian dwarf hamster
Relative susceptibility
Fig 2. Percentage of VSV-Sh infected cells normalised by the percentage of cells expressing the corresponding angiotensin
I-converting enzyme 2 (ACE2) to 100% expression, ie (% of green-fluorescent protein-positive) / (% of ACE2 expression) × 100%
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 37
surveil ance when SARS or SARS-like CoVs appear in the homologies with the human SARS-CoV S protein, and may
human population again.
be the direct progenitor of human SARS-CoV. Although the
S protein of al currently sampled bat SARS-like-CoV in R
Most species investigated were common consumption sinicus is highly divergent from that of human SARS-CoV,
and companion animals that intensively interact with the presence of an uncharacterised lineage in R sinicus is
humans. It is crucial to assess their potential for being possible based on the relatively high genetic diversity of
animal vectors for SARS-CoV transmission. Rodents bat SARS-like-CoV. Our previous study speculated that
have been proposed as a possible vector for SARS-CoV the direct progenitor of human SARS-CoV may exist in
transmission. The in vivo susceptibility of group III animals R pearsoni based on the ORF1 phylogeny.5 Interspecies
(chinchil a, Russian dwarf hamster, dog, and rabbit) has transmission of CoVs between Rhinolophus spp appears
not been investigated. Based on the results, the ACE2s of to be a common process, suggesting the possibility of
these animals did not seem to support entry of VSV-Sh coinfection and thus recombination between bat SARS-
as efficiently as groups I and II species. Nonetheless, the like-CoVs.
relative susceptibility of rabbit ACE2 was significantly
higher than that of the guinea pig, which was found to Acknowledgements
inefficiently support in vivo replication of SARS-CoV.
Thus, SARS-CoV might replicate more efficiently in rabbits This study was supported by the Research Fund for the
than in guinea pigs. The risk that group IV species transmit Control of Infectious Diseases, Food and Health Bureau,
SARS-CoV may be remote, as none of these species has Hong Kong SAR Government (#06060672). We thank
been shown to efficiently shed virus after experimental Mr Chung-tong Shek from the Agriculture, Fisheries and
inculcation. Although further in vivo experiments are Conservation Department of Hong Kong for his support in
needed to confirm such speculations, this study should bat species identification.
provide a bet er scope of investigation for animal vectors
of SARS-CoV, particularly of rabbit and Chinese rufous References
horseshoe bat.
1. Guan Y, Zheng BJ, He YQ, et al. Isolation and characterization of
The relative susceptibility of the ACE2 of R sinicus
viruses related to the SARS coronavirus from animals in southern
China. Science 2003;302:276-8.
was comparable to that of cat, mouse, and Golden Syrian 2. Li W, Moore MJ, Vasilieva N, et al. Angiotensin-converting
hamster, whereas the ACE2 of Japanese house bat (in this
enzyme 2 is a functional receptor for the SARS coronavirus. Nature
study) and Rhinolophus pearsoni (in a previous study4) did
not seem to support the entry of SARS-CoV S-pseudotyped 3. Li W, Greenough TC, Moore MJ, et al. Efficient replication of severe
acute respiratory syndrome coronavirus in mouse cells is limited by
viruses. These findings imply that the susceptibility of
murine angiotensin-converting enzyme 2. J Virol 2004;78:11429-33.
ACE2 towards human SARS-CoV may be species-specific 4. Ren W, Qu X, Li W, et al. Difference in receptor usage between
in bats. Further investigations of the ACE2s of different
severe acute respiratory syndrome (SARS) coronavirus and SARS-
bat species are needed to extend this observation. The
like coronavirus of bat origin. J Virol 2008;82:1899-907.
susceptibility of R sinicus ACE2 towards VSV-Sh implies 5. Hon CC, Lam TY, Shi ZL, et al. Evidence of the recombinant origin
of a bat severe acute respiratory syndrome (SARS)-like coronavirus
the potential existence of a bat SARS-like-CoV, which
and its implications on the direct ancestor of SARS coronavirus. J
may carry an S protein that shares significant structural
38 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
JTF Lau 劉德輝
HY Tsui 徐喜兒
Voluntary counsel ing and testing plus
information distribution to reduce
Key Messages
HIV-related risk behaviours among
1. A randomised controlled trial
was conducted to compare
Hong Kong male cross-border truck
the efficacy of voluntary
counselling and testing (VCT)
drivers: a randomised control ed study
plus information distribution
versus information distribution
alone in 300 Chinese male
cross-border truck drivers.
2. Two months after the
intervention, participants of the
Mobility is a risk factor for the spread of HIV across geographic locations.1-3
VCT intervention group were
Travel ers are more likely to practice HIV-related risk behaviours when they are
more likely to be consistent
away from home4,5 and may become a bridge population transmit ing HIV to
condom users when having
other populations.1-3 It is hence warranted to provide HIV intervention services
sex with female sex workers
to frequent travel ers. Cross-border truck drivers are one of the target groups, as
and non-regular sex partners,
they tend to have HIV-related risk behaviours.6
were more knowledgeable
about HIV, and were less likely
In 2010, there were 4832 reported HIV cases in Hong Kong and about 400
to have contracted a sexually
new cases per year, 29% of which were at ributed to heterosexual transmission,7
transmitted disease in the past
many of which were suspected to be related to cross-border sexual activities.7
2 months, compared to the
Respectively, 9-12% and 11-13% of Hong Kong adult men travel ing to mainland
China had had sex with a female sex worker (FSW) and a female non-regular sex
3. Almost all participants of
partner (NRP) during the most recent trip.8 A high prevalence of unprotected
the intervention group were
sex and sexual y transmit ed diseases have also been reported in this group.8 In
satisfied with the VCT service,
addition, there are 919 reported HIV/AIDS cases per year in Shenzhen in 2010.9
and almost 90% agreed that it
Cross-border HIV prevention needs to be strengthened to keep HIV prevalence
would increase their chance of
low in Hong Kong.
using condoms in the future.
With the advancement of rapid HIV testing tools, voluntary counsel ing and
testing (VCT) becomes an important means of HIV prevention.10 It can be used
for case detection and for reducing risk behaviours.10 Its effectiveness has been
mixed, and there have been few randomised control ed trials.11,12 Evidence-based
HIV interventions are lacking. Evidence-based randomised control ed trials are
important, as is translation of research results into practice. Col aboration with
Hong Kong Med J 2012;18(Suppl 3):S39-41
non-governmental organisations and the Department of Health is necessary for
Centre for Health Behaviours Research,
HIV prevention.
School of Public Health and Primary
Care, Faculty of Medicine, The Chinese
University of Hong Kong
Centre for Medical Anthropology and
This study was conducted from November 2004 to March 2006. During 2005
Behavioral Health, Sun Yat-sen University,
and 2006, a randomised control ed trial was carried out to compare the efficacy
of VCT plus information distribution versus information distribution alone.
RFCID project number: 01030972
With informed consent, more than 2000 cross-border truck drivers were
screened in a cafe (rest area) of the checkpoint while waiting for custom
Principal applicant and corresponding author:
clearance. Of them, 320 were eligible to join the study. They were 18+ years old,
Prof Joseph TF Lau
Centre for Health Behaviours Research,
self-reported to have had sexual intercourse with either a FSW or a NRP (who
School of Public Health and Primary Care,
was not a FSW, spouse, or girlfriend) in mainland China in the past 12 months. A
Faculty of Medicine, The Chinese University
total of 300 participants were randomised into the intervention group (VCT plus
of Hong Kong, 5/F, School of Public Health,
information distribution) or the control group (information distribution alone).
Prince of Wales Hospital, Shatin, NT, Hong
The intervention group was given a 30-45 minute VCT intervention, which
Tel: (852) 2637 6606
included the HIV rapid screening test and pre- and post-test counsel ing. None
Fax: (852) 2645 3098
of the participants tested HIV positive. The primary outcome measures were
Email: [email protected]
consistent (every time) condom use during sexual activity with FSW and NRP
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 39
in mainland China over a 2-month post-intervention period. although the fol ow-up period was short and the sample size
Anonymous surveys were conducted before randomisation was moderate. Further large-scale studies are warranted.
(baseline) and at month 2, using a computer-assisted
interviewing method to reduce bias.8,13 Absolute and relative Acknowledgements
risk reduction statistics and their 95% confidence intervals
were used to assess treatment effects.14
This study was supported by the Research Fund for the
Control of Infectious Diseases, Food and Health Bureau,
Hong Kong SAR Government (#01030972). The authors
thank the participants and those who helped in data
The results have been published in ful in AIDS Care.15 col ection. The results of this study have been published in:
Baseline statistics were not significantly different Lau JT, Tsui HY, Cheng S, Pang M. A randomized control ed
between the intervention and control groups. At baseline, trial to evaluate the relative efficacy of adding voluntary
only about two-thirds of the participants of both groups counseling and testing (VCT) to information dissemination
consistently used condoms during sexual activity with a in reducing HIV-related risk behaviors among Hong Kong
FSW in mainland China in the past 2 months, and about male cross-border truck drivers. AIDS Care 2010;22:17-28.
30% did so with their NRP.15 At month 2, participants of
the intervention group were more likely to be consistent References
condom users when having sex with a FSW and NRP, were
more knowledgeable about HIV, and were less likely to 1. Essuon AD, Simmons DS, Stephens TT, Richter D, Lindley LL,
have contracted sexual y transmit ed diseases in the past 2
Braithwaite RL. Transient populations: linking HIV, migrant workers,
months.15 Almost al participants of the intervention group
and South African male inmates. J Health Care Poor Underserved
were satisfied with the VCT service, and about 90% agreed
that it would increase their chance of using condoms in the 2. Magis-Rodríguez C, Lemp G, Hernandez MT, Sanchez MA, Estrada
F, Bravo-García E. Going North: Mexican migrants and their
vulnerability to HIV. J Acquir Immune Defic Syndr 2009;51(Suppl
3. Ramjee G, Gouws E. Prevalence of HIV among truck drivers visiting
sex workers in KwaZulu-Natal, South Africa. Sex Transm Dis
Our target population was at high risk of HIV/STD infection
4. Hawkes S, Hart GJ, Johnson AM, et al. Risk behaviour and HIV
as the prevalence of consistent condom use was low
prevalence in international travellers. AIDS 1994;8:247-52.
(especial y when having sex with a NRP), and the incidence 5. Egan CE. Sexual behaviours, condom use and factors influencing
of self-reported sexual y transmit ed diseases among the
casual sex among backpackers and other young international
controls and within the 2-month post-intervention period
travelers. Can J Hum Sex 2001;10:41-58.
6. Ho CO, Choy YL. AIDS awareness and sexual behaviors of truck
was quite high. The results of this study were disseminated
drivers in Hong Kong. Proceedings of the Hong Kong AIDS
to HIV workers and funders in Hong Kong, and one non-
Conference. 8-9 November 1996, Hong Kong; 229-34.
governmental organisation successful y applied funding 7. Centre for Health Protection, Department of Health. Press Meeting 1
using our findings and implemented an up-scaled VCT
March 2011 by Dr Wong Ka-hing. Available at http://www.info.gov.
hk/aids/english/new2011/nm02_3.pdf. Accessed 21 November 2011.
8. Lau JT, Tsui HY. HIV/AIDS behavioral surveillance surveys of the
cross-border sex-networker population in Hong Kong from 1997 to
This study exemplifies how public health research can
2001. Sex Transm Dis 2003;30:827-34.
be translated into real intervention programmes. Our role as 9. Shenzhen Center for Disease Control and Prevention. Report on the
academics is to provide feasible, innovative, and evidence-
analysis of the epidemiology of HIV/AIDS in Shenzhen in 2010.
based models, which can be implemented in a sustainable 10. Family Health International (FHI). FHI briefs: meeting the
need: HIV counselling and testing (July 2004). FHI's Institute
manner by health organisations or the government. During
for HIV/AIDS. Available at: http://www.fhi.org/NR/rdonlyres/
the research process, it was important to involve non-
governmental organisations, the truck drivers' associations
FHIBriefsvctshell.pdf. Accessed 7 September 2006.
and their community leaders, the checkpoint officials, 11. The Voluntary HIV-1 Counseling and Testing Efficacy Study Group.
the owner of the cafe (rest area), and the laboratory of
Efficacy of voluntary HIV-1 counselling and testing in individuals
and couples in Kenya, Tanzania, and Trinidad: a randomized trial.
the Department of Health in order to provide diagnostic
Lancet 2000;356:103-12.
services for positively screened results, if any. We used the 12. Landis SE, Earp JL, Koch GG. Impact of HIV testing and counseling
healthy set ing approach16 to access the target group at a
on subsequent sexual behavior. AIDS Educ Prev 1992;4:61-70.
place that they gather and have time to take up the VCT.
13. Lau JT, Thomas J, Liu JL. Mobile phone and interactive computer
interviewing to measure HIV-related risk behaviours: the impacts of
data collection methods on research results. AIDS 2000;14:1277-9.
HIV detection is very important for its treatment and 14. Guyatt G, Rennie D, editors. Users' guides to the medical literature:
control. Some health authorities suggest that HIV antibody
a manual for evidence-based clinical practice. Chicago: AMA Press;
testing should be simplified and the counsel ing component
should be reduced or even removed on the grounds that VCT 15. Lau JT, Tsui HY, Cheng S, Pang M. A randomized controlled trial
to evaluate the relative efficacy of adding voluntary counseling and
is ineffective in changing risk behaviours.17 Our studies
testing (VCT) to information dissemination in reducing HIV-related
showed that VCT is effective in reducing risk behaviours,
risk behaviors among Hong Kong male cross-border truck drivers.
40 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Voluntary counsel ing and testing plus information distribution to reduce HIV-related risk behaviours
AIDS Care 2010;22:17-28.
16. Green LW, Poland B, Rootman I. The settings approach to health
17. Branson BM, Handsfield HH, Lampe MA, et al. Revised
promotion. In: Poland B, Green LW, Rootman I, editors. Setting for
recommendations for HIV testing of adults, adolescents, and pregnant
health promotion: linking theory and practice. Thousands Oaks, CA:
women in health-care settings. MMWR Recomm Rep 2006;55:1-17.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 41
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES
WCW Wong 黃志威
Prevalence and risk factors of
TN Leung 梁子昂
sexual y transmitted infections in
H Lynn 林燧恒
female sex workers in Hong Kong
Key Messages
1. The prevalence of hepatitis
B surface antigen, syphilis,
gonorrhoea, chlamydia, and
Sexual y transmit ed infections (STIs) remain a major public health problem
HIV among the participating
in Hong Kong. Sex workers are reservoirs and vectors for the transmission of
female sex workers (FSW)
STIs in the community. To formulate prevention strategies, the prevalence and
accounted for 8.5%, 1.8%,
risk factors of STIs among asymptomatic female sex workers (FSW) should be
1.8%, 4.6%, and 0.2%,
2. Alcohol consumption, place of
In Hong Kong, STI (including HIV) testing, treatment, and other medical
origin, a history of termination
services are available for free to local residents, but non-Hong Kong residents
of pregnancy, higher education
are charged a minimum fee of HK$1400. These high fees deter many non-local
level, having multiple partners,
and being a non-smoker
FSWs from seeking proper treatment, and may result in the potential spread of
were risk factors of sexually
STIs to their clients and families.1 An outreach wel -women clinic for FSWs in
transmitted infections (STIs)
Hong Kong was established by the non-governmental organisation—Ziteng—in
among asymptomatic FSWs.
February 2004. In the clinic, Pap smears, STI (including HIV) screening, and
3. Inconsistent use of condom
basic physical examinations were provided for free to al FSWs. We aimed to
when having sex with regular
report on the prevalence and risk factors of STIs (including HIV) among FSWs
partners among FSWs may
in Hong Kong.
have a bridging effect in
the spread of STIs to other
population groups.
4. Continue surveillance of STIs
in FSWs in Hong Kong is
This study was conducted from October 2005 to September 2007. A total of
important. A coherent policy
511 FSWs aged 18 to 55 years were recruited in the clinic of Ziteng between
and holistic approach is
December 2005 and April 2007. It coordinated the screening service including
required to control the spread
Pap smears and venipunctures for STI (including HIV) testing, provided
of STIs in the community.
health education and ensured continuity of care through re-tests and fol ow-up
interviews, conducted outreach and screening services at places where FSWs
work. A team of two to three volunteer doctors worked in the clinic to provide
Hong Kong Med J 2012;18(Suppl 3):S42-6
medical counsel ing and care 2 to 3 hours a day, twice monthly.
Department of Community and Family
Medicine, School of Public Health and Primary
The subjects remained anonymous and their identification documents were not
Care, The Chinese University of Hong Kong,
checked to ensure privacy and confidentiality. They had a face-to-face interview
Prince of Wales Hospital
with a doctor or nurse, and HIV pre-test counsel ing and an opportunistic health
education were given. They also underwent a physical examination, Pap smear,
and blood tests for detection of gonorrhoea, chlamydia, hepatitis B, syphilis,
Department of Obstetrics and Gynaecology,
Prince of Wales Hospital
and HIV infections. Demographics (age, place of origin, and marital status),
lifestyle (smoking, drinking, and exercise habits), and sexual behaviour (use of
Department of Biostatistics, School of Public
Health, Fudan University, Shanghai, PRC
condoms, number of sexual partners, and vaginal douching) were recorded using
a multifaceted self-report questionnaire.
Department of Economics, California State
University, Fullerton, CA, USA
After 2 to 4 weeks, the results of these examinations were explained to the
patients. If the results were positive, fol ow-up medical care was arranged and
RFCID project number: 03040172
treatment was given based on the Department of Health's STI management
Principal investigator and corresponding author:
guidelines (except for HIV). Fol ow-up services (prescriptions and referrals)
Department of Family Medicine and Primary
Care, The University of Hong Kong, 3rd Floor,
Ap Lei Chau Clinic, 161 Main Street, Ap Lei
Chau, Hong Kong SAR, China
Tel: (852) 2518 5657
Fax: (852) 2814 7475
A total of 503 FSWs were classified into three groups according to their place of
Email: [email protected]
origin: 97 (19.3%) were local; 361 (71.8%) were new immigrants; and 45 (8.9%)
42 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Sexual y transmit ed infections in female sex workers
were non-local il egal migrants on a temporary visitor visa of the FSWs had worked for <1 year. The average number
(Table 1). Non-local FSWs were younger and less likely of clients per day was 5.0; new immigrant FSWs received
to be smoker, whereas local FSWs were less likely to be most clients per day.
married and more likely to be smokers. New immigrant and
non-local FSWs were more likely to have single child. The Twenty (4.0%) of the FSWs had ≥2 regular sexual
prevalence of STI among these FSWs was 43 (8.5%) for partners (Table 2); 97.5% and 77.0% of the FSWs reported
hepatitis B surface antigens, 9 (1.8%) for syphilis, 9 (1.8%) to have always used condoms when they had vaginal sex
for gonorrhoea, 23 (4.6%) for chlamydia, and 1 (0.2%) for and oral sex with their clients, respectively. However,
HIV infection.
only 23.0% insisted on using condoms when they had sex
with their partners. In addition, 56.1% of them performed
Of these FSWs, 55 (10.9%) worked on the street, 361 regular vaginal douching with over-the-counter medicines
(71.8%) in a single-woman brothel, 81 (16.1%) in a sauna or water. About 89.5% of FSWs had gynaecological
or massage parlour, and 6 (1.2%) in a karaoke club or for an examinations in the past and 70.6% had undergone a
agency (Table 2). The street was the most popular place for cervical smear, with non-local FSWs being significantly
non-local FSWs (91.1%), whereas single-woman brothels less likely to do so. Around 13.1% of FSWs had a history
were the most popular place for locals (72.2% of FSWs of STIs; new immigrant FSWs were least likely to contract
born in HK and 79.8% of new immigrants). About 57.6% STIs.
Table 1. Demographic and family characteristics of female sex workers
No. (%) of female sex workers
Local (born in Hong
immigrants, n=361)
Age group (years)
Primary school or below
Low secondary school
High secondary school
University or above
No. of children in family
Chlamydia infection
* Chi squared test† Chi square computed by Monte Carlo method for non-2x2 table, in which at least one cell has expected cell count of <5‡ Chi squared linear-by-linear association test computed by Monte Carlo method, in which at least one cell has expected cell count of <5
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 43
Table 2. Sexual behaviour and working conditions of female sex workers
No. (%) of female sex workers
Local (born in Hong
immigrants, n=361)
Single woman brothel
Sauna or massage
3 months to <1 year
Average no. of clients per day
No. of sexual partners
Condom use (vaginal sex)
Condom use (oral sex)
Condom use with partner
Knowledge on human papillomavirus and
Human papillomavirus vaccine
Income of one day
Previous gynaecological examination
Previous Pap smear
Previous sexually transmitted infection
Previous sexually transmitted infection in those
with previous gynaecological examination
Age of first sex (years)
* Chi squared test† Chi square computed by Monte Carlo method for non-2x2 table, in which at least one cell has expected cell count of <5‡ Chi squared linear-by-linear association test computed by Monte Carlo method, in which at least one cell has expected cell count of <5§ Kruskal Wallis test
Regarding risk factors for STIs, syphilis and gonorrhoea of education had a higher risk of contracting chlamydia.
were more common in non-local FSWs (Table 3). The Previous termination of pregnancy was associated with
FSWs who had ≥2 sexual partners were more likely to have contracting syphilis. Hepatitis B infection was associated
gonorrhoea infection, whereas those who had a higher level with being a non-smoker.
44 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Sexual y transmit ed infections in female sex workers
Table 3. Demographic features significantly associated with
Hygiene Service from 1999 to 2000,2 the rate of chlamydia
specific sexually transmitted infections
was significantly lower in our cohorts (41.7% vs 4.6%
Demographic feature
Sexually transmitted
had non-specific urethritis). The rates of gonorrhoea were
consistent (1.5% vs 1.8%), but those of HIV (0.1% vs 0.2%)
and syphilis (0.1% vs 1.8%) were significantly higher in
our sample. These increases could be due to the time gap
between the two studies. Currently, hepatitis B and HIV
are the only STIs that have to be reported according to the
Quarantine and Prevention of Disease Ordinance. It is of
public health interest to consider the inclusion of other STIs
or to conduct a continuous serial surveil ance other than the
sentinel surveil ance.
No. of sexual partners
Condom use with regular sexual partners was infrequent
(23.0%) among FSWs. This was consistent with a recent
systematic review reporting a proportion of 8% to 30%.3
The concept of a partner appeared rather unclear in this
group. It could refer to a husband in a formal marriage,
Local (new immigrants)
co-inhabitants, frequent customers, or whoever they feel
Chlamydia Infection
at ached to. In our sample, 4% of FSWs reported having
≥2 partners, but this figure may be an under-estimate. This
may have a bridging effect for the spread of STI to other
population groups, especial y clients and their families.
University or above
* Fisher's exact test for 2x2 table
Alcohol consumption and multiple partners are known
† Chi squared linear-by-linear association test computed by Monte Carlo
method, in which at least one cell has expected cell count of <5
risk factors. Unexpectedly, higher education level and not
‡ Chi square computed by Monte Carlo method for non-2x2 table, in which
smoking were correlates of chlamydia and Hepatitis B
at least one cell has expected cell count of <5
infections, respectively. These may be due to an unrealistic
optimism regarding their physical wel being, and thus less
concern about adopting various health protection measures.
More research is necessary to explore this argument.
Medical professionals and public health specialists
Of 503 FSWs, 71.8% were from single-woman brothels. should address these misconceptions through education and
Only 19.3% were born in Hong Kong, whereas most street prevention activities, which should focus on the promotion
FSWs were non-local il egal migrants. They received an of consistent condom use and awareness of the risks of
average of five clients per day; of whom 97.5% claimed STIs. Nonetheless, education alone may not be sufficient,
to have used condoms consistently. Nonetheless, condom as FSWs already have good awareness and appropriate
use with regular sexual partners remained low at 23.0%. at itudes towards protective behaviours, but have difficulty
Hepatitis B surface antigen, syphilis, gonorrhoea, translating them into action. Therefore, the World Health
chlamydia, and HIV infections were present in 8.5%, 1.8%, Organization's holistic approach to sexual health (the
1.8%, 4.6%, and 0.2% of our sample, respectively. The risk integration of the somatic, emotional, intel ectual, and social
factors for STIs among asymptomatic FSWs were place aspects of sexual wel -being in ways that are positively
of origin, a history of termination of pregnancy, higher enriching and that enhance personality, communication,
education level, having multiple partners, and being a non- and love) should be adopted.4
One limitation of this study was that our sample included
only those who were wil ing to engage with Ziteng and was This study was supported by the Research Fund for the
not representative of al FSWs in Hong Kong. This group of Control of Infectious Diseases, Food and Health Bureau,
FSWs was no doubt more health conscious; the actual STI Hong Kong SAR Government (#03040172). Special
rate in the general population FSWs is likely to be higher. gratitude is extended to the Chinese University of Hong
Moreover, this cross-sectional study was unable to identify Kong for its support. We thank Prof Sian Griffiths,
the specific timing and relationships of our participants' Director of the School of Public Health and Primary
responses and their STIs. Causal relationships between Care, for providing us the opportunity and freedom to
STIs and various risk factors should be inferred careful y.
conduct research in this population. We also thank the non-
governmental organisation—Ziteng, the volunteer doctors,
In comparison with FSWs who had at ended the Social and the sex workers for participation.
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 45
Results of this study have been published in: Wong WC,
medical needs of sex workers in a China/Myanmar border town.
Yim YL, Lynn H. Sexual y transmit ed infections among
AIDS Patient Care STDS 2003;17:417-22.
female sex workers in Hong Kong: the role of migration 2. Chan MK, Ho KM, Lo KK. A behaviour sentinel surveillance for
status. J Travel Med 2011;18:1-7.
female sex workers in the Social Hygiene Service in Hong Kong
(1999-2000). Int J STD AIDS 2002;13:815-20.
3. Wong WC, Wun YT. The health of female sex workers in Hong
References
Kong: do we care? Hong Kong Med J 2003;9:471-3.
4. World Health Organization. Working definition. Available at
1. Wong WC, Yilin W. A qualitative study on HIV risk behaviors and
html#3.2002. Accessed on 14 Dec 2005.
46 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
AUTHOR INDEX
Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012 47
The reports contained in this publication are for reference only and should not be regarded as a substitute for
professional advice. The Government shall not be liable for any loss or damage, howsoever caused, arising from any
information contained in these reports. The Government shall not be liable for any inaccuracies, incompleteness,
omissions, mistakes or errors in these reports, or for any loss or damage arising from information presented herein.
The opinions, findings, conclusions and recommendations expressed in this report are those of the authors of these
reports, and do not necessarily reflect the views of the Government. Nothing herein shall affect the copyright and other
intellectual property rights in the information and material contained in these reports. All intellectual property rights
and any other rights, if any, in relation to the contents of these reports are hereby reserved. The material herein may
be reproduced for personal use but may not be reproduced or distributed for commercial purposes or any other
exploitation without the prior written consent of the Government. Nothing contained in these reports shall constitute
any of the authors of these reports an employer, employee, servant, agent or partner of the Government.
Published by the Hong Kong Academy of Medicine Press for the Government of the Hong Kong Special Administrative
Region. The opinions expressed in the Hong Kong Medical Journal and its supplements are those of the authors and
do not reflect the official policies of the Hong Kong Academy of Medicine, the Hong Kong Medical Association, the
institutions to which the authors are affiliated, or those of the publisher.
48 Hong Kong Med J Vol 18 No 4 Supplement 3 August 2012
Source: https://rfs1.fhb.gov.hk/images/HKMJ/HKMJ_Vol18_No4_Supple3_Aug2012.pdf
14. Ein weitreichendes Spiel Als Elfriede noch ein kleines Mädchen ist, fällt ihr Va- ter im Krieg. In der Folge verbringt sie eine bescheidene Kindheit im Wiener Arbeiterbezirk Favoriten. Gemeinsam mit ihren fünf Geschwistern teilt sie sich ein Zimmer. Wenn Elfriede aber ausgeht, studiert sie die Kleidung der höhe-ren Gesellschaft, ihre Umgangsformen, ihr Selbstvertrauen. Denn sie hat sich früh geschworen: Sie muss hinaus aus ih-rem Milieu, hoch hinaus. In der ersten großen Liebe glaubt sie, einen Weg hinaus zu erkennen: die Ehe. Das Glück währt nicht lange. Nach der Geburt der gemeinsamen Tochter lässt sich ihr Mann scheiden. Seither bestimmen Elfriedes weite-ren Weg ihr absoluter Willen zu Wohlstand sowie ein beken-nender Hass auf Männer.
Circular 57 pinfish, eel, sea trout, tilapia, sturgeon, and striped bass (Inglis et al. 1993). Strep has also been Streptococcus is a genus of bacteria containing isolated from a variety of ornamental fish, including some species that cause serious diseases in a rainbow sharks, red-tailed black sharks, rosey number of different hosts. A major identifying

