Medcon.gr
CORNEAL IONTOPHORESIS
EXPERIMENTAL EVIDENCE
CLINICAL EVIDENCE
CORNEAL IONTOPHORESIS
EXPERIMENTAL EVIDENCE
CLINICAL EVIDENCE

CORNEAL IONTOPHORESIS
Iontophoresis consists of the transfer of molecules, with an ionic charge, inside the tissues to treat, thanks to a low intensity
electric field. Among these molecules various drugs are included. The rapidity of passage of the ionic molecules can be
increased by varying the intensity of the current applied or the characteristics of the preparation.
PRINCIPLES OF IONT
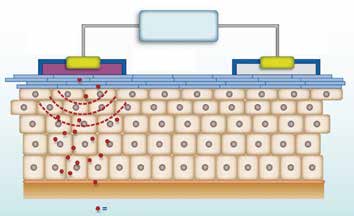
Using the physical principle of ionic migration from one
Principle electrode
(following molecule
pole to another (Fig. 1), specific polarized pharmaceu-
tical agents are prepared containing either positive or
negative ions, or both (bipolar). These polarized drugs
are applied to the electrodes according to their polari-
ty: for example, if the drug has a positive polarity it will
be applied to the positive electrode, if it has negative
polarity to the negative electrode, if bipolar indifferen-
tly to one or the other, while the other pole is placed on
the boundary of the area to be treated. Thus, applying
Penetration of the molecule into the tissue to be treated
the electrode with the drug on the area to be treated
Fig.1 Diagram of the iontophoresis process.
and the other at a maximum distance of about 10/20
cm, the current will transport the drug into the tissues,
as the ions of the drug migrate towards the opposite
polo until the drug is completely absorbed.
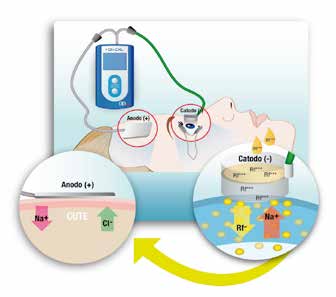
In corneal iontophoresis, the treatment is carried out by means of the application on the patient of two electrodes connected
to a continuous current generator (Fig. 2).
The principal electrode (- pole) is in a polycarbonate ring, specific for medicinal use, which is applied by suction onto the
cornea to be treated; the other electrode (+ pole) is a patch to be placed on the forehead of the patient. The current flow
(low intensity) between the two electrodes allows a specific formulation of riboflavin (RICROLIN®+), specifically developed
for iontophoretic administration, to rapidly penetrate into the corneal stroma, through the intact epithelium (that is without
de-epithelization), guaranteeing optimal imbibition.
The charge flow is possible thanks to the continuous current
from the battery power supply. The intensity that is produced for
the iontophoresis is of 1 mA/min (5 minutes of treatment, 5 mA
total). The duration of the treatment is automatically monitored
by a suitable software package of the generator program. When
5 minutes of treatment is reached, the iontophoresis automati-
cally stops. In ophthalmology iontophoresis is a well-known and
documented technique, and has been studied for several years
with many scientific publications. One can cite the research of
Frucht-Pery et al. on trans-corneal and trans-conjunctival ad-
ministration of dexamethasone or the studies conducted in the
USA by the Eye-Gate company. Iontophoresis, at the current in-
tensity of 1 mA, is completely harmless for the human cornea
and the other sensitive structures of the eye.
Fig.2 Corneal iontophoresis.

Diffusione della riboflavina
CORNEAL IONTOPHORESIS
EXPERIMENTAL EVIDENCE
Experimental studies with the application of riboflavin by means of iontophoresis have shown the penetration of this mole-
cule into animal corneas (in vivo) and in human corneas (ex vivo). The penetration was evaluated both directly (measured by
means of the determination of the concentration of riboflavin in the corneal stroma and aqueous humor), and indirectly (by
means of the biomechanical evaluation of the increase of stromal rigidity after CXL).
In the biomechanical studies all the corneas were treated, following imbibition with iontophoresis, with ultraviolet rays (UV-
A) at the dose of 3 mW/cm2 or 10 mW/cm2 to evaluate the effect of different intensities of irradiation on the structural resi-
stance of the corneal stroma.
CONCENTRATION AND DIFFUSION OF RIBOFLAVIN AND EFFECT ON STROMAL FIBERS
The studies carried out at the University of Toulouse (Malecaze et al., IOVS 2014) evaluated, on an animal model, the
concentration of riboflavin (HPLC), the diffusion/distribution of riboflavin (two-photon microscopy) and the stromal modifi-
cations (dimensions and course of collagen fibers by means of two-photon microscopy, Second Harmonic Generation) after
standard EPI-OFF CXL versus transepithelial cross-linking with iontophoresis and UV-A irradiation at 10 mW/cm2. The studies
demonstrated that, notwithstanding the concentration of riboflavin administered by means of iontophoresis was half that of
the standard treatment, its diffusion was optimal for all the cornea (Fig. 3) such that the effect of CXL on the stromal fibers is
identical to that of the standard EPI-OFF technique (Fig. 4).
The quantity of riboflavin administered by means of iontophoresis was thus adequate to obtain an efficacious cross-linking of
the anterior two-thirds of the stroma, similar to that obtained with the standard EPI-OFF technique.
Second Harmonic Generation
Cornea treated with iontophoresis and UV-A 10 mW for 9 min
Cross-linking with
Cornea treated with standard CXL
Fig. 4 Two-photon microscopy shows the corneal fibers perfectlycompact after
CXL-iontophoresis, as in standard cross-linking (EPI-OFF).
Fig. 3 Riboflavin diffusion.
CORNEAL IONTOPHORESIS
CONCENTRATION OF RIBOFLAVIN IN HUMAN CORNEAS
Mastropasqua et al., AJO 2014, carried out a kinetic study on ex vivo human corneas to determine the difference in
concentration of the riboflavin in the anterior, intermediate and posterior stroma, 3 different procedures of imbibition (30'
EPI-OFF with RICROLIN®; 30' EPI-ON with RICROLIN® TE; 5' Iontophoresis with RICROLIN®+). The corneas, after imbibition,
were divided into 3 slices by means of a femtolaser cut (I: 0-150 microns; II: 151-300 microns; III: residual stromal bed,
(Fig. 5) and then analyzed by HPLC. The results obtained (Fig. 6) confirm those obtained by Malecaze on an animal model.
L. Mastropasqua et al. Am J Ophthalmol 2014;157:623–630.
Fig. 5 Separation of the corneal stroma with
femtolaser in 3 slices for HPLC analysis.
Fig. 6 Concentration of the riboflavin in the anterior (SLICE A), intermediate (SLICE B)
andposterior (SLICE C) stroma after imbibition with the standard EPI-OFF (blue diagram),
EPI-ON with IONTOPHORESIS (red) and EPI-ON (green) techniques. The results obtained con-
firm those of the study by Malecaze (page 5) that demonstrate how the quantity of riboflavin
administered with iontophoresis is adequate to guarantee efficacious cross-linking.
STRUCTURAL RESISTANCE OF THE CORNEA
A study carried out in collaboration with the University
of Dresda (Spoerl et al.) and the Clinical Institute Hu-
manitas of Rozzano (Vinciguerra et al.) evaluated the
efficacy of iontophoresis measuring the increase of the
biomechanical resistance on human corneas (ex vivo)
after UV-A irradiation without removing the epithelium
and compared to other techniques of passive imbibition,
both EPI-OFF and EPI-ON. The method used was the
stress-strain test. The results showed how iontophoresis
combined with UV-A irradiation at 10 mW was efficacious
in increasing structural resistance of the treated corneas
CXL standard EPI-OFF
with respect to other techniques of impregnation and
power of irradiation (Fig 7).
Fig. 7 Group 4 (iontophoresis + UV-A 10 mW, 9' irradiation) showed, with
respect to Group 2 (standard CXL), an increase in structural resistance of
the corneas of more than 6%. The treatment with iontophoresis + UV-A 10
mW was also more efficacious with respect to the combination iontopho-
resis + UV-A 3 mW (30' irradiation, Group 3).
CORNEAL IONTOPHORESIS
CONCENTRATION OF RIBOFLAVIN IN HUMAN CORNEAS
IS THE QUANTITY OF RIBOFLAVIN ADMINISTERED WITH
IONTOPHORESIS ADEQUATE? IS THE EPITHELIUM A BARRIER?
The results of the study by Malecaze on an animal model were confirmed by an interesting experimental study carried out at the
Bietti Foundation in Roma (Lombardo et al.). The study had the aim of analyzing the diffusion (scattering) of riboflavin before
and after treatment with transepithelial CXL with iontophoresis compared with the standard CXL treatment. Iontophoresis was
efficacious in distributing riboflavin in the corneal stroma through the integral epithelium. After transepithelial illumination of the
corneawith a UV-A lamp of 10 mW/cm2 it was also demonstrated how the quantity of stromal riboflavin was more than adequate
for an efficacious corneal cross-linking (Fig. 8).
Fig. 8 A) Scheimpflug image of the cornea immediately after
Fig. 9 A) Scheimpflug image of the cornea immediately after
iontophoresis. B) Corneal densitometry (integrated values up to
administration of RICROLIN®. B) Corneal densitometry (integra-
280 microns of thickness and normalized with respect to the va-
ted values up to 280 microns of thickness) immediately after
lues of basal corneal scattering) immediately after iontophoresis
imbibitionwith standard RICROLIN® (blue curve) and after UV-A
with imbibition of RICROLIN®+ (blue curve) and after UV-A irra-
irradiation at 3 mW/cm2 (green curve). After CXL, the corneal
diation at 10 mW/cm2 (green curve). After UV-A irradiation there
scattering signal is still saturated, with the exception of the in-
was a residual signal of corneal scattering with respect to the base
termediate stroma more than 150 microns.
line demonstrating that the quantity of riboflavin diffused in the
stroma by means of iontophoresis is more than adequate for an
efficacious treatment with I-CXL.
The standard CXL procedure has been shown to impregnate the stroma with an elevated quantity of riboflavin, however,
a part of which is not used during irradiation (Fig. 9). The study also demonstrated how the epithelium, during the CXL
iontophoresis treatment, absorbs only 16-18% of the UV-A irradiation.
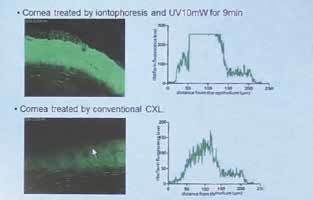
DOES THE TECHNIQUE GUARANTEE AN EFFICACIES APOPTOSIS OF THE
KERATOCYTES? IS IT SAFE FOR THE ENDOTHELIUM?
The studies carried out at the Ophthalmological Clinic of the University of
Florence (Mencucci et al.) showed, on human corneas ex vivo, how CXL
treatment by means of corneal iontophoresis + UV- A irradiation at 10
mW/cm2 causes an efficacious apoptosis of the keratocytes in the corneal
stroma for at least 250 microns, greater than that obtained with ionto-
phoresis + UV- irradiation A at 3 mW/cm2 (Fig. 10). No corneas showed
signs of fibrosis. There was no epithelial damage and no alteration of the
nerve fibers. The conclusions of the study were that corneal iontophoresis
applied to cross-linking can be considered an efficacious technique for im-
proving the penetration of riboflavin into the corneal stroma and that the
energy intensity of 10 mW/cm2 is safe for irradiated tissue.
Fig.10 The Group treated with iontophoresis and irradiation
a 10 mW/cm2 (Group 2) shows clear signs of apoptosis of the
keratocytes, greater than those from the treatment with ionto-
phoresis + UV-A at 3 mW (Group 1). The iontophoresis without
UV-A irradiation (Group 3) does not cause stromal effects.
CORNEAL IONTOPHORESIS
CLINICAL EVIDENCE
The mid-term results (12-18 months) available in scientific literature (Bikbova et al., Acta Oftalmologica; Vinciguerra
et al., JRS; Mastropasqua et al., EUCORNEA and ESCRS Congress 2014) show how iontophoresis is an efficacious
technique in stabilizing progressive keratoconus (reduction of Kmax, no variation in corneal thickness in the follow-up
period) with a moderate inflammatory activation and no cases of haze in the treated patients.
CORNEAL IONTOPHORESIS
Transepithelial corneal cross-linking with imbibition
by means of iontophoresis: preliminary clinical results
1Paolo Vinciguerra, 2J. Bradley Randleman, 3Vito Romano, 1Emanuela F. Legrottaglie,
1Pietro Rosetta, 1Fabrizio I. Camesasca, 1Raffaele Piscopo, 4Claudio Azzolini, MD, 1,4 Riccardo Vinciguerra
1 Istituto Clinico Humanitas, Rozzano, Milano
2 Department of Ophthalmology, Emory University, Atlanta, Georgia (JBR);
3 Dipartimento di oftalmologia, Seconda Università di Napoli
4 Dipartimento di Chirurgia e Scienze Morfologiche, Sezione di Oftalmologia, Scuola di medicina, Università dell'Insubria, Varese
Published in
Journal of Refractive Surgery, 2014
Aim of the study
Report the preliminary clinical results of transepithelial corneal cross-linking with Iontophoresis (I-CXL).
We included in the clinical study (prospective non randomized) 20 eyes of 20 patients with diagnosis of progressive
keratoconus who had undergone I-CXL.
We evaluated pre-operatorially and after 1, 3, 6, and 12 months from treatment: corrected distance visual acuity
(CDVA), spherical equivalent and cylindrical refraction, topographic and tomographic (Scheimpflug) parameters,
aberrometry, OCT of the anterior segment, and endothelial cell count.
The CDVA improved in a statistically significant way at 3, 6, and 12 months after treatment (difference of -0.07 ±
0.01 logMAR, -0.09 ± 0.03 logMAR, and -0.12 ± 0.06 logMAR, respectively; p< 0.05). Even if the aberrometric values
and all the topographic parameters (including Kmax) remained stable in the follow-up period, there was a tendency
towards improvement (without being statistically significant). The corneal thickness did not vary over the 12 months
of observation. The endothelial cell count did not vary in a statistically significant way (p>0.05).
None of the patients showed progression of keratoconus.
The preliminary results at one year from treatment show the efficacy of I-CXL in stabilizing the progression of kerato-
conus, with a significant improvement of the CDVA.
I-CXL, a technique that spares the corneal epithelium, could potentially be a valid therapeutic option to arrest the
progression of keratoconus, with the benefit of reducing pain, risk of infection and the duration of treatment.
The efficacy of the treatment in the long-term still needs to be confirmed compared to the standard EPI-OFF technique.
CORNEAL IONTOPHORESIS
Transepithelial corneal cross-linking with imbibition
by means of iontophoresis: preliminary clinical results
1Paolo Vinciguerra, 2J. Bradley Randleman, 3Vito Romano, 1Emanuela F. Legrottaglie,
1Pietro Rosetta, 1Fabrizio I. Camesasca, 1Raffaele Piscopo, 4Claudio Azzolini, MD, 1,4 Riccardo Vinciguerra
1 Istituto Clinico Humanitas, Rozzano, Milano
2 Department of Ophthalmology, Emory University, Atlanta, Georgia (JBR);
3 Dipartimento di oftalmologia, Seconda Università di Napoli
4 Dipartimento di Chirurgia e Scienze Morfologiche, Sezione di Oftalmologia, Scuola di medicina, Università dell'Insubria, Varese
Fig.1 Variation of corrected distance visual acuity (CDVA) in the follow-up pe-
Fig. 2 Variation of max keratometry (Kmax) in the follow-up period (12
riod (12 months). The CDVA shows a significant increase at 3, 6 and 12 months
months). Kmax shows a statistically significant increase, 1 month after tre-
and a not significant increase at 1 month.
atment, followed by a progressive decrease in the following follow-up period, even if not reaching statistical significance.
Fig. 3 Variation of the chromatic aberration in the follow-up period (12 months).
Fig. 4 Variation of the corneal pachymetry (thinnest point) in the follow-up
The COMA shows a tendency towards improvement, without reaching statistical
period (12 months). The pre-operatory values (434.3 ± 37.8 μm) remained
stable for all the follow-up period.
Correspondence: Paolo Vinciguerra, MD, Istituto Clinico Humanitas, Rozzano (MI)
CORNEAL IONTOPHORESIS
Corneal cross-linking with iontophoresis: clinical
and morphological results at 18 months
L. Mastropasqua, M. Nubile, M. Lanzini, R. Calienno
Presented at the
Scienze of the Visione dell'Università of the Studi of Chieti-Pescara, Chieti
V EUCORNEA Congress
London 12-13 September 2014
Aim of the study
Investigate, on patients affected by progressive keratoconus, the clinical and morphological modifications after
I-CXL that includes an imbibition by means of corneal iontophoresis (5 minutes) and successive exposure to a UV-A
source at 10 mW/cm2 for 9 minutes.
Prospective study carried out on 35 corneas of 35 patients, affected by progressive keratoconus having undergone I-CXL.
We evaluated natural uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA), the topographic para-
meters (Kmax, Penta-cam), corneal pachymetry (thinnest point), the corneal modifications (Laser Scanning IVCM), the
biomechanical variations of the cornea (Corvis). Follow-up: 1 day, 7 days, 1, 3, 6 , 12 and 18 months after treatment.
UCVA and BCVA respectively went from 1.77 LogMAR (pre-operatory data) to 1.69 LogMAR (18 months) and from 0.2
LogMAR to 0.13 LogMAR (p>0.05). The Kmax decreased in a statistically significant way from 58.81 (pre-operatory)
to 50.2 (18 months).
The pachymetric values (thinnest point) remained the same (from 449 um to 452 uni).
The in vivo confocal microscope (IVCM) showed no alteration in the of the nerve fibers, neither modifications in their
density or endothelial damage. In the treated patients a moderate stromal edema and a slight inflammatory activa-
tion were seen. The deformation amplitude index (Corvis) showed, in the follow-up period, a progressive increase of
structural resistance in the corneas treated with I-CXL with respect to the pre-operatory period.
The intraocular pressure, the endothelial cell count, the transparency of the crystalline and the ocular fundus show-
ed no variation after 6 months from treatment with respect to the pre-operatory period.
The I-CXL treatment demonstrated to be a safe and efficacious technique in arresting the progression of keratoconus,
documented not only by clinical experience, but also by basic research, without any relevant adverse effects.
CORNEAL IONTOPHORESIS
Corneal cross-linking with iontophoresis:
clinical and morphological results at 18 monthsL. Mastropasqua, M. Nubile, M. Lanzini, R. Calienno
Scienze of the Visione dell'Università of the Studi of Chieti-Pescara, Chieti
Fig. 1 Variations of uncorrected visual acuity (UCAV) and best-corrected visual acuity (BCVA) in the follow-up period.
Fig. 2 Variations of Kmax and the thinnest point in the follow-up period.
Correspondence: Manuela Lanzini, MD-PhD, Università degli Studi di Chieti-Pescara, Chieti
CORNEAL IONTOPHORESIS
Cross-linking by means of iontophoresis:
6 months of follow-up with SD-OCT. Pilot study
G. Prosdocimo, G. Capello
Ospedale De Gironcoli, Conegliano Veneto (TV)
XXXII ESCRS Congress
London 13-17 September 2014
Aim of the study
To evaluate the efficacy of the new technique of transepithelial corneal cross-linking by means of iontophoresis (I-CXL) to incre-
ase the penetration of riboflavin through the intact epithelium in the treatment of progressive keratoconus.
Prospective study carried out on 19 eyes of 18 patients affected by progressive keratoconus (stage I-III according to the classi-
fication of Krumeich). The I-CXL treatment was carried out after topical anesthesia and the corneas were soaked with a formu-
lation based on riboflavin 0.1% without dextran neither sodium chloride (RICROLIN®+, SOOFT Italia S.p.A) using a system for
corneal iontophoresis (I-ON CXL®) for allow a rapid and uniform passage into stroma through the intact epithelium. The time
of imbibition was 5 minutes, while that of UV-A irradiation (10 mW/cm2) was 9 minutes. For all the follow-up period (1, 3 and
6 months) we evaluated: visual acuity, topographic parameters, the pachymetry (CASIA SD OCT) and endothelial cell count.
Best-spectacle corrected acuity visual (BSCVA) improved from 0.198 ± 0.703 LogMAR up to 0.165 ± 0.667 LogMAR.
The analysis of the topographic data of the eyes treated showed a stabilization of the average keratometry (Kave) 6 months
after the treatment (baseline: 46.52 ± 3.37 D; 6 months: 46.56 ± 3.49 D) and of the average posterior keratometry (baseline:
-6.73 ± 0.73 D; 6 months: -6.73 ± 0.72 D). Astigmatism decreased from 2.94 ± 1.39 D to 2.71 ± 1.16 D.
The pachymetric values (thinnest point) were unvaried (from 465 ± 39.73 to 463 ± 40.95 um). The intraocular pressure, the
endothelial cell count, the transparency of the crystalline and the ocular fundus showed no variations after 6 months from
treatment with respect to the pre-operatory period.
The treatment with I-CXL has shown that it is able to improve the BSCVA and stabilize the K readings for all the follow-up period.
Iontophoresis is a safe procedure and seems able to arrest the progression of keratoconus thanks to an optimal intrastromal
diffusion of riboflavin through the intact epithelium. The advantage of the iontophoretic technique is the capacity to combine
the efficacy of the standard EPI-OFF technique with absence of adverse effectstypical of the EPI-ON technique.
CORNEAL IONTOPHORESIS
Cross-linking by means of iontophoresis:
6 months of follow-up with SD-OCT. Pilot study
G. Prosdocimo, G. Capello
Ospedale De Gironcoli, Conegliano Veneto (TV)
Fig.1 Variations of the average anterior and posterior keratometry and of the pachymetry in a patient who had undergone I-CXL in June 2013.
The map refers to the pre-treatment acquisition (D), after 4 months (C), 13 months (B) and 15 months (A) from treatment.
The diagrams top right show a reduction of the average anterior keratometry (0.8 D) and a stabilization of pachymetric data.
The differential map top left shows a notable reduction of Kmax of 2.6 D.
The parameters were evaluated with CASIA SD OCT.
Correspondence: Gianluca Capello, MD, Ospedale De Gironcoli, Conegliano Veneto, (TV)
CORNEAL IONTOPHORESIS
Demarcation Line Evaluation of Iontophoresis-
Assisted Transepithelial Corneal Collagen
Cross-linking for Keratoconus
Samantha Bonnel, MD; Marouen Berguiga, MD; Benoit De Rivoyre, JD; Gabriel Bedubourg, MD;
Damien Sendon, MD; Françoise Froussart-Maille, MD, MSc; Jean-Claude Rigal-Sastourne, MD, MSc
Published in
Journal of Refractive Surgery, 2015
Aim of the study
To evaluate the visualization and depth of the demarcation line with anterior segment optical coherence tomography (AS-OCT)
after iontophoresisassisted transepithelial corneal collagen cross-linking (CXL).
This prospective, consecutive, single center, non-randomized clinical study involved 15 eyes of 12 patients with keratoconus
who underwent an AS-OCT scan (Spectralis; Heidelberg Engineering, Inc., Carlsbad, CA) to search for a demarcation line and its
depth at 1 month after iontophoresis-assisted transepithelial CXL. AS-OCT scan measurements were performed by two inde-
pendent examiners.
No intraoperative or postoperative complications were observed. Kappa coefficient estimation foroperator agreement in de-
marcation line visualization (whether it was visualized) was 70.6%. The corneal stromal demarcation line was identified in 9
eyes (60%) by both examiners. Mean depth of the corneal stromal demarcation line was 246.67 ± 50.72 μm (range: 183 to 339
μm) for the first examiner and 241.89 ± 62.52 μm (range: 163 to 358 μm) for the second examiner. There were no statistically
significant differences for the measurements of the paired comparisons between the two examiners (P = .61). The Pearson
correlation coefficient between the measurements was 0.910.
Iontophoresis-assisted transepithelial CXL creates a demarcation line that can be visualized with AS-OCT, which seems less
easily distinguishable and shallower than in conventional CXL. However, its depth and visualization seems to be more similar to
conventional CXL than transepithelial CXL.
CORNEAL IONTOPHORESIS
Demarcation Line Evaluation of Iontophoresis-
Assisted Transepithelial Corneal Collagen
Cross-linking for Keratoconus
Samantha Bonnel, MD; Marouen Berguiga, MD; Benoit De Rivoyre, JD; Gabriel Bedubourg, MD;
Damien Sendon, MD; Françoise Froussart-Maille, MD, MSc; Jean-Claude Rigal-Sastourne, MD, MSc
Fig.1 High-resolution corneal anterior segment optical coherence tomography
Fig. 2 High-resolution corneal anterior segment optical coherence tomo-
scan visualizing the corneal stromal demarcation line at a depth of 218 μm at
graphy scan with a disagreement on visualizing the corneal stromal demarca-
1 month after iontophoresis-assisted transepithelial corneal collagen cross-
tion line 1 month after iontophoresis-assisted transepithelial corneal collagen
crosslinking. The corneal stromal demarcation line is not visualized by the the (A) first examiner, whereas the (B) second examiner noticed a line at a depth of 270 μm.
CORNEAL IONTOPHORESIS
Transepithelial corneal cross-linking with
iontophoresis in pediatric patients. Preliminary results
L. Buzzonetti, G. Petrocelli
Ospedale pediatrico IRCCS Bambino Gesù, Roma
Presented at the
CORNEAL CROSS-LINKING
Up to Date
Rome, 20 September 2014
Aim of the study
Evaluate the efficacy of transepithelial corneal cross-linking with iontophoresis (I-CXL) in the stabilization of
progressive keratoconus in pediatric patients.
Thirteen eyes from 8 pediatric age patients (average age: 13±2.9 years; range: 10-18 years) were treated with
transepithelial corneal cross-linking by means of iontophoresis of riboflavin. The procedure began with 5 minutes
of imbibition with RICROLIN®+ by means of IONTOforCXL® applicator, specific for corneal iontophoresis, and
then UV-A irradiation at 10 mW/cm2 for 9 minutes.
The patients, pre-operatively and after 3, 6 and 12 months from treatment, underwent the following examinations:
DCVA (Distance Corrected Visual Acuity); corneal topography: Kmax, Kmin, Kavg; corneal aberrometry: COMA,
spherical aberration and high order aberrations (HOAs) for a pupil diameter of 5.0 mm; pachymetry (thinnest
point); endothelial cell count.
Visual acuity DCVA improved in the 12 months of follow-up, passing from a value of 0.7±0.1 (pre-operatory) to
0.7±0.1 (3 months, p=0.04), to 0.8±0.2 (6 months, p=0.06), to 0.8±0.2 (12 months, p=0.07).
One year after treatment, the topographic and aberrometric parameters showed no significant variations (p>0.05).
The thinnest point (average pre-operatory value: 485 um; average value after 12 months of follow-up: 483 um) and
the density of the endothelial cell count (average pre-operatory value: 2962±214 cells/mm2; average value after 12
months of follow-up: 2940±241 cells/mm2) were stable in the follow-up period (p=0.01 and 0.09, respectively).
OCT analysis showed a not homogeneous hyper-reflective band but deep in the first 180 μm of the cornea. There were
no post-operative complications.
Our preliminary results on pediatric patients appear to be promising, even if they have to be confirmed by studies on
a greater cohort and with a longer follow-up.
LA IONTOFORESI CORNEALE
Transepithelial corneal cross-linking with
iontophoresis in pediatric patients. Preliminary results
L. Buzzonetti, G. Petrocelli
Ospedale Pediatrico IRCCS Bambino Gesù, Roma
Table 1 Values of Distance Corrected Visual Acuity (DCVA), spherical equivalence and refractive astigmatism measured at baseline and after 3, 6 and
12 months from treatment with I-CXL.
Table 2 Topographic and aberrometric data measured at baseline and after 3, 6 and 12 months from I-CXL treatment.
Correspondence: Luca Buzzonetti, MD, Ospedale Pediatrico IRCCS Bambino Gesù, Roma
CORNEAL IONTOPHORESIS
Transepithelial corneal cross-linking by means
of iontophoresis in the treatment of progressive keratoconus
in pediatric patients: one-year follow-up
F. Montrone, L. Lapenna
Ospedale Di Venere, Bari
XXXII ESCRS Congress
London 13-17 September 2014
Aim of the study
To verify the efficacy of transepithelial corneal cross-linking by means of the iontophoresis of riboflavin (I-CXL) in
patients under 18 years old affected by progressive keratoconus.
Materials and methods
The treatment with I-CXL was carried out on 11 eyes of 7 patients affected by progressive keratoconus (stage II-III
according to the classification of Amsler-Krumeich). Average age was 15±2.6 years. All the patients had pachymetric
values above 400 microns (thinnest point). Corneal impregnation was carried out by means of a solution of hypotonic
riboflavin, specific for corneal iontophoresis (RICROLIN®+), administered for 5 minutes by means of a special device
(IONTOforCXL®). The cornea was then irradiated with ultraviolet light at 10 mW/cm2 for 9 minutes. The following were
measured at baseline and at 1, 3, 6 and 12 months: uncorrected visual acuity (UCVA) and best spectacle corrected
visual acuity (BSCVA), spherical equivalent, central corneal thickness and the Kmax.
Results
The average value of the UCVA and the BSCVA at one year had improved in a statistically significant way by 56.6% and
48.5%, respectively. None of the patients lost lines in BSCVA. Spherical equivalent showed, at 12 months from tre-
atment, a decrease of 1 D (average value, p>0.05). I Kmax is diminuito of 0.7 D after 1 anno of follow-up. The central
corneal thickness was the same. There were no reports of pain or adverse events. The endothelial cell count did not
vary in a statistically significant way (3164.6±25.7 cells/mm2).
Conclusions
The treatment with I-CXL appears to be safe and efficacious in the treatment of progressive keratoconus in pediatric
patients. Further long-term studies are needed to establish a more complete profile of safety and efficacy of the tech-
nique for this new and promising technique of cross-linking.
LA IONTOFORESI CORNEALE
CORNEAL IONTOPHORESIS
Transepithelial corneal cross-linking by means
of iontophoresis in the treatment of progressive
keratoconus in pediatric patients: one-year follow-up
F. Montrone, L. Lapenna
Ospedale Di Venere, Bari
Corneal topography (Anterior)
Corneal topography (Anterior)
12 m post CXL
Fig. 1 Male patient (12 years old) affected by Down Syndrome with progressive keratoconus. Topographic evaluation pre-operatory and at 12 months
after CXL with iontophoresis. The topographies show a clear stabilization of the ectasia.
Corneal topography (Anterior)
Corneal topography (Anterior)
12 m post CXL
Fig. 2 Male patient (15 years old) with progressive keratoconus.
Topographic evaluation pre-operatory and at 12 months after CXL with iontophoresis. The topographies show a reduction of Kmax from
61.8 D to 60.2 Dreduction of Kmax from 61.8 D to 60.2 D.
Correspondence: Lucia Lapenna, MD, Ospedale Di Venere, Bari
CORNEAL IONTOPHORESIS
Transepithelial corneal collagen cross-linking by iontophoresis of riboflavin.
12 m post CXL
Bikbova G, Bikbov M.
Acta Ophthalmol. 2014 Feb;92(1):e30-4
Corneal cross-linking: intrastromal riboflavin concentration in iontophoresis-assisted imbibition versus tradi-
tional and transepithelial techniques.
Mastropasqua L, Nubile M, Calienno R, Mattei PA, Pedrotti E, Salgari N, Mastropasqua R, Lanzini M.
Am J Ophthalmol. 2014 Mar;157(3):623-30
Iontophoresis transcorneal delivery technique for transepithelial corneal collagen crosslinking with ribofla-
vin in a rabbit model.
Cassagne M, Laurent C, Rodrigues M, Galinier A, Spoerl E, Galiacy SD, Soler V, Fournié P, Malecaze F.
Invest Ophthalmol Vis Sci. 2014 Mar 18
Structural modifications and tissue response after standard epi-off and iontophoretic corneal crosslinking
with different irradiation procedures.
Mastropasqua L, Lanzini M, Curcio C, Calienno R, Mastropasqua R, Colasante M, Mastropasqua A, Nubile M.
Invest Ophthalmol Vis Sci. 2014 Apr 17;55(4):2526-33
Biomechanical changes in the human cornea after transepithelial corneal crosslinking using iontophoresis.
Lombardo M, Serrao S, Rosati M, Ducoli P, Lombardo G.
J Cataract Refract Surg. 2014 Oct;40(10):1706-15
12 m post CXL
CORNEAL IONTOPHORESIS
CORNEAL IONTOPHORESIS
CORNEAL IONTOPHORESIS
CORNEAL IONTOPHORESIS
EXPERIMENTAL EVIDENCE
CLINICAL EVIDENCE
CORNEAL IONTOPHORESIS
EXPERIMENTAL EVIDENCE
CLINICAL EVIDENCE
Source: http://www.medcon.gr/wp-content/uploads/2015/02/OPUSCOLO-Iontoforesi-INGLESE-09-03-15.pdf
DIABETES MELLITUS Understanding Type 1 and Type 2 Diabetes and Disease Progression Buge Apampa PhD MRPharmS Some Questions to start off! 1. How many people are expected to have diabetes in the UK by 2025? [5m] 2. What is the estimated hourly cost of diabetes to 3. How many diabetic patients are dying avoidably each year? [24,000]
> Accueil > Actualité > Le magazine > Troubles obsessionnels compulsifs Actualité Le magazine Troubles obsessionnels compulsifs La vie est un " enfer " pour 2 à 3 % des Français atteints de Les Urgences troubles obsessionnels compulsifs (Toc), maladie loin d'être rare

