Ihb.net



t i o n a l H C
o s p i t a l o U
f B a h r a i Sn W.L.L
Vol. 2 Issue No. 18
The Second Physician Attribute:
Medical and Clinical Knowledge
Medicine changes rapidly. Clinical practice and standards advance fast. We in the Hospital place great
importance to the management of change. We al think that proper management of change is the
one thing we must do al the time. For a physician to stay up-to-date he must adopt a pattern of life
which enhances his knowledge and improves his skil s. A physician who spends much of his spare
hours watching television cannot be up-to-date, and this wil eventual y show. Being knowledgeable in Medicine
and being a competent medical practitioner cal s for extra effort on the part of the physician to hone his skil s
and to enhance his knowledge. Proctoring for this attribute is looking for the practitioner to demonstrate not only
knowledge, but know-how of established, up-to-date protocols, policies, procedures, and the best of evidence-
based clinical practices. The attributes of the new physician must include his knowledge and use of evidence-
based practices and guidelines. These guidelines emulate and fol ow the protocols from the best international y
recognized medical centers of excel ence. The physician we want to work with must be versed in and familiar with
the guidelines of these best practices which are reached by evolving biomedical, clinical, therapeutics and social
sciences. Our physician must be able to demonstrate his confidence in his knowledge. The proctor is looking for
the ability of the newly-appointed physician to apply his skil and his knowledge to patient care and the education
of others. The proctored Practitioner must be able to demonstrate service quality. He is committed to quality;
another pil ar on which the Hospital stands. The three pil ar of our practice in the International Hospital of Bahrain
are SPS (Superior Patient Service), CQI (Continuous Quality Improvement) and constant innovation: with the ability
to meet the changing needs of patients, col eagues and the Hospital. These three pil ars of quality and quests
for enhancing quality of the Hospital Medical Staff are not theoretical, but part of our culture. The proctored
physician must be seen to participate in superior patient service. He must be wil ing to adapt to innovation and
improvement. He must be seen to contribute to and be part of the path to excel ence and improvement. He
must show that he can adapt and make it his way or his new way of life. Continuous quality improvement has a
momentum in the Hospital, and we evaluate the reaction and interaction of the new physician to this. We are
looking at his enthusiasm and absorption in the quest of improvement of everything we do.
In the second attribute we are looking for a knowledgeable, scientific clinician whose practice is evidence-
Vol 2 Issue No. 18May 2012
Editor-in-Chief: Dr. Faysal S. Zeerah
Editors:• Dr. Dilip Malhotra
• Dr. Nader Albert Ghobrial• Dr. Mona Issa Farrag• Dr. Meena Khalatkar
• Dr. Ivo Fernandez
Designer: Mildred Belen
Published by: International Hospital of Bahrain, W.L.L.
PO Box 1084, Manama
Kingdom of Bahrain.
Switchboard: +973 1759 8222Email: [email protected]
Website: www.ihb.net
For Appointments,
please call +973.17598200
How are we doing?
We need your feedback for continuous
improvement and want to hear from you. We welcome a letter or email detailing your patient care experience. Excellent,
good, bad, indifferent, let us know how we are doing!
We constantly strive to offer the best care and customer service and appreciate your feedback.
FOCUS is published as a service to the
community. Although every effort has been made to ensure the accuracy of information on this publication, the
International Hospital of Bahrain cannot be held liable for any errors or omissions contained in this publication. Readers
are advised to seek specialist advice before acting on information contained in this publication which is provided for
general use and may not be appropriate
for the reader's particular circumstances.



Obesity in Children
Childhood obesity is a serious medical condition
that affects children and adolescents. It occurs
when a child is well above the normal weight for
his or her age and height.
Not al children carrying extra kilos are overweight or obese. Some
children have larger than average body frames and carry different
amounts of body fat at the various stages of development. Your
child's doctor can help you figure out if the child's weight could
pose health problems by calculating the child's body mass index
(BMI). The BMI indicates if the child is overweight for his or her age
and height. Using a growth chart, your doctor determines your child's
percentile, meaning how your child compares with other children
of the same sex and age. For example, you might be told that your
child is in the 80th percentile. This means that compared with other
children of the same sex and age, 80 percent have a lower BMI.
• BMI-for-age between 85th and 94th percentiles — overweight
• BMI-for-age 95th percentile or above — obesity
Childhood obesity can have the fol owing complications:
• Type 2 diabetes. Type 2 diabetes in children is a chronic
condition that affects the way your child's body metabolizes
glucose (sugar). Type 2 diabetes is caused in part by poor
diet and can often be reversed by eating healthier foods and
• Metabolic syndrome. Metabolic syndrome isn't a disease itself,
but a cluster of conditions like high blood pressure, high blood
sugar, high cholesterol and excess abdominal fat that can put the
child at risk of developing heart disease, diabetes or other health
problems.These factors can contribute to the buildup of plaques
in the arteries. These plaques can cause arteries to narrow and
harden, which can lead to a heart attack or stroke later in life.
• Asthma and other breathing problems. The extra weight on
the child's body can cause problems with the development and
health of your child's lungs, leading to asthma or other breathing
• Sleep disorders. Sleep apnea, a condition in which the child may
snore or have abnormal breathing when he or she sleeps, can be
a complication of childhood obesity.
• Early puberty or menstruation. Being obese can create hormone
imbalances for your child. These imbalances can cause puberty
to start earlier than expected.
• Low self-esteem and bullying. Children often tease or bul y
their overweight peers, who suffer a loss of self-esteem and an
increased risk of depression as a result.
• Behavior and learning problems. Overweight children tend to
have more anxiety and poorer social skil s than normal-weight
Dr. Mona Issa Farrag

Implantable Contact Lenses
Don't want Glasses?
Don't want LASIK?
Don't want to wear contact lenses?
We still have a solution -
IMPLANTABLE CONTACT LENSES
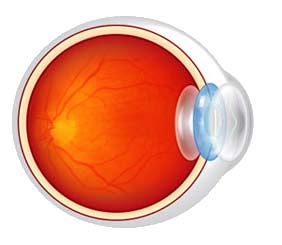
What are Implantable Contact Lenses (ICL)?
Implantable collamer lenses (ICL) are a type of
After this treatment, the patient can leave the
phakic intraocular lenses which are specialized
hospital after a couple of hours and is able to enjoy
lenses made of plastic or silicone material which
new sight almost immediately and go back to his/
are implanted into the eye to permanently reduce a her active lifestyle.
person's dependence on glasses or contact lenses.
They are called Phakic lenses as they are implanted The ICL is invisible to the naked eye: The ICL works
into the eye without removing the eye's natural
like a contact lens. The difference is that the lens is
lens. The lens is inserted through a small incision
placed inside your eye, rather than on the surface.
and placed just in front of or just behind the iris.
The only way that you will know that it is there, is
the improvement in your eyesight. You can not see
The lens is soft and tiny, much like the natural lens, the lens once it is inside your eye.
but does not replace it. The ICL is specially shaped
to correct nearsightedness or farsightedness.
Deciding to Go Ahead?
Phakic lenses once placed in the eye, focuses the
Talk to your doctor about your expectations, medical
light rays on the retina providing clear distance
history, eye history, or past eye examination. This
vision without the aid of glasses or contact lenses.
will help you decide whether phakic lenses are right
Advanced phakic lenses, also called as Toric ICL go for you. After a detailed eye examination, you will
a step further. They can also correct the cylindrical
be counseled and provided the various options of
vision correction.
What makes ICL Special?
Talk to your doctor about your expectations,
ICL treatment is completely safe even if you have
medical history, eye history, or past eye
thin corneas, surgically stabilized keratoconus,
examination to help you decide whether phakic
dry eyes, or large pupils as it does not involve
lenses are right for you
removing tissue from the cornea. It is also suitable
for candidates who are otherwise unfit for laser
vision correction and can correct a large range of
refractive errors. In addition ICL gives the patients
the ability to see well in low light such as dusk or at
Dr. Deepak KhoslaOphthalmologist
Throat Irritation
Patients present with several throat
symptoms like irritation, tickle, cough,
throat clearing and a sensation of
mucous in the throat.
irritation because of the substances contained in
In the majority of cases, there is little to find on
the smoke, it causes further drying and promotes
examination of the ear, nose and throat. However,
mouth breathing.
a thorough examination is mandatory to exclude
more serious il nesses. Most patients can be easily
Anxiety and Stress. Stress causes an overall
managed with reassurance and careful explanation
increase in muscle tension and this effect is often
that the throat is a very sensitive area and the cough
noticed in the throat, either as a mild change in
reflex is a natural protective mechanism to an irritant.
the quality of voice, or as a sensation of tightness
or lump in the throat which then leads to constant
Common Causes of Throat Irritation
throat clearing. Stress also increases acid
production in the stomach, which may worsen the
Reflux. Acid stomach contents may pass upwards
effect of reflux.
to the throat causing irritation as a result of
low-level chemical burn. In fact GERD (gastro-
Coughing and Throat Clearing. The very act
esophageal reflux disease) is a common cause of
of coughing or throat clearing can actual y cause
chronic sore throat, cough and inflammation of
throat problems to become worse or longer lasting.
the larynx (wind pipe).
This occurs as a result of the violent bringing
together of the vocal cords, which in itself can
Mouth Breathing. The nose is the air conditioner
cause inflammation of the throat. This can quickly
for the respiratory tract. It warms and moistens
lead to a self-perpetuating condition.
the air we breathe. If the nose gets blocked and
mouth breathing takes over, then this effect is lost Infection. Upper respiratory tract infections can
and the throat and the air ways become dry and
sometimes lead to long lasting throat problems.
This occurs as a result of excessive coughing and
swal owing of mucous, in addition to inflammation
Rhinitis. Rhinitis causes nasal block with nasal
of the throat. These effects can continue long after
and post nasal secretions. The latter drips to the
the cold itself has gone.
back of the throat causing irritation and excessive
Drugs. Some drugs can cause cough or throat
irritation. ACE inhibitors (drugs used for lowering
Asthma. Many patients with rhinitis also have
the blood pressure) often cause dry cough. Non
asthma, and vice versa. People with al ergic
steroidal anti inflammatory drugs can increase
rhinitis and asthmatic bronchitis can have
acidity and reflux.
sensitivity in the area in between, i.e. the throat.
Poor air quality. Pol utants, fumes, dust and
smoke cause irritation of the lining of the throat.
Also air conditioning and central heating dries up
Dr. Hisham Halabi
the air leading to a dry, poor quality air. This can
have adverse effect on the throat.
Smoking. Smoking has serious effects on
the lining of the throat. In addition to causing
Intra-Articular and
Soft Tissue Injections
Intra-articular and soft tissue injections of steroids
• Infection: Local or systemic
are useful in control ing refractory pain, suppressing
• Intra-articular injury/Haemarthrosis
inflammation, and increasing joint function in patients • Severe joint destruction with instability
with arthritis and musculoskeletal disorders.
• Regional osteoporosis
• Anticoagulant patient
• Uncontrol ed diabetes
The clinical effects of local steroid injection are anti-
• Unclear diagnosis
inflammatory with a diminution of redness, swel ing,
heat and pain. There may be a systemic improvement
Frequency of Injection
in function as wel . The clinical efficacy is wel known
Conventional opinion holds that three injections can
but the biochemical mechanism is unclear.
be given safely into the same joint over a 12-month
period. In addition, response to previous injection
Different theories have been proposed, including
is a relevant factor in deciding whether and when
stabilisation of lysosomal membranes, inhibition
to proceed with re-injection. Significant therapeutic
of cel ular metabolism and decrease in synovial
benefits fol owing injection support the use of a
second injection when the symptoms have returned.
Failure to obtain significant relief after two injections
clearly argues against additional injections.
• Rheumatoid Arthritis
• Seronegative arthropathies: Ankylosing Spondylitis, Dosage and Volume
Psoriatic Arthritis, Reiter's Syndrome
Tendons and ligaments should have minimum possible
• Crystal induced Arthritis: Gout & Pseudo gout
amount of volume and steroid injected. A smal volume
• Osteoarthritis with Synovitis
avoids painful distension of the structure and the
• Bursitis: Subacromial, Olecranon, Pes anserine,
smal dose minimises risk of rupture. Most tendon
Pre-patel ar, Trochanteric
lesions and smal joints need 10-20mg of steroid and
• Tendinitis/Fasci tis: Supraspinatus, Bicipital, de
1-2 ml of local anaesthetic. Larger joints and bursa
Quervain's, Tenovaginitis/Trigger finger, Plantar
require 30-40mg and 5-10ml of local anaesthetic.
fasci tis/heel spur
• Entrapment Neuropathies: Carpal Tunnel
Problems with Injection Therapy
Syndrome, Tarsal Tunnel Syndrome
Problems arise when:
• An inappropriate drug is chosen. Virtual y insoluble
steroid suspensions are used because intra-
articular soluble steroids wil rapidly clear into the
Dr. Dilip Malhotra
systemic circulation. Methyl Prednisolone acetate
Orthopaedic Surgeon
(Depo-Medrol) and Triamcinalone acetonide
(Kenacort) are best suited for the purpose.
Hydrocortisone is short acting.
• Too large a dose is used.
Intra-Articular and Soft Tissue
Injections of Steroid
• Injections are given too frequently.
• Spread of drug to adjacent tissues.
• Insufficient attention is directed to the
cause of the lesion.
• Improper aftercare.
• Systemic: Facial flushing, menstrual
irregularities, impaired diabetic control,
syncope (fainting), anaphylaxis (usual y
to the local anaesthetic).
• Local: post injection flare of pain
(due to crystal induced synovitis),
skin depigmentation, subcutaneous
atrophy, bleeding/bruising, soft tissue
calcification/steroid chalk, tendon
rupture, steroid arthropathy, joint/soft
tissue infection (rare).
Advice to Patients
• Immediate pain relief due to the effect
of the local anaesthetic wil disappear
in a couple of hours.
Headache is a common complaint which we all experience
every now and then. It is a major symptom in many
of ordinary illnesses such as common cold, errors of
• Occasional y initial worsening of
refraction, sinusitis, tooth problems, constipation, etc.
pain may occur (treat with rest, ice,
Paracetamol or anti inflammatory
To consider headache as an alarm for a serious illness, it must be of
a specific character and is usually accompanied by other symptoms
• The steroid may take several days to
of clinical importance:
become effective.
• Physical exertion of the part should be
1. Unilateral headache: Unilaterality is very significant and should
avoided for two weeks.
always arouse suspicion of an underlying pathology such as brain
tumor or vascular lesion.
Intra-articular and soft
2. Chronicity: Chronic headache should call for more investigations
as MRI or CT scan of the brain as well as EEG to rule out any
tissue injections of steroids
are useful in controlling
3. Change in the character of the headache: "I have never
refractory pain, suppressing
experienced like this before ". This is a common statement which
inflammation, and
should always be taken seriously.
4. History of trauma or fever.
increasing joint function in
5. Other important associated symptoms:
patients with arthritis and
• Blurring of vision or double vision
musculoskeletal disorders.
" • Projectile vomiting
• Weakness in one or two limbs on one side (usually opposite
• Deterioration in conscious level or difficulty in speech
• Difficulty in walking or maintaining balance
• Urinary or stool incontinence
Dr. Hassan MouktharNeurosurgeon
SCREENING MAMMOGRAPHY:
What Everybody Should Know
Other types of breast screening
Dr. Sagiraju Varma
Digital mammography is similar to film screen
mammography but images are acquired in digital form.
Sensitivity and specificity of screening ultrasound are not
Screening mammogram is a radiographic Present indications are for evaluation of breast nodule
examination of the breasts performed for early
(solid or cystic), clinically occult mammography findings
detection of breast cancer in asymptomatic
in dense breast tissue, supplementary examination of
women with high risk breast cancer and guidance during
It is recommended that women get mammogram done at
age of forty and annually thereafter.
Screening MRI is not used in every day clinical practice.
Present indications are pre-operative local staging,
There are instances when screening should start earlier.
differentiation between post operative scar and
Patients with history of Hodgkin's disease treated
recurrence carcinoma, CUP [Carcinoma with Unknown
with radiation or those with strong family history of
Primary] syndrome, prosthesis and problem cases.
breast cancer. A woman treated for Hodgkin's disease
surveillance may begin 10 years after chest wall/
Role of primary physicians
mediastinal irradiation. For patients with history of first
The most important thing is to recommend a
degree relative, screening should begin 10 years before
mammogram for asymptomatic women. Reassure that
the age at which the relative was diagnosed.
mammography should not be painful, although certain
degree of temporary compression is necessary to obtain
For routine mammography, four views are obtained.
Additional views may be required in some patients. The
amount of radiation for routine mammogram is very small Remind the patient to bring all the previous
[0.2 rads/2mGray].
mammograms to the imaging center at the time of next
examination. Also remind that she may be called back
The risk for developing cancer due to bilateral
for additional views. The call back does not always mean
mammography in a 45 year old is 0.0055%.
something is wrong.
Benefits of mammography are seen immediately; the
potential side effects after 20-30 years.
Comparison filmsIf the patient has multiple sets of prior films, radiologists
KEY POINTS
like to compare with the studies that are two years old.
• Annual screening mammography should begin
Sensitivity of screening mammography depends on the
• Mammography is stil the best screening test to
density patterns; the sensitivity seems to decrease as
detect sub clinical breast cancer.
the glandularity of the breast tissue increase.
• The sensitivity of mammography is in the range
Difference between screening mammogram and
diagnostic mammogram
• False negative rate is approximately 10-15%.
A screening mammogram is performed on asymptomatic
• An individual's risk of developing breast cancer
patients as part of routine annual surveillance. A
increases with increasing age.
diagnostic mammogram is performed when the patient
• Most breast cancers occur in women with no
has history of breast cancer or presents with breast
family history of the disease.
related complaint.
Day-Care Anaesthesia
Day-care surgery offers several advantages to
patients, doctors, and insurance companies.
Recent advances in medical technology,
anaesthesia and pain management have
allowed a huge expansion of this modality of care with a
consequent reduction in the need for hospitalization.
Successful conduct of procedure is based on :
• careful patient selection.
• type of surgeries based on the facilities available.
• Postoperative nausea and vomiting. The incidence
• appropriate preparation and planning.
varies between 2.2% and 4.6% and this may delay the
patients discharge at times.
There is no significant relationship between pre-
existing diseases, extremes of age and incidence of
Postoperative pain is the most significant complaint
perioperative complications in a day care setting,
following ambulatory anaesthesia. Factors associated
provided proper attention is paid to preoperative
with severe pain in the post anaesthesia care unit
assesment, prepration and discharge planning.
(PACU) include younger adults, patients with a
Children are excellent candidates for daycare surgery
larger body mass index (BMI), prolonged duration of
as it provides minimal separation from parents and
surgery, orthopaedic, urological and plastic surgeries.
minimal exposure to potentially contaminated hospital
A concept of multimodal analgesic technique with
combination local anaesthetics, non-steroidal anti-
inflammatory drugs (NSAIDs), opioids has shown
Pre Procedure Evaluation and Preparation
better results.
In addition to reducing anxiety about the surgery and
anaesthesia, it identifies potential medical problems in
• Post dural puncture headache. Due to early
advance and initiates appropriate corrective measures.
ambulation in patients having spinal anaestheisa it
Thereby, minimising the numbers of cancellations and
is almost negligible with use of small 25- or 27-gauge
The patients are allowed clear liquids up to 4 hours
Recovery and Discharge Process
before surgery, without increasing residual gastric
The Aldrete Score is used for evaluating patient recovery
volume. Administration of antacid and antiemetic can
after anaesthesia and patients' "home readiness" is
reduce both residual gastric volume and acidity. The
assessed with modified Post Anaesthesia Discharge
patients should take all chronic oral medications up to 1
Scoring system (PADSS). These scores are useful in
hour before the procedure.
allowing documentation of objective measurements of
clinical recovery.
Total intravenous anaesthesia (TIVA) provides
Following day care procedure, patients should be
advantages for all short surgical procedures, as even
discharged home with an adult escort, who ideally will
after prolonged infusion there is rapid recovery .
continue overnight supervision of patients' recovery and
patients should also have ready access to healthcare
Spinal anaesthesia, commonly used with local
anaesthetic agents specific to the expected duration of
surgery, provides superior recovery profiles .
Newer technology i.e. ultrasound-guided interscalene
Dr. Avijit Gaikwad
and supraclavicular blocks are used effectively and
safely for shoulder and hand surgeries as compared to
landmark based nerve blocks.
After Tooth Extraction
Extracted tooth socket heals over a
period of one to two weeks, gum
tissue takes about 3-4 weeks and
complete healing of the bone can
take about 6-8 months depending on your care
of this area. Some discomfort, bleeding and
swelling is be expected in the first 24 hours.
Following these simple instructions will normally be Medications: Pain medications may be taken every
all that is needed.
four hours as needed.
Do Not Disturb the Wound: Simple pressure from
Swelling: To prevent swelling, apply an ice pack
a piece of gauze is usually all that is needed to
outside of your face in the area of the extraction
control the bleeding and to help a blood clot to
during the first 24 hours. This is the best way to
form in the socket. Blowing your nose or sneezing
avoid excessive swelling.
violently can dislodge the blood clot and impair
Diet: For the first 24-48 hours, you should maintain
a soft diet. Also avoid carbonated drinks and
Do Not Smoke or Use Tobacco Products or Alcohol
hot beverages for 3-4 days. Eating immediately
for 72 Hours because smoke can interfere with the
following the procedure is not recommended.
healing process, promote bleeding and can cause a
very painful situation known as "dry socket".
For Women Only: If you are taking birth control
pills or are in the first 22 days of your menstrual
Brushing: It is important to keep the area as
cycle, your are twice as likely to develop a ‘dry
clean as possible to prevent infection and promote
socket', which is a very painful condition, after an
healing. This area can be gently and carefully
wiped with a clean, wet gauze pad or cloth. After 48
hours teeth may be brushed and flossed gently.
Anesthesia Warning: When a local anesthetic is
used your lip, tongue and cheek will be numb for
Mouthwash: Avoid all rinsing for 24 hours after
several hours after the procedure. During this
extraction. After the first 24 hours you should
period you must be careful not to bite or scratch
gently rinse of this area using warm salt water or
this area which can lead to serious soft tissue
mild antiseptic.
Bleeding: Follow the verbal instructions regarding
Follow-Up Appointment: You are required to return
the control of postoperative bleeding. It is normal
for follow up in one week to check on the healing of
for some blood to ooze from the area of surgery for this area.
12 hours. We will also give you a packet of gauze
to take with you to use at home if the bleeding
continues. Hold it firmly in place, by biting down on
the gauze pad for about 30-60 minutes.
Dr. John MeakkaraDentist
the Big Little ThyroidThe thyroid is a small gland situated in the front of the neck
below the Adam's apple and can usually neither be felt nor
seen. However this little gland is a very big player when it
comes to survival. The thyroid gland affects every cell in
the body by increasing metabolism, within the cells, when
When the metabolic rate of a cel is increased, the
cel requires a larger amount of fuel which is basical y
oxygen and substrates in the form of carbohydrate,
weight despite over eating.
fat or protein. And when anything burns, there is
4. Musculoskeletal system. There is a loss of
heat produced as a by-product. To increase delivery
weight and a decrease in muscle mass.
of oxygen and food to cel , the cel has to receive a
5. Urogenital system and sexual
greater amount of blood supply and therefore the
characteristics. Thyroid hormones in physiologic
heart has to work faster and harder. The thyroid
amounts are necessary for every aspect of sexual
hormones also potentiate the action of circulating
development and function.
catecholamines (substances of "fight and flight") and,
therefore, the action of normal circulating levels of
One can see that a decrease in circulating thyroid
catecholamines is amplified. By affecting the cel the
hormone leads to an exact opposite of the above
thyroid affects various organ systems in the fol owing
When we talk about common thyroid afflictions, we
1. Brain. In the foetus and growing child, thyroid
talk about an overactive thyroid, an under active
hormones are required for brain development
thyroid, a thyroid that is enlarged and presses on
and lack of it early in life causes the brain to
adjacent structures causing problems with breathing,
remain under developed. Increased activity in
swal owing and voice change, and final y a thyroid
the Reticular Activating System (center that is
that is cancerous.
responsible for keeping us awake) and other
parts of the brain make us anxious, alert and
Common investigations include the thyroid function
awake, causes muscles to contract briskly and
tests of which the TSH or thyroid stimulating hormone
stay contracted for longer than is usual. These are
is the most important, ultrasound scan of the thyroid,
seen as an inability to sleep, tremors, a staring
fine needle aspiration cytology of the thyroid, thyroid
look, being hyperactive.
antibodies and isotope scan.
2. Heart. Increase force and rate of contraction
thereby increasing the amount of blood flowing
Treatment may be with drugs, surgery or with radio
out of the heart and this manifests as a pounding
active iodine ablation depending on what the problem
rapid pulse.
is or may include a combination of the above.
3. Intestines. Because the thyroid hormones
increase requirement of food, the person develops
an increased appetite and eats more. Because
there is increased activity of muscle cel s of the
Dr. Ivo Fernandez
intestines, the intestine contracts faster causing
diarrhoea. However even this increased food
intake is not sufficient and often cel s borrow from
body stores and there is paradoxical y a loss of
ULTRASOUND IN PREGNANCY:
Of course, initialy, skeptics, mostly from the
medical community, were indignant at this
"violation" of the secrecy of the pregnancy.
Ultrasound was accused of al possible
evil side effects. However, with time and technical
advances, and despite the ferocious war of the
"skeptics", ultrasound became the eyes and the ears
of modern obstetricians, al owing them to make valid
decisions for best fetal outcome. Most importantly, in
more than 50 years of ultrasound use, and contrary to
what the skeptics were claiming, not a single fetal or
maternal untoward effect has been reported from the
use of ultrasound. Perhaps the only drawback is the
financial aspect, as an obstetrical ultrasound may be
However, over the years, it has been suggested that
low risk pregnant women may not benefit from any
ultrasound done during their pregnancy. On the other
hand, some obstetricians have suggested (and are
actual y practising) ultrasound on every pregnant
woman coming for every antenatal visit.
There is no doubt that high risk pregnancies should
al be checked with frequent ultrasound. Obstetricians
wil be amazed at the amount of information they
Though skeptics were
can obtain from even a quick ultrasound (amniotic
fluid, presentation, placenta, etc.), information that
indignant at the "violation" of
could have been unsuspected before, and when
the secrecy of the pregnancy,
found, could make a tremendous difference to the
ultrasound became the eyes
and the ears of modern
But frequent ultrasound exam though safe, should
obstetricians, allowing them to
not be imposed on low-risk pregnant women, unless
they ask for an ultrasound. In fact, majority of patients
make valid decisions for best
show tremendous satisfaction when they are given the
fetal outcome.
chance to watch their fetus by ultrasound, especial y
the 4D ultrasound. As obstetrical ultrasound has been
shown to be safe so there is no reason to deny this
satisfaction to pregnant women.
Antenatal care has been so much emphasized not only
for its medical necessity, but also for its psychological
Dr. Roland MouawadOb-Gynaecologist
and emotional support to pregnant women.
Obstetrical ultrasound is a major factor enhancing this
kind of support. It may not be medical y indicated, it
is certainly psychological y and emotional y very much
Urinary Tract Stones
The first documented urinary tract
stones were found among the 7,000
year-old remains of the pelvis bones of
teenage boy in El-Amara. Before the industrial
revolution in Britain, stones in the bladder were
more common than in upper urinary tract. Around
the turn of the nineteenth century, upper tract
stones disease began to become more prevalent.
In developing countries, bladder stones are still
endemic and is more common in males.
The presenting symptoms of upper urinary tract stones
are loin pain which may radiate to the groin in a colicky
nature sometimes associated with hematuria (blood in
urine). If urinary infection is present there may also be
symptoms and signs of infection as dysuria (pain while
• Sedentary occupations
passing urine) and frequency of micturition. Bladder
• Anatomical abnormalities of the urinary tract
calculi (stones) may cause changes in the urinary
stream due to the stone acting as a bal valve over
The common types of the stones are:
the bladder neck and the symptom of strangury (slow
• Calcium oxalate, calcium phosphate or combinations
painful urination) due to strong painful contraction of the • Uric acid, cystine.
bladder in attempt to evacuate a calculi.
• Magnesium ammonium phosphate (Struvite).
Risk factors for stone formation
• Presence of promoters of stone formation
High risk patients with urinary symptoms especial y loin
• Absence of inhibitors of stone formation
pain and hematuria need to be evaluated by:
• Urinary tract infection
• Urine analysis and culture.
• Urinary stasis
• Blood tests for renal function, calcium, uric acid,
• Concentrated urine due to poor fluid intake
phosphate and magnesium.
• Diet too high or too low in calicum
• Plain X-ray kidney, ureter and bladder (KUB)
• Ultrasound kidney, ureter and bladder
• Intravenous pyelogram ( I.V.P )
A kidney stone is a hard mass developed from • C.T scan crystals that separate from the urine within the urinary tract.
Treatment is according to the size and the position of
stone by medical or surgical means; endoscopic or open
surgery especial y for the stag- horn stone. Some stones
can be crushed by special instruments or by extra
corporal shock wave lithotripsy (ESWL) .
Fainting is defined as a loss of awareness or consciousness
for an interval of time. The medical term used to describe
fainting is syncope.
How does it occur? Fainting occurs when the blood supply to the brain is not enough for its functioning. This may happen
in any condition when the heart is not able to pump enough blood to the brain as in case of heart valve
problems; and if the heart rate is either too slow or too fast. It may also happen if the person is fasting for
too long resulting in fall in his blood sugar level.
What are the symptoms of fainting? The symptoms that a patient may feel before fainting are palpitations, i.e. feeling or hearing the heart
beating very fast, nausea, dizziness, weakness or a black out.
How is it diagnosed?
The doctor should be consulted immediately to find out the cause. The doctor will take the patient's
medical history, check the pulse and blood pressure. He will also suggest some lab tests and
electrocardiogram (ECG). The ECG is a recording of heartbeat. He may also suggest echocardiogram which
is an ultrasound scan of the heart to find out any abnormality in the heart valve.
How is it treated?
The treatment will depend upon the cause of fainting. In case of abnormality in heartbeats, medicine will
be prescribed. In case of reduction of blood flow to the brain because of problems in the blood vessels,
specific blood flow increasing drugs may be prescribed.
What first aid can be provided?
The patient returns to consciousness when normal blood flow to the brain returns. The patient
should be made to lie down with his legs in a raised position. If the patient has normal
breathing, his legs should be raised above the level of his chest as this will help in supplying
more blood to the brain and help the patient to come back to normal.
To prevent fainting in future, avoid sudden changes in posture and intense
Religion, Spirituality, and
an experience includes support for the patient's suffering, the avoidance of undesired artificial
Dr. Samy GoudaNeurosurgeon
prolongation of life, involvement of family and/or close friends, resolution of remaining life conflicts, and attention to spiritual issues that surround the meaning of illness and death.
Clinicians can and should help dying patients find meaning and hope through recognition of the
Spiritual, religious, and cultural beliefs
and practices play a significant role in the lives of patients who are seriously ill and dying. In addition to providing an ethical
spiritual dimension of their experience. Although
foundation for clinical decision making, spiritual
they may lack the expertise to address spiritual
and religious traditions provide a conceptual
concerns in depth, healthcare professionals should
framework for understanding the human experience be able to discuss spirituality with their patients of death and dying, and the meaning of illness and and identify those in spiritual distress so that suffering.
appropriate referral may be made to spiritual care providers. These include chaplains, community-
The importance of spiritual and religious beliefs
based clergy, spiritual directors, pastoral
in coping with illness, suffering, and dying is
counselors, and culturally based healers.
supported by clinical studies as well as individual narrative descriptions. Most patients derive
Spiritual care is recognized as a necessary domain
comfort from their religious/spiritual beliefs as they of palliative care. Guidelines for interprofessional face the end of life, and some find reassurance
spiritual care as well as an implementation model
through a belief in continued existence after
for spiritual care were developed by a national
physical death. However, religious concerns can
consensus conference of experts. In their report,
also be a source of pain and spiritual distress, for
practical tools as well as recommendations are
example, if a patient feels punished or abandoned
presented to help clinicians integrate spirituality
by God. Furthermore, beyond the role of religious
more fully into patient care.
faith in coping and adjusting to illness, religion also influences patient's medical decisions, both about active treatment and end of life care.
A common goal for the dying patient, family members, and the health care professional is for a meaningful dying experience, in which loss is framed in the context of a life legacy. Such
A common goal for the dying patient, family
members, and the health care professional is for
a meaningful dying experience, in which loss is
framed in the context of a life legacy.
Though pomelo juice is acidic in nature, it helps in the digestive
process of the body, by having an alkaline reaction after digestion.
• Pomelo rind contains huge amount of bioflavonoid that can stop the cancer cel s from spreading
the effect of breast cancer in a patient, by making the body
get rid of the excess estrogen.
Nutrition Facts
• The high amount of vitamin C present in the body makes the
fruit an effective stimulant that facilitates in strengthening
and maintaining the elastic nature of the arteries.
Amount Per Serving
• Pomelo is also effective against fatigue, diabetes, fever,
Calories 72 Calories from Fat 1
insomnia, sore throat, stomach and pancreatic cancer and other such infectious diseases.
% Daily Value*Total Fat 0 g
• Pomelo contains pectin which proves to be very effective in
Saturated Fat 0 g
reducing the accumulation of arterial deposits in the body,
thereby clearing out al the impurities.
Cholesterol 0 mg
• Pomelo is also useful in reducing the cholesterol count in the
Total Carbohydrates 18 g
body, thus saving you from running the risk of various heart
Dietary Fiber 2 g
related problems.
SugarsProtein 1 g
• Pomelo can also prove out to be useful for people seeking
out weight loss. The fat burning enzyme in pomelo absorbs
Vitamin A 0% Vitamin C 193%
and reduces the starch and sugar content in the body
Calcium 1% Iron 1%
contributing towards weight loss.
*Percent Daily Values are based on a
• Pomelo is also useful in cleaning the RBCs which are very
2,000 calorie diet. Your daily values may
be higher or lower depending on your
essential for the body to breathe fresh air. It keeps the RBCs
calorie needs.
away from al sorts of toxins and impurities.
Confront Your Exercise Enemies it
What gets in the way of your exercise? Whether
it's work, the couch, your kids, or the grubby fella e
hogging the treadmill, now's the time find a way
to work around these roadblocks to success.
Today, you will overcome one of your exercise
enemies. The truth is that there's a way around
every exercise obstacle. It just takes a little
planning and persistence.
Do you have trouble getting moving when you get
home from work as you're drawn into reruns of
The Office? Pack a bag in the morning and hit the
gym, or go for a walk before you head home.
Are you a stay-at-home mom and can't find
anyone to watch the kids? Put them in a stroller
or jog alongside as they ride bikes or scooters.
The kids get some fresh air and exercise, too!
source: Sharecare
Source: http://www.ihb.net/pdf/newsletter/2012/issue182012-lowres.pdf
Evolution of Blood Gas Analysis - Focusing on the Source of Impaired O2 Supply to the Tissue Ellis Jacobs, Ph.D, DABCC, FACB Associate Professor of Pathology, NYU School of Medicine Director of Pathology, Coler-Goldwater Hospital and Nursing Why measure blood gases Overview of acid-base disturbances Use of the Acid- Base Chart
Clinical Case Studies Cognitive Behavioral Treatment of Postpartum Onset: Obsessive Compulsive Disorder With Aggressive Obsessions Lisa M. Christian and Eric A. Storch Clinical Case Studies DOI: 10.1177/1534650108326974 The online version of this article can be found at: Additional services and information for can be found at:

