The dementia epidemic: economic impact and positive solutions for australia
THE DEMENTIA EPIDEMIC: ECONOMIC IMPACT
AND POSITIVE SOLUTIONS FOR AUSTRALIA
ALZHEIMER'S AUSTRALIA
Disclaimer and Acknowledgements
This report was prepared by Access Economics for Alzheimer's Australia, funded by an unrestricted grant from Janssen-Cilag and Pfizer who had no part in the direction or findings contained in this report. Access Economics would like to acknowledge with appreciation the comments, previous research and expert input from:
Professor Henry Brodaty
Academic Department for Old Age Psychiatry, University of New South Wales Euroa Centre, Prince of Wales Hospital
Ms Anne Eayrs
National Policy Officer, Alzheimer's Australia
Mr Richard Gray
Director Aged Care Services, Catholic Health Australia
Dr Anna Howe
Consultant
Professor Anthony Jorm
Director, Centre for Mental Health Research, Australian National University
Mr Lewis Kaplan
Chief Executive Officer, Alzheimer's Australia New South Wales
Ms Lynette Moore
Executive Director, Alzheimer's Australia Victoria
Ms Virginia Moore
Dementia Services Consultant, Brightwater Care Group, Western Australia
Mr Alan Nankivell
Executive Director, Alzheimer's Australia South Australia
Mr Glenn Rees
National Executive Director, Alzheimer's Australia
Ms Barbara Squires
Director, Centre of Ageing, Benevolent Society
Dr Michael Woodward
Director, Aged and Residential Care, Austin and Repatriation Medical Centre
Dr Robert Yeoh
President, Alzheimer's Australia
The analogy of the receding tide on piii is drawn from Jorm (2001), paraphrased, in turn drawn from
Gavin Andrews (St Vincent's Hospital, Sydney). Photo from www.williamjosephgallery.com. The fifth epidemiological transition is detailed in Broe (2002).
While every effort has been made to ensure the accuracy of this document, the uncertain nature of
economic data, forecasting and analysis means that Access Economics Pty Ltd is unable to make
any warranties in relation to the information contained herein. Access Economics Pty Ltd, its employees and agents disclaim liability for any loss or damage which may arise as a consequence of
any person relying on the information contained in this document.
Alzheimer's Australia, 2003.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
CONTENTS
EXECUTIVE SUMMARY. IV
DEMENTIA – THE EXTENT OF THE EPIDEMIC . 1
EPIDEMIOLOGY AND AETIOLOGY.1
1.1.1 Diagnosis . 1
1.1.2 Types of dementia. 3
1.1.3 Aetiology . 7
1.1.4 Mortality. 9
TREATMENT AND MANAGEMENT .10
1.2.1 Quality of care . 10
1.2.2 Prevention and early diagnosis . 13
1.2.3 Pharmacological management. 15
1.2.4 Natural / alternative treatments . 18
1.2.5 Other medical and surgical interventions . 19
1.2.6 Psycho-social interventions. 20
1.2.7 Caring for families and carers. 24
1.2.8 Care in the community . 25
1.2.9 Residential Care. 28
1.3.1 Worldwide prevalence. 31
1.3.2 Current prevalence in Australia . 31
1.3.3 Projected prevalence in Australia. 32
HEALTH AND SOCIOECONOMIC IMPACTS IN AUSTRALIA .33
1.4.1 Disability. 33
1.4.2 Socio-economic status and rurality. 33
1.4.3 Employment . 34
1.4.4 Use of medical services . 34
1.5 INTERNATIONAL COMPARISONS.35
1.5.1 North America . 36
1.5.2 Europe. 38
SUMMARY OF CHAPTER ONE.39
THE DEMENTIA BURDEN FOR AUSTRALIAN PEOPLE . 42
DIRECT HEALTH COSTS .42
2.1.1 Direct costs in 1993-94 and 2002. 42
2.1.2 Projections of direct costs . 44
2.1.3 Home and community care costs . 44
INDIRECT FINANCIAL COSTS.45
2.2.1 Lower workforce participation of people with dementia . 45
2.2.2 Family and carer costs . 46
2.2.3 Cost of welfare payments. 48
2.2.4 Modifications and aids. 48
2.2.5 Summary of financial costs . 49
THE BURDEN OF DISEASE.50
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
COMPARISONS, CONSTRAINTS AND SCENARIOS. 52
COMPARISONS WITH OTHER DISEASES.52
3.1.1 Comparisons of prevalence. 52
3.1.2 Comparison of financial costs . 53
3.1.3 Comparison of disease burden. 54
CONSTRAINTS TO SERVICE DELIVERY .55
3.2.1 Medical and hospital services. 55
3.2.2 Pharmaceuticals. 56
3.2.3 Research. 57
3.2.4 Home and community care . 58
3.2.5 Residential care. 61
3.2.6 Health financing and cross-cutting access issues . 65
SCENARIO ANALYSIS OF VARIOUS INTERVENTIONS.67
3.3.1 Pharmaceutical interventions . 68
3.3.2 Support for family carers . 73
3.3.3 Research resulting in a ‘cure' . 74
3.3.4 Summary of scenario analysis. 75
OPTIONS AND CHALLENGES . 76
SETTING THE SCENE .76
4.1.1 National Action Plan for Dementia Care. 76
4.1.2 Aged care reforms and the Two Year Review. 77
THE FUTURE VISION .79
STRATEGIES AND RECOMMENDATIONS.80
4.3.1 Prioritisation of dementia. 80
4.3.2 Research. 82
4.3.3 Prevention and early intervention activities . 82
4.3.4 General practice. 83
4.3.5 Other medical and acute care services . 83
4.3.6 Pharmacotherapy. 83
4.3.7 Home and community support services . 84
4.3.8 Families and carers. 84
4.3.9 Strengthening community services provided though Alzheimer's Australia. 85
4.3.10 Residential care. 85
4.3.11 Cross-cutting issues. 86
4.3.12 Health financing. 87
METHODOLOGY. 88
BRODATY TRIANGLE . 93
GLOSSARY OF COMMON ABBREVIATIONS . 94
REFERENCES. 96

The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
The receding tide
The next epidemiological transition
A century ago, Australia's birth rate was much higher, but few people survived to old age. With better
sanitation, the dangers of the past – infectious diseases and childbirth – became far less serious threats
to our health. As the tide of infectious diseases receded, the rocks that were always there were
exposed – systemic degenerative diseases such as cardiovascular disease and cancer. But, gradually,
even these problems are receding as we see the benefits of prevention programs and the better
treatments possible with new technologies, particularly new surgeries and drugs. As the tide recedes
further, the new rocks to be revealed are the neuro-degenerative diseases that strike the brain most
often in old age. It is predicted that the neurodegenerative disorders will over the next two decades
replace the systemic disorders as the major causes of both death and disability. Managing the
challenges presented by these diseases, most notably dementia, will be the overwhelming priority of
health care in the 21st century.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
EXECUTIVE SUMMARY
Australia needs to move towards more positive public awareness of dementia, encouraging the
community to view this disabling condition with more optimism and hope. We have a long way to go in understanding its causes and best treatment practices. Managing the dementia epidemic presents huge
and growing challenges in terms of prevalence, costs and burden of disease. However, with appropriate research, funding and prioritised coordinated strategies for home-based, community and residential
care, it is possible to minimise these burdens, enhance the quality of life of many Australians with dementia and their families and carers, and move forward this century with world class models of care
and prevention, until a cure is found.
The dementia epidemic has arrived. In Australia there were over 162,000 people with dementia in 2002,
including 6,600 under 65 – with ‘younger onset' dementia.
□ The prevalence of dementia is growing rapidly – reaching the 500,000 mark around 2040. □ Dementia is more common than skin cancer, yet with significantly less investment in public health
In Australia, dementia already costs $6.6 billion - $5.6bn in real economic costs and $1bn in transfer
costs.
□ Direct health costs: Dementia is the most expensive mental health item in Australia, costing
$3.2 billion in 2002, dominated by residential care costs ($2.9 billion). By the end of the decade,
these costs will nearly double. In addition, home and community care costs are also rising steeply; currently $175m of Federal community services program money is spent on people with dementia.
□ Real indirect costs: These are dominated by carer costs ($1.7 billion) valued at replacement cost,
together with the lost earnings and mortality burden of patients ($364m) and the cost of aids and
home modifications ($120m).
□ Transfer costs: $592m of tax is foregone each year for people with dementia and their families and
carers. Carer payments represent another $324m, while additional welfare payments total $52m.
o By mid-century, dementia costs may exceed 3% of GDP, from nearly 1% today.
The socio-economic and disability burden of dementia is severe.
□ 98.5% of people with dementia are disabled and use medical services more than the age-average. □ People with dementia have lower than average incomes and are under-represented in the
workforce – 2.3% compared to the Australian average of 8.5% for people over age 65.
□ Dementia cost over 117,000 years of healthy life (disability adjusted life years or DALYs) in 2002,
and severe dementia has the highest disability weight of all conditions, equal with severe
rheumatoid arthritis and higher than terminal stage cancer.
□ Dementia is the second largest cause of disability burden in Australia after depression, and will
become the largest by 2016, continuing to outpace other chronic illnesses.
Dementia costs more years of healthspan than any of the national health priority areas.
Strangely, the enormity and priority of the dementia epidemic have not yet been acknowledged in
national policy making. Dementia has links to recognised national health priorities including
cardiovascular disease, diabetes and depression, and it is the mostly costly area of mental health. A national strategy to realise the vision, is long overdue.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
A national strategy must address current constraints to delivery of services for dementia, including:
□ General practitioners (GPs) are generally poor at diagnosing dementia and could be assisted
through greater access to specialists services (eg, memory clinics) and education and training
programs, which could assist in diagnosis and ongoing support and management. Early diagnosis means the person and the family benefit from drug treatments, support and planning.
□ Acute care: Average length of stay (ALOS) is prolonged and there is a lack of understanding about
dementia in acute facilities, which could be addressed through broad-based training and awareness
programs, as well as capital needs such as dementia-friendly and secure environments.
□ Early access to cholinesterase inhibitor (CEI) drugs through the Pharmaceutical Benefits
Scheme (PBS) is impeded by an overly rigid definition of acceptable benefit, the exclusion of people with non-Alzheimer dementia, and a cost-cutting approach that ignores the economy-wide benefits
of pharmacotherapy as investment in wellness.
o Comparative static cost-benefit analysis across the whole population of people with dementia
shows that, by deferring institutionalisation for one year and delaying progression of illness, cholinesterase inhibitors can save up to $49,219 per entry avoided (a 7:1 return on investment)
plus a 13% increase in healthspan.
□ Research is severely underfunded, yet there is scope for huge savings from investment in research
for cause, prevention and care.
o $1 is spent on research for each $342 of the total costs of dementia (0.29%).
□ Despite welcome growth in home and community services, there remains unmet need resulting
from barriers to access that would be eased by continued additional funding in each of the major
programs. The lack of dementia-specific expertise needs to be addressed.
□ In terms of support for families and carers, new innovative models should be implemented, in
particular for respite care. Often the respite care that is available is inappropriate for people with dementia, and as a consequence there is a sub-optimal take-up rate (64%) of residential respite
places. There need to be incentives to encourage increased employment participation for families and carers.
□ There is a need for substantially expanded dementia and person-centred care education and
training across the care sector, for families and carers and care workers. New models of care need
to be trialled and utilised.
□ Better use could be made of the services of cost-effective community organisations such as Carer
Associations and, in particular, Alzheimer's Associations, which are limited due to funding
constraints. Additional funding is required for programs such as the Dementia Education Support
Program (DESP), the Early Stage Dementia Support and Respite Program (ESDSRP) and the Carer Education Workforce and Training (CEWT) project to deepen penetration rates and ease
□ Within existing residential care, there are multiple issues. Some of these include:
o the descriptors in the Resident Classification Scale (RCS) currently do not accord well with
assessments of Aged Care Assessment Teams (ACATs) or with appropriate placement of
people with dementia, and need to include behaviour and environmental aspects;
o sustainable pricing needs to be addressed within the context of the current federal Residential
Aged Care Pricing Review, in particular capital costs for high care and recurrent costs for low care facilities;
o current staff-to-resident ratios, staff training and nursing and care staff remuneration appear
inadequate for quality dementia care;
o firmer accreditation and monitoring of standards are required with tighter restrictions placed on
chemical and physical restraint practices and more emphasis on person-centred care;
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
o planning ratios do not make provision for dementia-specific care;
o better access to appropriate care is required for people with dementia with serious psychiatric
symptoms, as well as those with serious mental health problems who develop dementia;
o cluster housing campus models are needed that can cater well for a range of different needs as
a person ages, with facilities appropriate to various ‘groups' (eg, people with younger onset
dementia for whom co-residence with older people is inappropriate) and various stages of dementia.
□ Access for different groups of people with special needs must be addressed, including:
o people with younger onset dementia;
o people from culturally and linguistically diverse backgrounds;
o indigenous people; and
o people in rural and remote areas, including better use of new information technologies in
delivering services.
□ Long term intergenerational planning including better insurance or savings vehicles is needed to
finance future growth in dementia prevalence, care and costs.
A national vision is needed which acknowledges the challenges of the dementia epidemic, and that
responds with a broadly scoped and positive agenda for future action to meet those challenges. A key premise of the vision is a commitment to increasing healthspan for Australians with dementia through
prevention, care and cure. This commitment must come from all stakeholders though a nationally
coordinated strategy. Quality chronic care models must be utilised to maximise returns from health
resources that are becoming increasingly scarce as the demographic transition proceeds. Dementia
must be prioritised.
□ At present, although significant sums are spent on dementia care through the aged care system,
there remains inadequate recognition of and planning for the special needs of dementia care in
mainstream community and residential care. Strategic coordination of dementia does not fit completely comfortably within either the aged care or mental health portfolios.
□ Whatever decision is taken on the most effective point of coordination, it is clear that a whole of
government approach is needed. This is because dementia care is so broad ranging, covering
aspects of aged care, community care, residential care, medical services, psychiatric and specialist services, pharmaceuticals, workforce and housing.
Apart from prioritisation, five pillars of a future national strategy for dementia should involve:
1) a significant investment in research for cause, prevention and care; 2) early intervention through improvement in diagnosis, and the provision of cost-effective
pharmacotherapies;
3) comprehensive provision of support, education and respite services – in place in the
community as far as is optimal;
4) quality residential care, appropriately financed, that are centred on the person with dementia
and their family/carer; and
5) provision for special needs, including people with younger onset dementia, people with
behavioural and psychological symptoms of dementia (BPSD), people from culturally and linguistically diverse backgrounds, indigenous Australians and people in rural and remote
Detailed strategies and recommendations are provided in Section 4.3.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
If, starting today, we embark on such positive strategies, Australia can lead the way in effectively and
smoothly managing the dementia epidemic. Advances in medical science cannot be predicted but the probability is that the total costs of dementia care will rise significantly to the middle of this century to 3% of GDP given the demographic ageing of
the population. However, the current returns from expenditures on medication and carer support can be expected to reduce the total costs to government substantially below what they might otherwise have
been, through delays in admission to residential care. Every year residential care is delayed saves the Government $30,632 per entry avoided. And the quality of life of people with dementia, their families
and carers will be enhanced through these interventions. It is for these reasons we have to tackle the constraints to services and invest in research.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1. DEMENTIA – THE EXTENT OF THE EPIDEMIC
1.1 EPIDEMIOLOGY AND AETIOLOGY
Dementia is a progressive and disabling condition, primarily of older persons, that can bring turmoil and
anguish to those involved. The progression of dementia over many years is often categorised as mild (early stage), moderate (middle stage) and severe or advanced (late stage), before the person dies.
Different people may have different symptoms at various times, depending on the parts of the brain affected and the characteristics of each individual. That said, symptoms can be broadly classified
(Burns, 2001) as:
1. Cognitive impairment: Symptoms include problems with memory (amnesia), speech or
understanding of language (aphasia), a failure to carry out physical tasks despite having intact motor function (apraxia), and failure to recognise objects or people despite having knowledge of
their characteristics (agnosia).
2. Psychiatric and behavioural features: There may also be any of a range of psychiatric symptoms
– such as depression, delusions1, hallucinations (visual and auditory) – and behaviours such as wandering, incessant walking or agitation. A number of behavioural features derive from a person's
response to the confused situation in which they find themselves, such as repetition, following, crying or "confabulating"2.
3. Dysfunction in activities of daily living (ADL): In the early stages of dementia these can take the
form of difficulties with shopping, driving or handling money. In the later stages more basic tasks are
affected such as dressing, eating and bathing.
1.1.1 Diagnosis
There are as yet no known biological markers for dementia, so clinical diagnosis is based on medical
and psychiatric history; neurological and physical examination; tests (mainly blood tests) to rule out
other conditions and record baseline levels of cholesterol etc; a ‘baseline' evaluation of the person's ADL functionality, thinking and memory (such as the widely used Mini-Mental State Examination –
MMSE3 – or Abbreviated Mental Test Score); and a caregiver interview or questionnaire.4 Magnetic resonance imaging (MRI), computed tomography (CT) and positron emission tomography (PET) reveal
any brain atrophy (shrinkage) or evidence of stroke, and distinguish other brain disorders (eg, tumour, bleed) that may be more treatable. Scanning technology involving radiology, electroencephalography,
blood and cerebrospinal fluid may in the future be able to identify characteristic plaques, tangles and
other markers of dementia, formerly identifiable only in autopsy (Alzheimer's Association US, 2002a)5. Genetic testing presents serious ethical implications for families and clinicians (Black et al, 2001 p4, 21).
Black et al (2001) provide a good current summary of diagnostic processes and issues in Australia.
1 Examples are that a carer is ‘trying to poison me", "trying to put me away" or "stealing my money". 2 Confabulating may involve providing an answer that may not be true, but could be, since the real answer is unknown – eg,
"What did they give you for dinner?' Answer: ‘Fish, I hate fish!' Reality: Lamb and vegetables. 3 MMSE tests orientation (time of year and current location), ability to absorb and retain information (delayed recall of the
names of three objects), level of attention, ability to calculate (count backwards from 100 by 7s) and competence in responding to instructions ("Take a piece of paper in your right hand, fold it in half and put it on the floor." MMSE scores are
usually around 18+ for mild illness (maximum is 30), 10-18 for moderate illness and less than 10 for severe illness. It can be
poor at detecting very mild dementia and has biases in relation to education and culture. 4 For example, IQCODE (Informant Questionnaire of Cognitive Deficits in the elderly). 5 A team at the Brigham and Women's Hospital, Boston US, achieved high accuracy in diagnosis of AD with single photon
emission computed tomography – SPECT (Neurology, June 1998). The National Institute of Aging in 2002 reports a powerful
new imaging technique, multiphoton microscopy. Advances with functional MRI are reported in Black et al (2001, p19-20).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Differential diagnosis and assessment by a specialist is important, in particular distinguishing dementia
from "normal" memory and cognitive impairment of ageing, and from other disorders such as delirium, major depression, drug abuse, amnestic disorder, anaemia6 and others. It is also important to
distinguish between the different types of dementia, which can have different features of onset, treatment and progression, often measured by the Clinical Dementia Rating Scale or Alzheimer's
Disease Assessment Scale - Cognitive Subscale (ADAS-Cog). Diagnoses by trained doctors are 80%-90% accurate. Internationally recognised diagnostic criteria for dementia are:
□ DSM-IV: Impairment in memory and at least one of the following: agnosia, apraxia, aphasia or
executive functioning impairment.7 Cognitive deficits are severe enough to interfere with
occupational/social activities and represent a decline from previous level.
□ ICD-10: Decline in both memory and thinking, of a degree sufficient to impair function in daily living.
To tell? And how to tell…
"I don't know if June knew she had Alzheimer's. She may have had an idea because her brother and sister had it. We never sat down and talked about it. Later when I did refer to dementia, it was a bit hard
to know how much she was taking in. I think she felt it was all part of being old. She once said to me that she had retired, like I had."
A survey of 281 GPs in the UK found that only 39% would inform their patients of a diagnosis of
dementia, compared to 95% who would inform them of a diagnosis of terminal cancer (Black et al,
2001). Reasons for not telling include emotional distress and other negative impacts for the person and their family, fear of incorrect diagnosis, a judgement that there is no benefit in the person knowing, or a
request from the family or carer not to tell. However, there is no evidence that this information has long-term negative effects – rather, the diagnosis may help explain confusing symptoms. Moreover, people have a right to know about their own
health, and information is likely to bring the best health outcomes in terms of ability to become informed and supported, to know what to expect, to make plans and strategies for managing the illness and
associated disability, to facilitate access to services including medical treatments and community services, and to enhance the relationships between the person, their families and carers and health
professionals. Indeed, the earlier that these processes begin, the better. In telling a person about a possible diagnosis of dementia, many skills are required. There may be suspicions and questions early on and, before compelling evidence is accumulated, the possibility of
dementia is canvassed. Primary care professionals need to be truthful about what is happening, about the possibility of and reasons for both a correct or incorrect diagnosis, and provide sufficient verbal and
written information and referral so that the person and their family can understand and adjust to the implications and options available. It may be beneficial for the person and a significant family member to
be informed together. Sufficient time should be allowed to respond to emotional reactions, which are likely to include shock and grief that need to be expressed in healthy ways. Compassion needs to be
exercised, a team approach adopted, and written information, support, counselling and referral offered.
6 Other common physical tests include liver and kidney function, vitamin levels in the blood, thyroid function and blood
glucose levels (diabetes). The physical examination may include checking pulse and blood pressure, and for any signs of
stroke, chest or heart abnormalities or abdominal lumps. 7 Executive functioning – the ability to think abstractly, plan, initiate, sequence, monitor and stop complex behaviours. 8 A number of quotes in this document are extracted from personal stories collated in Hampson (2000). Where these are
cited in this document they are sourced to the original storyteller.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.1.2 Types of dementia
There are numerous diseases that cause dementia. A fuller list is provided in Wimo et al (1998, Table
1.1.2, p6). The most common types are outlined below, noting that they can occur together.9
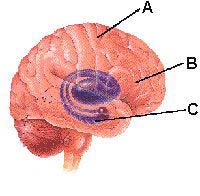
Alzheimer's disease (AD), the most common of the dementia disorders (comprising 50-70% of cases),
is progressive, degenerative and currently incurable. The shrinkage or atrophy of the brain due to nerve
cell loss can be seen during life on a brain scan, as pictured below.
PET scans: Dementia involving AD10
A person with dementia
may appear healthy on
the outside, but on the
inside, irreversible
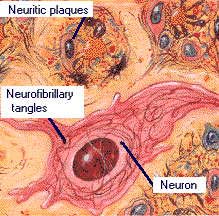
However, it is post-mortem analysis that confirms a diagnosis of AD, due to two key observations:
□ neurofibrillary tangles within the nerve cell body. One theory assigns a causative role to the protein
tau, which helps organise and stabilise a cell's internal ‘skeleton', but which is deformed in AD, eventually aggregating into the tangles. This is a growing area of research.
□ abnormal (senile) plaque deposits between nerve cells, containing the protein beta amyloid (Aβ).
This is a prime area of research, to understand the abnormal processing of amyloid precursor protein (APP) which yields the Aβ fragments.
Areas affected by AD
A Cerebral Cortex
B Basal Forebrain
Alois Alzheimer, a German psychiatrist and pathologist, first published his findings on these ‘tangles and
plaques' in 1907. They occur consistently in people with AD and, interestingly, have also been observed
9 The following sections utilise information from Burns A, Purandare N, Mann D and Bagley H, of the Personal Social Services Research Unit, North West Dementia Centre, University of Manchester, NHS Executive North West, UK, 2001. 10 Images here and below courtesy of the National Institute on Aging, National Institute of Health, US, www.nia.nih.gov.
Illustrator: Lydia Kibiuk.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
in older people free from dementia. The ‘tangles and plaques' disrupt normal electrical conduction of
messages within the brain. A nerve cell chemical acetylcholine is also deficient in AD. Symptoms of AD can include:
□ gradual memory loss □ decline in ability to perform routine tasks □ disorientation to time and space □ impaired judgement, abstract thinking and physical coordination □ difficulty in learning and concentration □ loss of language and communication skills □ changes in personality, behaviour and mood (up to two thirds of people with AD have depressive
symptoms and about 20% exhibit aggression, more common in men)
□ hallucinations (experienced by 16%) and delusions (false beliefs), often paranoid (30%) □ loss of initiative □ altered sleep patterns, eating disturbances and screaming.
Cummings (2001) lists the prevalence of neuropsychiatric symptoms that commonly accompany AD as agitation (60% to 70% of people), apathy (60% to 70%), depression (50%), anxiety (50%), irritability
(50%), delusional disorders and psychosis (40% to 50%), disinhibition (30%) and hallucinations (10%). The symptoms and behaviours of AD, as well as the decreased functionality in ADL, can be physically
and emotionally difficult for families and carers to manage, requiring person-centred care skills, ongoing training, understanding and support.
"It is one of the truly heart-warming things about Alzheimer's that so many partners and offspring quietly
take on another's chores and devote themselves, quite selflessly, to the care of someone they love."
Hampson (2000), p54
Disease progression: Onset of AD is insidious and the disease lasts for 3-20 years (an average of 8)
from diagnosis although average length of time from diagnosis may be increasing as people are now presenting earlier in the illness (previously diagnosis was made on average 2–3 years after onset of
symptoms11). The first phase is typically around three to four years, characterised by mild symptoms of memory loss and disorientation requiring some assistance and surveillance (30% of diagnosed AD
sufferers have mild disease). As the disease progresses, more difficulties with daily functioning occur and assistance with daily living is increasingly required. Moderate disease occurs in a further 40% of
diagnosed AD cases. In the final years the disease is severe (the remaining 30% of diagnosed cases), with communication and movement problems and incontinence requiring high levels of specialised care,
often in a nursing home setting.12 Death is often attributable to pneumonia or infection.
Vascular dementia (VaD), accounts for a further 20-30% of cases of dementia. These people appear
to develop dementia from a narrowing of the arteries supplying the brain. The lack of blood can lead to
many small areas of damage to the brain, each too small to be noticeable as a ‘stroke' but collectively devastating in their effect. VaD is itself divided into sub-types:
□ arteriosclerotic – reduced oxygen supply to the brain (chronic ischaemia); □ acute onset – following strokes;
11 Brodaty H and Lie D, "Symptomatology: Functional Capacity and Behaviour" in Wimo et al (1998), p34. 12 When institutionalisation is required depends on marital status, caregiver availability/burden and disease severity. Galasko
et al (1995) found that about half the people developed severe symptoms within three years of onset, and two thirds within
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ multi-infarct dementia – gradual onset following a number of mini-strokes (transient ischaemic
attacks) in the outer brain (cortical areas);
□ subcortical or Binswanger's disease – demyelination (loss of the covering sheath of nerve fibres)
affecting multiple sites in the deep white matter of the brain; and
□ mixed cortical and subcortical VaD.
Like AD, VaD also results in symptoms that include impairment of memory, new learning, recognition,
fine motor movements and planning and, since it is quite common for both VaD and AD to occur together (mixed dementia) it may be difficult to separate the two. VaD can be distinguished if there is:
□ abrupt onset eg, following a stroke □ stepwise decline – severe worsening, then stability, then further deterioration □ patchy cognitive deficits eg, in memory but not so much in language □ less personality change and more insight into memory loss than in AD, where it is lost early □ more severe mood swings and more common depressive symptoms, hallucinations and delusions □ focal neurological signs and symptoms (eg, weakness or loss of sensation in part of the body) □ fluctuation in functioning – ‘good' days and ‘bad' days □ nocturnal confusion □ presence of vascular risk factors such as hypertension, diabetes.
Disease progression: As with AD, average survival is around eight years, although the course of VaD can be highly variable. In the early stages there may be only minor cognitive problems such as problem
solving, planning and memory. There may be long periods of stability with abrupt stepwise worsening. Disease progression is more amenable to control by addressing the severity of underlying vascular risk
factors. Cause of death is ultimately usually stroke or heart attack, or an associated chest infection.
Dementia with Lewy bodies (DLB): Lewy bodies are abnormal brain cells found in all parts of an
affected person's brain, the hallmark of this type of dementia. DLB can be quite common (10% of all
dementia), and has sub-types such as Diffuse Lewy Body Disease, Cortical Lewy Body Disease, Lewy Body Dementia, Senile Dementia Of Lewy Type, and Lewy Body Variant of Alzheimer's Disease. DLB is
similar to AD with ongoing loss of memory, language and reasoning, and often the presence of AD-type senile plaques although seldom with significant neurofibrillary tangles. DLB, however, progresses much
more rapidly than AD, and frontal lobe and visuo-spatial impairments usually occur earlier. Other features that differentiate DLB from AD include: motor traits of Parkinsonism, visual hallucinations,
systematised delusions, REM disturbance, marked daily fluctuations, and falls and syncopal episodes
(sudden loss of blood pressure resulting in fainting). In some families, DLB can be inherited.
Brain of a person with DLB
The diagram on the left shows the loss of nerve cells in the
midbrain region where the substantia nigra is located (where dopamine is made), which also occurs with Parkinson's disease. In
both diseases, the dark-brown pigment called neuromelanin is also lost so the substantia nigra appears abnormally pale. Shrinkage of
the brain is particularly seen in the temporal lobe, parietal lobe and cingulate gyrus. Lewy bodies can be detected by immunochemical
staining for the protein ubiquitin. The protein alpha synuclein is a major component of Lewy bodies.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Fronto-temporal [lobe] dementia (FTD): also discovered by Alzheimer, in 1923, and commonly
named after his colleague Arnold Pick (‘Pick's disease'). It occurs in 1 in 5,000 people, but with earlier onset (even as young as 30-40), so is the second most common dementia of under-65's. Illness
duration is longer – 10-15 years, with family history an important risk factor. Psychological testing and brain scanning (showing loss of tissue in the front parts of the brain) enable differential diagnosis.
Symptoms are largely personality and behavioural changes, including restlessness and loss of inhibitions resulting in unsocial attitudes and actions eg, sexual disinhibition. Behaviours become
repetitive and ritualistic, such as hoarding and food fads, with apathy and reduced or inappropriate speech as the disease progresses. Final stages include muteness. Post-mortem can show tangled
bundles of proteins in nerve cells, similar to those of AD, as well as rounded ones called ‘Pick bodies'.
Parkinson's disease, a progressive disorder of the nervous system, results from loss of the
neurotransmitter dopamine in the brain. Dopamine is a chemical involved in communication between the
nerves that control voluntary movements such as walking, talking and writing. It can take many years for Parkinson's disease to result in dementia, and indeed it may not always do so.
Huntington's disease: Huntington's disease is a hereditary disorder of the central nervous system
affecting about 1 in 10,000 people. It often strikes in mid-life (ages 30-50) but ranges from 2 to 80, and runs a relentless degenerative course over a period of 10-25 years. Unusual jerking or twisting
movements of the body (‘chorea', its distinguishing characteristic) accompany the onset of dementia with cognitive and emotional elements. Other symptoms later on are muscle rigidity, and impairments to
speech and swallowing (choking on food becomes a concern). Mortality is often from complications such as heart failure or aspiration pneumonia. There is now a presymptomatic blood test available
although taking it is the prerogative of at-risk individuals. Cell death in Huntington's disease may be caused by a ball of protein that forms in the cell nucleus, with current research exploring possible drug
treatments to prevent the accumulation of protein in cells.
Creutzfeldt-Jakob disease, is one of a group of disorders called human spongiform encephalopathies
that, until recently, were extremely rare, with an incidence of about 1 in 2 million, onset normally
between age 50 and 70 and with rapid deterioration. People may quickly pass from dementia symptoms into akinetic mutism (catatonic state) and die within 6 to 18 months. Recently a variant of Creutzfeldt-
Jakob disease has arisen with younger onset (mostly people under 30), transferred to humans from animals with Bovine Spongiform Encephalopathy (‘Mad Cow Disease'). In most instances the disease
appears without any apparent obvious cause, although there are very rare inherited forms, such as Gerstmann-Straussler Syndrome (characterised by ataxia – loss of balance – and dementia with death
after 3-5 years) and Fatal Familial Insomnia, as well as a transmissible form (once common in a Papua New Guinea tribe known as Kuru) and a few other medically induced cases. In most instances a definite
diagnosis can only be made through post mortem, characterised by:
□ swelling and loss of nerve cells, producing a widespread spongy change throughout the brain □ an increase in the size and number of brain cells, called astrocytes □ abnormal prion protein deposits between nerve cells, sometimes in large plaque accumulations.
Because of the long and variable latent period during which the disorder can be ‘incubating' it is
presently uncertain as to the extent to which iatrogenic Creutzfeldt-Jakob disease, especially the new variant form, might increase in future years. About 100 cases of the new variant have been confirmed in
UK, where the risk is possibly highest.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Younger onset dementia
Harvey (1998) reports epidemiological data and bottom-up costings for pre-senile dementia conducted by the Dementia Research Group in the UK. Specific findings, supported in other research, were that:
□ AD and DLB were less common in younger onset dementia, while FTD was more common; □ prompt and accurate diagnosis is critically important in younger people because there is more
likelihood that they are working, have children at home, have heavier financial commitments, have an inheritable form of dementia, and have difficulty obtaining a diagnosis and receiving care;
□ the earlier treatment is commenced, the greater the possibility of recovery; □ neuro-imaging was under-utilised, which should be addressed through better primary care training; □ high levels of non-cognitive (psychological and behavioural) symptoms were identified in this
□ individual packages of care services were required, which were often unavailable or underutilised by
younger people (eg, community psychiatric services), with informal (family) carers filling the gap;
□ levels of caregiver distress and burden were higher – over half of family carers were considered to
have formal psychiatric illness, including depression, indicating that assessment and ongoing
treatment of the family carer should be linked to that of the person with dementia;
□ lower use of community services led to a lower estimate of financial costs for this component but
shifted the burden to higher utilisation of institutional care – one third of the participants (under 65) were in institutional care compared to 15% aged between 65-74 (the requirement for residential
care increases with age after age 65);
□ residential care was estimated to have twenty times the direct costs of community care; □ costs increased slightly with increasing severity of disease, in part masked by the jump in costs of
institutionalisation (people in residential care were in all disease severity groups);
□ the study did not consider indirect costs, although concluding that these were also likely to be higher
for younger people, due to the greater economic impact of work sacrificed for both the person and
their younger carer;
□ dementia in younger people was thus found to have higher direct costs than in older people –
£7,189 to £7,868 (A$20,636 to A$22,586) per patient per annum;
□ average cost of AD was second-lowest while VaD, FTD and alcohol-related dementia were highest
(the latter most costly);
□ enhanced coordination, communication and training of community resources commenced in
response to the study, in order to better address the behavioural issues, reduce carer burden and distress and hence delay institutionalisation and provide more cost-effective care overall;
□ more epidemiological (‘bottom-up') studies of younger onset dementia need to be done, as there
are so few with which to compare.
1.1.3
The causes of dementia are not well understood, although certain risk factors
not a ‘normal'
may be significant.
Age: Age is the most well-accepted risk factor, with the likelihood of dementia
increasing from around 1 in a 1000 for people under 65, to 1% for people in their early sixties to well over 50% for people in their nineties.
Family history: Genetic factors contribute to dementia risk, particularly for certain types of younger
onset AD. A clear inherited pattern of AD exists in less than 10% of cases. Several genes have been identified on chromosomes 21 and 14 in the familial type of AD. In the more common sporadic type, people with the e4 form of a gene for a protein called apolipoprotein E on chromosome 19 (APOE-ε4)
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
tend to have a higher incidence of AD than the general population.13 In some cases of FTD, there is
mutation of a gene on chromosome 17 that makes tau, inhibiting the protein's function and causing it to bundle up into tangles and Pick bodies. However, about half of cases do not have these changes in tau
protein, although there are strong familial indicators for this type of dementia. In Creutzfeldt-Jakob disease, the prion gene is located on chromosome 20, with inherited forms the result of mutations in this
gene, causing a 50% chance of children inheriting the disease from an affected parent. For Huntington's disease, there is a ‘genetic stutter' - a stretch of DNA repeated over and over at one end of a gene on
Chromosome 4. Much more work needs to be done to fully understand how genetics influences the incidence of AD. In addition, there is growing concern that genetic testing (eg, for the e4 allele) may lead
to misunderstanding and that insurance companies or employers may misuse positive test results.
Gender: Over the age of 80, women are at slightly higher risk of AD, while men may be at higher risk of
VaD. The Boston University School of Medicine Multi-Institutional Research in Alzheimer's Genetic
Epidemiology study showed that by age 93, female risk is 13% higher than male risk. There is some evidence that higher risk in women may be due to post-menopausal hormonal changes.
Cardiovascular risk factors, stroke-related and atherogenic causes contribute to VaD and there is
increasing evidence that they also contribute to AD – including high blood pressure (severe systolic hypertension), narrowing of the arteries (atherosclerosis), irregular heartbeat (atrial fibrillation),
ischaemic heart disease and attacks (myocardial infarction), diabetes, high saturated fat and LDL cholesterol intake and smoking.14 On-pump coronary artery bypass graft surgery may contribute to VaD.
Education and employment: One hypothesis is that higher levels of education or a lifetime of mental
activity may increase the brain reserve by increasing the synaptic density in the neo-cortical association cortex (Stern et al, 1994). Other studies suggest that specific occupational exposures may increase AD
risk, such as manual work (Fratiglioni et al, 1993) and exposure to organic solvents (Kukull et al, 1995) or electromagnetic fields (Sobel et al, 1995 and 1996), for example in occupations such as carpenter,
electrician, machinist, sheet metal worker, typist or welder. If further research strengthens this evidence, and the link is not just socio-economic, there would be further rationale for preventive workplace
measures such as shielding and separation.
Other possible risk factors: Psychiatric illness (especially depression) may also contribute to AD, as
may previous thyroid diseases, head trauma, excessive alcohol intake, or aluminium (eg, in drinking
water)15. Free radical damage to neurons (oxidative stress), probably the most significant cause of biological ageing, may contribute to dementia (Christen, 2000). Inflammation, involving cytokines and
prostaglandins, may be another contributing factor to AD, primarily because beta-amyloid is an inflammatory protein (C-reactive protein is a marker of inflammation associated with AD)16. Glycation is
a process central to aging, where advanced glycation end products (AGEs) are formed that may also be part of AD, as they have been found in the neurofibrillary tangles. There has also been the hypothesis
that the immune system may gradually attack the brain as we age. Some brain disorders that cause
13 ApoE is a transport protein in lipid metabolism with three major isoforms – e2, e3 and e4 on chromosome 19. It is the e4
allele that is associated with increased risk of AD (e2 is thought to reduce risk). This is another area of research, as is the
link with Down's Syndrome; nearly all people with Down's Syndrome (trisomy 21) who live into their 40s develop AD. 14 A few studies have shown reduced incidence of AD among light smokers (fewer than 10 cigarettes per day), but increased incidence among heavy smokers (more than 20 cigarettes per day). Nicotine causes acetylcholine transmitter release and is
thus theoretically of benefit in AD which has reduced acetylcholine levels. 15 If AD is a possible long term outcome of head trauma, there is even more justification for public prevention activities such
as compulsory seat-belts, helmets and restrictions on boxing. Aluminium, mercury, copper and other metals found in the brain tissue of people with AD may not cause AD, but result from the disease process. Further research is needed to clarify
the roles of these metals in dementia. For more detail, see Alzheimer's Australia (2002b). 16 A recent study on CRP as a marker (or playing a causal role) is in Ann Neurol 2002,52: 168-174.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
symptoms similar to AD are caused by slow viruses. However, a virus specific for AD has not been
identified. There has been some evidence of lower prevalence rates for AD in some developing countries and in rural areas, although the evidence regarding ethnic and cultural influences is unclear.
Possible protective factors that may reduce the risk of developing AD, include:
□ Use of pharmacotherapies: The use of anti-inflammatory drugs (eg, in treating arthritis) – including
both steroids and non-steroidal anti-inflammatory drugs (NSAIDs) – has shown a protective effect for dementia, triggering research on inflammation as a possible element of dementia pathology.
Pooling data from many case-control studies show that people with prolonged use of anti-inflammatories have around half the risk of AD, and it is being trialled as a preventive therapy in
high-risk individuals in the US. Taking statins, the most widely used cholesterol-lowering drugs, may reduce dementia risk by as much as 71%.17 Oestrogen may well have a protective effect (up to 30%
reduced risk), although there is contradictory evidence regarding postmenopausal hormone replacement therapy as the link may be educational and socio-economic. Further research is being
undertaken in this area, such as the Women's Health Initiative Memory Study, a large US trial.
□ Diet: Recent studies have found that high intakes of antioxidants from food – vitamin C, vitamin E,
and beta carotene, for example — may guard against AD.18 Other studies have identified fish and seafood, wine and Ginkgo biloba consumption as having a potentially protective effect.19 More
recently, a Boston University study corroborated other evidence that the risk of contracting AD nearly doubles in people with high levels of the amino acid homocysteine (also a risk factor for heart
disease), suggesting that consuming more folic acid and vitamins B6 and B12, which can reduce homocysteine levels, may also guard against AD (see also Section 1.2).
1.1.4 Mortality
The dementia specific mortality rate is twice the rate of people without dementia – 2.4 (1.4-4.4) per 100
person-years, controlling for co-morbidities and socio-demographic factors. In Australia the crude mortality rate reported in 2000 was 19.1 per 100,000 (3,655 deaths), 26.3 for women and 11.8 for men,
or 15.4 and 12.4 age-standardised respectively20. Age-standardised rates for people 85 and over are much higher at 982 for women and 641 for men per 100,000. 70% of people over 75 with dementia die
within five years.21 Death certificates grossly under-report dementia as the cause of death, often citing instead respiratory infection. AD is estimated to be the fourth leading cause of death in developed
nations (after heart disease, cancer and stroke).22 The number of deaths from dementia in Australia by age and gender is shown in Table 14 (Section 2.2.1), under-estimated for the reasons above.
Dementia shortens life even in the very old. Iris Murdoch, prominent British novelist and lecturer, described her decline as "sailing into darkness". Her husband and carer, John Bayley, comments on
her death: "She is not sailing into the dark: the voyage is over, and under the dark escort of Alzheimer's,
she has arrived somewhere. So have I."
17 "Statins Associated With Lower Dementia Risk", Harvard Medical School Family Health Guide: Chapter Update - Brain and
Nervous System, available on www.health.harvard.edu, October 2001 update. 18 "Dietary Antioxidants May Decrease Risk of Alzheimer's Disease", ibid, August 2002 update. 19 For example, British Medical Journal (fish), October 2002, the UK Alzheimer's Society (ginkgo), October 2002, and Journal of Neurology (wine) November 2002 articles cited in Alzheimer Europe (2002). 20 AIHW (2002a), p36-37, for this and the next sentence. 21 Wimo et al (1998), p24. 22 Life Extension Foundation (2002). 23 Bayley's book was made into a Miramax film, Iris, starring Judi Dench, Kate Winslet and Jim Broadbent. It sensitively
depicts Bayley's life with Murdoch "from their first meeting at Oxford through their struggles with Murdoch's heartbreaking
decline as Alzheimer's disease eroded one of the keenest minds in contemporary literature" (http://video.go.com/iris/)
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.2 TREATMENT AND MANAGEMENT
Although there is no cure, there are ways to reduce risk factors, treat and manage the behavioural and
psychological signs and symptoms of dementia (BPSD), and improve quality of life for the individual and family carer, through:
□ promoting an understanding of what is quality dementia care; □ prevention and early diagnosis/intervention; □ psychosocial approaches including support, counselling, education and memory loss programs; □ use of medications (pharmaceutical and natural) to treat cognitive decline and memory loss; □ medical and surgical interventions; □ the availability of appropriate community services, including respite; and □ residential care services, including dementia specific services.
The progression of dementia, the variety of causes and differences in individual circumstances prevent any mechanical approach to treatment but the model of severity by types of care for patients with BPSD
(see the "Brodaty Triangle" diagram after the Methodology section) illustrates the different levels of management that need to be in place.
1.2.1 Quality of care
Henderson and Jorm (1998) summarise quality care principles as:
□ accurate assessment of the resident's needs and functioning □ knowledge of the staff about dementia □ individualised care □ activities that are tailored to the individual □ appropriate attitudes of staff □ communication skills □ use of the physical environment24 □ support for the family carer.
Rosewarne et al (2000) also emphasise the need for residential care facilities to own and practise a
person-centred care philosophy, from senior management down, and apply it to day-to-day practices, care planning, behaviour management, staff appraisals, personal care routines, communication with
relatives and activity programming. Features of quality care outlined below include the need to:
□ redefine problems and understand behaviours of people with dementia – ie, focus on the person
and not just target the behaviours;
□ plan and implement specialised activity programs – to stimulate interest and encourage activities
designed to address specific psychosocial needs and preferences;
□ personalise the care – emphasising intimate knowledge of who the resident is – their history, family
connections, values and current circumstances;
□ give staff ownership and care responsibility - build staff-resident relationships by subdividing large
numbers of residents into small working groups, for whom designated care teams are responsible;
□ create domestically scaled social environments – cluster house designs, with kitchen-dining focus
areas, have been successful in creating a homelike environment and building social interactions;
24 For example, ample space for safe walking.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ provide flexibility of care routines and practices – a relaxed organisational environment using
strategies that focus on timing, routines and needs of residents, preventing resistive responses;25
□ cultivate professionalism of care and support of staff – create a culture of doing something
innovative, progressive and worthwhile, rather than a task-oriented ‘completion of jobs' approach;
□ include relatives in the life and care of the resident – expend effort to maintain continuity in the
resident's life through encouraging ongoing contact with family and others who can provide undivided personal attention.
Person-centred care philosophy
Care is about the person behind the illness, and entering into their world. A fundamental premise is that all people are entitled to the best possible quality of life, with dignity, in comfortable surroundings and
with the assurance that he or she has personal worth and is valued by others. ‘Challenging' reactions and behaviours may be environmentally provoked and are rarer in a calm environment with trained staff
who are understanding and take a personal interest in the residents and who promote a feeling of security. Sherman (1999) is an excellent book for carers, written from many years' experience as an
Australian carer in a residential setting and also caring for her husband, Bill, who had dementia. The book is rich with personalised examples of care that is full of skilled insights into the reasons for
behaviours, patience, respect, wisdom and humane strategies for sensitively helping people. For example, people with dementia may be prone to agitation, wandering, suspiciousness, inappropriate language or screaming, sexual disinhibition, apathy, self-injury, combativeness, repetitious demands or
resistance to maintaining hygiene. In each case there is a need to seek the reason underlying the specific behaviour, and then as far as possible to meet the need - listening, responding, gently
prompting, providing reassurance, company, respect, praise, etc. The following checks can also help:
□ environmental modifications, such as limiting noise and glare from windows to reduce confusion
caused by over-stimulation, putting calendars and clocks in many rooms, or playing soft music
□ providing predictable but stimulating routines with structured times for daily activities and, if
insomnia is a problem, cutting down caffeine, getting regular exercise and avoiding daytime naps
□ explaining tasks beforehand, for example "Peter, I'm going to help you put on your shirt now" □ providing reassurance without challenging or contradicting accusations or misperceptions □ redirecting attention and use of light-heartedness and humour "The man in the mirror is taking his
clothes off – you put yours on and he'll put his back on too!"
□ dignified precautions to help prevent wandering/intrusions/"attacks" eg, disguised doors, signs □ recording behaviour patterns including frequency, timing and strategies that work with that person.
Modelling: The three women who sit near the outside door are irritated by Bob, who no longer knows,
and is beyond learning, how to manipulate handles and knobs. Several times a day he tries to go into
the garden. Gripping the handle, he rattles the door. The women call to him to stop. ‘Go away, go away'
they tell him, as he becomes infuriated when the door fails to open. For the next day of two the nurse
quietly opens the door for him. ‘There you are, Bob, you can go out now', each time turning to the women to say, ‘He has forgotten how to open the door. He can't help it, you know.' From then on, one or
other of the women opens the door for Bob, explaining to anyone who cares to listen, ‘He can't help it, he's forgotten.' Staff praise them for their caring attitude.
25 Rosewarne et al (2000, p66) describe this as "Flexibility and resident-centred care is a product of staff attitudes and organisational predisposition, a more even allocation of direct care hours throughout the day, multi-tasking approaches,
resident-staff assignment models and a willingness to give more control to residents, or refrain from exerting control when
not really necessary."
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Establishing connection
A key to providing quality care is to provide effective
Normal connection
connection (different from communication, which can
Increasing egocentricity
be passive) between the
as external world shrinks
person with dementia and
environment of perhaps a metre diameter
the caregiver (either formal or informal). This is
illustrated in the diagram at left. As dementia
progresses, there is an
increasing egocentricity of
the person – their capacity
to connect to the world becomes increasingly smaller. Conversely, this means that any caregiver has to
provide greater effort to establish and maintain connection. Connection involves caregiver time and skills, and thus is intimately related to costs of care in terms of dollars as well as emotional burden that,
in turn, relates to financial costs in terms of carer support levels, staff turnover and training.26 Alzheimer's Australia (2003) provides an excellent summary of the philosophy, care environment and key elements of quality dementia care. Current accreditation standards could be enhanced further to
promote these aspects of quality dementia care. At present, the stated aims of standards and certification are to "provide a high quality of personal care to every resident, to have a safe building and
to be committed to protecting their resident's rights"27. Standards cover all aspects of residents' needs
from health and personal care and safety to a range of lifestyle matters including independence, privacy
and dignity. Accreditation standards focus on:
□ identification and compliance with all relevant State and Territory legislation, regulation, professional
standards and guidelines (including those issued by Nurses Registration Boards); and
□ maintenance of an adequate number of appropriately skilled staff to ensure that the care needs of
residents are met, with an obligation of providers to ensure that the staffing skills mix reflects current
resident care needs, and arrangements for the ongoing development of staff skills.28
Accreditation is granted through the Aged Care Standards and Accreditation Agency, with some 3000
residential aged care services currently accredited nationwide. Under the Aged Care Act 1997, the Commonwealth pays residential care subsidies – 75% of the cost of care for residents – only if
accreditation standards are met, with sanctions imposed for non-compliance29. Monitoring involves scheduled visits and spot checks. The complementary certification process focuses on improving the
physical environment in residential facilities, which led to over $800m in capital investment between 1997 and 2001 when first phase accreditation was completed. Under the 1997 Act, a service must be
certified to be able to charge accommodation bonds or accommodation charges or receive concessional resident supplements. All new buildings must meet privacy and space requirements while existing
buildings must meet these no later than 31 December 2008.
26 Diagram and concept courtesy of Virginia Moore, Dementia Services Consultant, Brightwater Care Group, with
acknowledgement also of Perrin and May (2000). 27 DHA, Residential Care Standards and Accreditation, available on www.health.gov.au/acc/rescare/standard.htm 28 DHA, Residential Care Manual - Chapter 11 - Accreditation and Quality of Care, Sep 2002, available on
www.health.gov.au:80/acc/manuals/rcm/contents/11accrq3.htm 29 At the time of writing, 5 facilities Australia-wide had sanctions imposed, 2 in QLD, and 1 in each of NSW, SA and TAS.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.2.2 Prevention and early diagnosis
Prevention and research: Prevention of dementia can involve either elimination (not yet possible) or,
as for other chronic diseases of ageing, postponement of onset till later in the lifespan. The best chance for disease elimination is possibly related to stimulating an immune system response that destroys Aβ
(see Section 1.2.2).
Postponing onset: Addressing contributing medical or psychological factors (eg, cardiovascular
factors, reducing head trauma) is important as either preventive or treatment measures – for example,
cessation of smoking, balanced diet, regular exercise, modest intake of alcohol, controlling blood pressure and cholesterol30 (eg, through statins, cholesterol-lowering drugs and reduced salt intake).
Reducing stress may also be important. The preventive value of NSAIDs, oestrogen, antioxidants, anti-platelet treatment and reducing homocysteine through increased folate are discussed in the following
sections.
Research: A number of dementia research activities are funded through the National Health and
Medical Research Council as well as other public and private interests, although these are limited (see
Section 3.2.5). There is scope to substantially increase research in prevention, treatment and cure:
□ understanding of the biomedical causes of dementia; □ measures that can prevent or postpone the onset of dementia; □ new pharmacological therapies to slow and reverse disease progression (these may be just around
□ epidemiological (population-based) medical and public health research31; □ effective models of care for people with dementia.
"Alzheimer's research is advancing at an accelerating pace. Recent discoveries support the notion that we may soon be able to delay the onset of the disease and allow people with Alzheimer's disease to
continue functioning independently for longer periods."
US Alzheimer's Association
Prospects for indicated prevention: Indicated prevention is one step before early intervention, where
people have minimal symptoms foreshadowing disease. Researchers have proposed the existence of a state of Mild Cognitive Impairment (MCI) – memory impairment beyond that expected for their age and
education – which may be an indicator of high risk (10-15%) for developing dementia (Black et al, 2001). Jorm (2002) states that:
"It is only a matter of time before some drug is developed which actually slows progression. If such a drug were very cheap and had no side effects, we might want to give it to everybody above a
certain age as a [selective] preventive measure. However, if it were expensive and had side-effects, as is more likely to be the case, it could be reserved for people with minimal symptoms, for
example with MCI."
30 The Syst-Eur trial showed that people aged 60+ with systolic hypertension and randomly receiving anti-hypertensive drugs
had 50% reduced incidence of dementia (AD and VaD) after two years. Another large trial underway is the PROGRESS trial,
with results expected soon. Statins may reduce stroke risk by 29% and there is also evidence they lower the risk of dementia (Jorm, 2002). 31 This research, together with awareness campaigns, has enabled diseases such as lung, skin and breast cancer to be seen
as conditions with preventable elements subject to a public health approach.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Trials of such preventive interventions are already occurring, including for example one trial in the US
comparing the effects of vitamin E and donepezil (Aricept) in preventing the development of AD in people diagnosed with MCI.
Early diagnosis and intervention helps those involved have more control over the disease and their
lives. By early use of pharmacotherapies and by learning strategies to help cope with the many changes brought on by dementia, people are more able to live meaningful, productive lives for longer periods.
Being able to recognise symptoms and obtain an accurate diagnosis early means:
□ Drug and medical treatments can be commenced which
benefit people most in the early to moderate stages;
Early diagnosis means
□ Reversible conditions (such as depression and delirium)
the person and the family
can be treated, improving the prognosis;
can benefit from drug
□ Financial and legal plans can be made, with the full
treatments, support and
agreement of the person with dementia;
□ The individual and family can adjust better to the diagnosis,
understand the illness and learn how to cope better through adequate counselling and education.
Pipher (1999) observes that taking a pragmatic, uncomplaining approach, as many older people
(particularly males or people of English origin) may do, may not be helpful – their "stoicism is now called denial". Hampson (2000) observes that "denial is a major issue in the delay of diagnosis of dementia,
and even after diagnosis". Many family members cannot come to terms with dementia or feel that it is stigmatised. Initially it can be harder to accept because of the lack of tangible "proof". For others, the
problem may be convincing the family doctor that something is wrong, when dementia symptoms are diagnosed as stress, tiredness, depression or ‘old age'. Even though this may be ‘comforting', several
years later the symptoms become too severe to ignore and precious time has been lost. However, many GPs remain uninformed about advances in dementia assessment and diagnosis, have difficulty diagnosing dementia and do not refer the person with dementia on to community support
services, although steps are being taken to address these problems (see Section 1.2.4 on GPs and 3.2.1 on cost-effectiveness of early intervention).
"I still consider myself fortunate. I believe my early diagnosis led me to accept the disease more easily
because I still retain powers of reasoning. It has allowed Mavis and me to become educated about the disease and to complete all the legal documents while I am still in possession of my faculties. Together
we can make important decisions about my future treatment. My wishes can be discussed in a rational way without either of us becoming upset. For these reasons I urge the medical profession to make an
early diagnosis and allow Alzheimer's sufferers the time to make their own decisions."
Another important benefit of early intervention is the positive impact for the caregiver. A recent US study
demonstrated that the well-being of the caregiver and care recipient are closely related, and in particular that the risk of clinical depression for the caregiver was higher if either the care recipient was depressed
or agitated, or they themselves were in poor health. Early interventions for the person with dementia were thus found to also increase the level of health of the caregiver. Black et al (2001, p11) also point to
evidence that early diagnosis can improve the health and coping skills of the family carer and delay institutionalisation.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.2.3 Pharmacological management
Anticholinesterase32 (anti-dementia) drugs: The chemical that breaks down acetylcholine is blocked
by drugs called (acetyl) cholinesterase inhibitors or CEIs. They work best in the mild to moderate stages of AD – by the later stages so few cells are left that make acetylcholine, that even if their breakdown is
protected there are still not a lot carrying messages. Evidence is also growing that they may be effective in VaD and dementia with Lewy bodies, and that use in later stages may also be beneficial. The
situation is very much a moving feast. Numerous trials indicate that consistent prolonged use of the various anti-dementia drugs delays the progression of symptoms of dementia in the majority of people
for nine to twelve months on average and possibly longer (see Section 3.3.1). There may be some improvement in clarity of thought, ADL functionality, mood and behaviour. The current drugs do not
result in halting the progression of dementia, although studies are looking at the effectiveness of combination treatments to this end.33 Side effects (which vary with each drug) may include nausea,
vomiting, cramps, fatigue and loss of appetite, and are minimised if the dose is gradually increased, often settling down with time. There are four cholinesterase inhibitors currently available in Australia.34
□ Tacrine ("Cognex") was approved for marketing in Australia by the TGA in 1995, but two
successive applications for a PBS listing were refused. Its use is thus uncommon in Australia.
□ Donepezil ("Aricept" by Pfizer) was approved for marketing in 1998, but an initial application for
PBS listing was turned down, ostensibly for cost-benefit reasons. The efficacy and tolerability of Aricept has been established, with Cochrane review concluding: "In selected patients with mild or
moderate Alzheimer's disease treated for periods of 12, 24 or 52 weeks, donepezil produced modest improvements in cognitive function and study clinicians rated global clinical state more
positively in treated patients" (Birks, Melzer and Beppu, 2003). Results showed improvement from baseline ADAS-Cog and Clinician's Interview-Based Impression of Change measures. Since then,
Aricept has undergone extensive trialling against placebos and other drugs and in other contexts showing, for example, that people with moderate to severe AD may also benefit from treatment.35
□ Rivastigmine ("Exelon" by Novartis) was approved for marketing in 2000 and both it and donepezil
became available on the PBS from February 2001, after subsequent applications. Cochrane review concluded that: "Rivastigmine appears to be beneficial for people with mild to moderate Alzheimer's
disease. In comparisons with placebo, improvements were seen in cognitive function, activities of daily living, and severity of dementia with daily doses of 6 to 12 mg" (Birks, Grimley Evans,
Iakovidou and Tsolaki, 2003). Longitudinal studies of ambulatory patients with mild to moderate AD suggest the gain on placebo may be an average 4.9 units (from 23 at baseline) after 26 weeks on
the ADAS-Cog from 6-12mg Exelon daily.36
□ Galantamine ("Reminyl" by Janssen-Cilag) was approved for marketing and PBS subsidy from
1 November 2001. Cochrane study concluded: "This review shows consistent positive effects for galantamine for trials of 3 months, 5 months and 6 months duration…. There is therefore evidence
for efficacy of galantamine on global ratings, cognitive tests, assessments of ADLs and behaviour. This magnitude for the cognitive effect is similar to that associated with other cholinesterase
32 Also known as cholinergic drugs, cholinesterase inhibitors, anti cholinestrators. 33 For example, donepezil has been shown to improve aspects of cognitive functioning and on ADL in persons with AD
(Saine et al, 2002). However, Phase III trials are showing that combination therapy of memantine and donepezil elicit a sustained improvement in cognitive function. See "Forest Labs' Drug Combo Effective in Alzheimer's Study" Monday 9
December 2002, Dow Jones report (New York). 34 Medscape's "New Treatments for Alzheimer's Disease: Pharmacokinetics of ChEIs" Drug Benefit Trends, provides a
concise comparative summary of the mechanisms of these drugs, usage, and side-effects. See also Alzheimer's Association (2001b), including dosages, for this section and the prescribing information following. 35 See Birks, Melzer and Beppu (2003 Cochrane Library) and www.aricept.com, for product information. 36 See www.exelon.com for product information.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
inhibitors including donepezil, rivastigmine, and tacrine" (Olin and Schneider, 2003). Recent trials
suggest galantamine may slow decline in cognitive function (memory, learning and problem-solving) by 12 to 18 months in mild to moderate patients who take 24-32mg daily consistently over three
years ie, 50% delay in disease progression.37 Reminyl is subsidised on the PBS to a maximum of 16mg/day.
The full cost of CEI drugs to government in Australia in 2002 is approximately $160 per month. Rules for
obtaining subsidised Aricept, Exelon and Reminyl through the PBS are complex. People must have a diagnosis of probable mild to moderate AD confirmed by a specialist (MMSE score of at least 10), with a
baseline cognitive measurement (ADAS-Cog) if the MMSE is 25 or more. A diagnosis of VaD or dementia with Lewy bodies precludes the subsidy. Continuing to receive the subsidy depends on the
results of reassessment within or after the first six months, which must show cognitive improvement of at least 2 MMSE points (or of at least 4 ADAS-Cog points if this was required). The subsidy then
continues to be available until the doctor identifies that AD has moved into the severe stage, with reassessment every six months. The initial authority application (including test results), and the first
ongoing authority (also including test results) must be in writing; there is no access to telephone, fax or email approval.38 There are special provisions for people who have language difficulties affecting the
test results eg, indigenous people, people from non-English speaking backgrounds and people with intellectual disabilities or illiteracy. PBS data shows around 18,500 Australians were using Aricept,
Exelon and Reminyl in December 2002, some 16% of those with mild and moderate dementia or 23% of those with mild and moderate AD. There thus appears scope for increasing application to the target
group.
Aspirin and blood-thinning (anti-platelet) agents: These reduce the risk that blood will clot and
produce a stroke, as well as having anti-inflammatory properties (see footnote 43). Cochrane review
stated that: "Aspirin is widely prescribed for patients with a diagnosis of vascular dementia; in one study, completed by geriatricians and psychiatrists in the UK, 80% of patients with cognitive impairment (with
vascular risk factors) were prescribed aspirin" (Williams, Rands, Orrel and Spector, 2003). Although they form the mainstay of treatment to slow the progression of VaD, there is a division of opinion on
their effectiveness. One side-effect of aspirin is increased risk of bleeding, particularly for high-risk people (eg, with duodenal or stomach ulcers).
Other medications: A variety of drugs are used to manage symptoms of depression (eg, insomnia),
restlessness, hallucinations, hostility and agitation, and can help the involuntary movements and emotional disorders for some people with Huntington's disease.
Other existing new or upcoming drug therapies for dementia include:
□ future amyloid-based treatments: research into amyloid processing has identified some potential
therapeutical applications:
• stimulating an immune system response that destroys Aβ. Although the first immunotherapy to
reach trials – the Alzheimer "vaccine" – was disappointing (Chapman, 2000), new ones under development show promise in preventing and possibly reversing AD39
37 See "Study shows benefits of reminyl may be sustained for at least three years for patients with alzheimer's disease" on
www.janssen-cilag.com/news/detail.jhtml?itemname=c_02_news_jul02 See www.reminyl.com for product information. 38 International Psychogeriatric Association, 2001 and www.health.gov.au/pbs/index.htm 39 Clinical trials of AN-1792, the investigational "Alzheimer vaccine" being developed by Elan Corporation and Wyeth Pharmaceuticals, were stopped in January 2002 after 15 participants developed symptoms of brain inflammation. However,
new findings in late 2002, reported in Nature Medicine and Nature Neuroscience, by two groups of researchers provide
evidence that the concept underlying the vaccine is promising and that modifications may be possible to make it safer. The
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
• secretases – are inhibiting enzymes that break up APP, thus reducing levels of Aβ by affecting
its cleavage and metabolism. These are a promising area of research currently at the clinical trial stage.40
• p53 inhibitors – the protein p53 helps damaged cells to die, thus defective p53 allows cancer
cells to grow. In very recent research, new compounds are being developed to inhibit p53 in the brain, keeping cells alive longer and protecting the brain from Aβ.41
□ memantine, available in the EU and undergoing Phase III trials in the US, is a non-competitive N-
methyl-D-aspartate antagonist that blocks the action of glutamate (glutamate can over-stimulate the nervous system and become toxic to nerve cells). Memantine has had positive response in the
Clinical Global Impression of Change and the Behavioural Rating Scale for Geriatric Patients (BGP), particularly the 'care dependence' sub-score. It is very promising, particularly in combination
therapy.42
□ hormone replacement therapy – oestrogen and progesterone supplementation continue to be
investigated, though opinion is mixed (Fillit, 2002) – see possible protective factors (Section 1.1.3).
□ anti-inflammatories – including preventive effects of long term use of NSAIDs (Zandi et al, 2002)43,
ibuprofen, Cox-2 inhibitors. Anti-inflammatory drugs may warrant future trials, although they can have potentially dangerous side effects so preventive benefits may only outweigh risks in very high-
risk individuals.
□ possible new acetylcholinesterase inhibitors – research is continuing in the hope of improved anti-
dementia drugs which may further slow the progression of dementia – one such (metrifonate), seemed promising but was withdrawn after a number of adverse effects. More recently, phenserine, a third generation acetylcholinesterase inhibitor with dual action, reducing APP and Aβ formation,
has possible potential to further slow progression of AD and other dementia.44
□ MAO-B inhibitors (anti-oxidants) – notably selegilene (Eldepryl or Deprenyl), a drug approved for
use in Parkinson's disease, which may have a long-term helpful effect on memory in mild to moderate AD through a number of pathways – reducing free radical damage, anti-apoptotic (reducing programmed cell death as per p53 below) protecting cells from the toxic effects of Aβ and
increasing nitric oxide production which increases cerebral blood flow (Life Extension Foundation, 2002).
□ nerve growth factor (NGF) supplementation – stimulates neuronal cell growth, survival and repair,
and is a promising area of research, with trials now underway.45
study showed 60% reduction in plaque formation in mice, using an antibody that blocks the CD40-CD40L protein. Because
there was also a reversal in established plaque formation, this research holds hope as both a prevention and a cure. 40 Secretases are the same category of enzymes targeted by the protease inhibitors that have revolutionised AIDS therapy.
Researchers led by Dr Michael Irizarry at Massachusetts General Hospital concluded their mid-2002 tests showed "clear
support for beta-secretase activity as an important target for therapeutic intervention" Arch Neurol 2002; 59:1367-1368. 41 Journal of Medicinal Chemistry, 7 November 2002, cited in Alzheimer Europe (2002). 42 "Ebixa" (by Merz) is a trade name for memantine released in October 2002 in the UK. 43 This study was of 3,227 over-65s in Cache County, Utah, and found that long term use (more than two years) resulted in
45% the incidence of dementia in non-users, with even greater protection for longer term users, and provided the use occurs
well before the onset of dementia. Aspirin compounds showed the best results, but these were strong also for ibuprofen, naproxen, diclofenac, nabumetone, sulindac and oxaprozin, as well as histamine H2 receptor antagonists (H2RA). Non-
inflammatory pain relievers used as controls had no effect on dementia risk. 44 See for example, National Institute of Ageing www.nia.hih.gov and "Phenserine shows potential to slow or stop
progression of Alzheimer's disease", April 4 2002 on www.seniorjournal.com 45 There are now trials of NGF proteins on humans, also for stroke, spinal cord injury and other nerve-damaging conditions
(Gustilo et al, 1999). Experiments on rats have shown that NGF promoted growth of new synaptic connections in a part of
the brain called the hippocampus, which could help restore memory loss and potentially reverse AD.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ nimodipine, a calcium channel blocker, can be of some benefit in the treatment of patients with
dementia, cerebrovascular disease, or mixed AD and cerebrovascular disease; however, its short-term benefits probably do not justify its use as a long-term anti-dementia drug (López-Arrieta, 2002).
□ piracetam, a derivative of gamma-aminobutyric acid, also used in Europe for the treatment of
memory loss and other cognitive defects. Piracetam has beneficial effects on the fluidity of
membranes from the hippocampus of people with AD (Muller, Eckert et al, 1999). In a Hungarian study, MMSE scores increased, with particular improvement for memory, concentration-
psychomotor speed and depressive symptoms (Tariska and Paksy, 2000).
□ aminoguanidine could be of value in reducing AGEs in AD, but requires large clinical trials if merit is
to be established (Ramamurthy et al, 1999).
□ nefiracetam may be useful in AD due to its ability to stimulate nicotinic acetylcholine receptors
(Nishizaki, Matsuoka et al, 2000).
□ metanicotine, which is less toxic than nicotine and causes nearly the same acetylcholine release, is
currently under clinical studies for use in AD.
1.2.4 Natural / alternative treatments
Many natural, traditional or alternative treatments are used with dementia46, including:
□ acetylcholine support – eg, lecithin (phosphatidylcholine) □ antioxidants – Ginkgo biloba (see below), Vitamin C, Vitamin E, Acetyl-L-carnitine, N-Acetyl
cysteine; some studies show Vitamin C may be protective but evidence for Vitamin E is more mixed.
□ anti-inflammatories – essential fatty acids including omega-3 and omega-6, docosa-hexaenoic acid,
eicosa-pentaenoic acid, gamma linolenic acid and S-adenosyl methionine (SAMe).
□ homocysteine reduction – Vitamin B12, Vitamin B6, folic acid, SAMe (particularly if depressive
signs); trials are now underway exploring the effects of increased folate on VaD.47
□ nervous system support – methylcobalamin (the neurologically active form of vitamin B12),
phosphatidylserine, inositol, Vitamin K, idebenone, melatonin (particularly if there is insomnia) and
□ Early morning sunlight exposure – for people who suffer sleep disorders and night wanderings as a
result of damage to the pineal gland (which produces melatonin), together with a strict routine of sleep, meals and social activities.
□ AGEs inhibitors – Vitamins B1 and B6, carnosine. □ herbal treatments – huperzine A, kut, curcumin (tumeric).
Of these, Ginkgo biloba, derived from the leaves of a Chinese tree, has recently come under new
scrutiny for its anti-inflammatory, anti-oxidant and anti-platelet properties. A 2002 British review of 33 clinical trials since 1976 concluded: "Overall there is promising evidence of improvement in cognition
and function associated with Ginkgo. Our view is there is need for a large trial using modern methodology to provide robust estimates of the size and mechanism of the treatment effects."
46 More detail on alternative treatments, as well as pharmacotherapies, is provided in Life Extension Foundation (2002). 47 Homocysteine is a by-product of a wide variety of chemical reactions in the body, possibly associated with AD as well as
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
"I decided not to use Aricept because it is far too expensive. I wanted to see how good the herbal things
are, and so far they are doing a wonderful job. I take ginkgo biloba and vitamin E, 1000mg/day. They have been crucial, and I have noticed the effect. I also take fish oil, aloe vera, lecithin, B complex and
vitamin C. These have all helped me immensely. There is a fellow at my early onset group who has dementia and had been virtually housebound for three years, very disoriented and confused, lost all his
confidence. I noticed he had started to slur his words. I told his wife to get him into the ginkgo and vitamin E. That was about six weeks ago. I saw him at a meeting recently and the improvement was
incredible… To talk to him you wouldn't know he had dementia, and he had actually been down to Sydney for a little holiday – on his own!
1.2.5 Other medical and surgical interventions
General practice: The GP plays a key, long term role recognising, assessing, planning, managing,
referring, coordinating and supporting the person with dementia, and their family carer. The GP's role is
very important from the early stages of the diagnostic process (especially differential diagnoses), through relationship and life planning, learning strategies, prescribing medications, co-ordinating referral
to specialists and to community care, arranging admission to hospital and attendance at nursing homes. As the illness progresses, the family or carer will seek the GP's advice more on behalf of the individual –
so there are in effect two patients, not just one. However, surveys showed that, in 1998, only about half of GPs were able to recognise mild dementia and about 70% were able to identify moderate dementia (Creasey and Brodaty, 1998). Many GPs find it
difficult to differentiate between depression in older people and dementia. One key difference is that people suffering from depression are more aware of the problem and more likely to complain about
symptoms (Blackmun, 1998). In 1998, Australian psychogeriatrician Professor Henry Brodaty developed a questionnaire to help GPs make early diagnoses of dementia (see Section 3.2.1). Feedback from GPs has been very positive, and
it is hoped that the questionnaire will assist a higher rate of early diagnosis in the future. Moreover, with better treatments and tests now available, GPs may now be more interested and able to diagnose AD.
GPs may also not be as effective as desired in acquiring up-to-date information on dementia and
dementia care, understanding the family's and carer's role and accessing a range of local support services available at different times. "Shared-care" initiatives, aimed at spreading information between
GPs and other aged care professionals, are under way to help inform and resource GPs for ongoing care.
Because most people with dementia are elderly, they may also suffer a number of other disorders,
which need to be treated by the GP alongside dementia (unless the illness is very advanced and an express desire not to treat at such an occurrence was documented when the person had mental
capacity). In many cases this requires the GP to be up-to-date on the most recent pharmacotherapies, their subsidisation arrangements and their interaction with other drugs for concurrent ailments of ageing.
"Please remember this: If we want GPs to play a central and continuing role in the care and
management of their patients who have dementia, they need to be trained in the role and remunerated accordingly."
Alzheimer's Australia (2001a)
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Specialists: Specialist neurologists, psycho-geriatricians, psychiatrists, physicians in geriatric medicine
and other consultant physicians are important in undertaking initial assessments of people for diagnosis, as well as ongoing assessments and treatment of people with dementia, including prescription of
medications, management in wards and nursing homes, and so on. There may be a battery of cognitive and behavioural tests, for example the Dysfunctional Behaviour Rating Instrument, to assess each
major cognitive and behavioural domain as well as functionality in ADL. Tests for depression and delirium may also need to be conducted, for example the Geriatric Depression Scale. Caregiver input or
direct observation are important in assessing functionality, as overstatement of abilities can be an issue. Occupational therapists can assist in functional assessments.
A neuropsychological assessment takes 45 minutes to two hours and possibly longer for people with
mild dysfunction. Strategies need to be put in place to avoid anxiety, which can affect test performance. Computerised instruments are now an alternative to paper-based tests, requiring less assessor time and
enabling a more accurate recording of time spent, although people need to be comfortable with the use of computers. Assessors need to consider factors that may influence test performance.
Other specialist therapies can include those listed in Section 1.2.4 under "specific therapies" and
possibly surgical intervention (see below), while the disproportionate use of specialist services is shown in Section 1.4.4. Specialist involvement in memory clinics is noted in Section 1.2.8.
Hospitalisation: As with other older people, acute care services are occasionally required by people
with dementia, whose average length of stay (ALOS) is four times that of people without dementia (DHA, 2000). Part of the reason for the long ALOS may be that individuals are awaiting entry to long-run
facilities, triggered by the event which led to the stay in acute care – a fall, for example. Acute care hospitals are not always well equipped to cater for the special needs of dementia patients, however.
Surgery: Two controversial potential surgeries are in the experimental stage, a shunt for cerebrospinal
fluid and a more radical omentum transplantation.
□ Shunts: A shunt can help drain the Aβ protein fragments away and increase the flow of
cerebrospinal fluid (CSF). Dr Gerald Silverberg, a Stanford US neurosurgeon, published results48
showing that experimental shunts in a small trial had slowed disease progression, with safe overall outcomes. An expanded, multi-centre, controlled clinical trial is now underway (Allen, 2002;
Barclay, 2002; Ajmani, 2002).
□ Omentum transplantation - Dr. Harry S. Goldsmith, at the University of Nevada School of
Medicine, places part of the omentum – a biochemical-rich membrane of fat and blood vessels in
the abdomen – directly on the brain. This is claimed to improve symptoms in people with AD, although further research is warranted to explain how (and how effectively) this surgery works.
1.2.6
Psycho-social interventions
Counselling and psycho-education: Appropriate counselling through all stages of dementia
progression is very helpful for the individual and the family. Psycho-education can help the person and
their family learn to manage certain symptoms - such as cognitive behaviour therapy to address misbeliefs (delusions) - and can help prevent secondary morbidity such as depression or anxiety.49
Because of the strong emotional impact of a dementia diagnosis, particularly younger onset dementias 48 Neurology (2002) 52:1126-1127, 1139-1145, 22 October. 49 For example, in treating depression resulting from moving Ms W to the confining environment of nursing home following
the independence of hostel accommodation, medication and hospitalisation were not helpful. Identifying the source of the
problem, loneliness, and organising a volunteer companion a few hours a day, resolved the depression.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
where there may be the additional stress of the knowing that children may be at risk, family counselling
and/or participation in support groups can be very helpful. Personality changes can be very difficult for spouses and families; for example, flat affect and low motivation that can be perceived as loss of love.
The problem-solving approach
Each problem is as unique as each person. There is no single tolerable solution and contributing factors may include the person's background, environment, habits, reactions and feelings. There are three
steps in planning the problem-solving approach: 1. Defining the problem
2. Assessing the person in the situation 3. Planning a strategy to solve the problem.
Miss Perkins causes a commotion each evening when she refuses to shower. After consulting her
sister, we restore her lifelong routine of showering in the morning and dressing ‘ready for work'. The problem is solved.
As a sales manager, Mr Grant frequently ate in expensive restaurants. At the day centre, having no
money to ‘pay' for his meal and leave a tip for the ‘waitress' distresses him. He eats little. His wife supplies him with some coins, restoring his dignity – and his appetite.
In her broken English, Mrs Berger repeatedly tells staff: "I worried … going to ask me leave … nowhere
go." If a member of staff accompanies her to her room, points to her name on the door and opens cupboards so that she can see and touch her clothes, she is content for a few hours. On the other hand
if she is ignored or told she is mistaken, she becomes agitated, noisy and demanding. She goes to her room, picks up the flexible shower hose in her bathroom and sprays around the room shouting, ‘Not
mine, not mine.'
Specific therapies: Physical, occupational and speech-language therapies can assist with specific
problems – for example, an occupational therapist can help maximise independence while identifying necessary modifications in the home or in driving. Diversional, reminiscence, validation, music,
movement/dance and craft therapies may be useful to calm, comfort and occupy people with dementia, particularly when they involve loved ones. Swimming and hydrotherapy can also bring peace and
quality of life. Massage, aromatherapy, light therapy, laughter, companionship and warm touch (from children or pets as well as other adults) may also be beneficial.50
Professor Faith Gibson, a leading proponent of reminiscence therapy in Northern Ireland, notes that
people with dementia can have very good long term memories and that tapping into these provides a means of affirming and including people with dementia and enabling them to "shine, perform, get things
right, rather than being constantly confronted with their shortcomings." Tools include old photographs, family albums and personal mementos, compiling ‘this is your life' books with family and friends,
questions about and listening to tales of the past, and so on. Validation therapy affirms the utterances of a person with dementia through an interested or warm response, rather than ignoring or minimising them. For example, a word or behaviour may be constantly
repeated, indicative of an unresolved worry. By validating the concern and asking sensitive questions about it, the therapist may be able to trace the source of the problem and allow relief, even closure.
50 For a recent study on the benefits of aromatherapy see Alistair et al (2002).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
"It is intuitively reasonable to expect that a life which involves the presence of others, which is
stimulating through variety of experience during the day, and which calls for personal initiative or self-expression, will be preferable for persons with dementia…. There is no evidence as yet that a
psychosocially enriched environment brings about any lasting benefit to cognitive function, but it does promote the quality of life of patients, and is of considerable importance in maintaining high standards of
nursing care."
Henderson and Jorm (1998)
Music therapy has also been recommended to increase melatonin in the blood, as well as helping
people to relax (Kumar et al, 1999). Musical ability and enjoyment may remain intact, as with long term memory, even into late stage dementia, and bring great joy and shared experience.
As a child, I recall visiting my grandmother and great aunt who both suffered from dementia. By the
time they were eventually placed in nursing care in Adelaide, neither could recognise me nor hold a conversation. My great aunt would count agitatedly for hours, while my grandmother went through a
very aggressive stage, which may have been due in part to her frustration at losing language skills. However, both would become calm and contented if my mother and I began to sing with them. As
though there was no problem, they would join in with gusto to songs in English and, in the latest stages, in their native tongue, continuing to sing peacefully even after my mother and I had left to go home.
Multicultural issues: Although people from non-English speaking backgrounds may have been fluent
in English, studies show that the most recent language is lost first for people with dementia. Sometimes
a mix of native and second languages is used for a time. Translation may be of little help, but it can bring joy to a person to hear their native language spoken or played on tapes. It is estimated that 25%
of Australia's population aged over 60 are post-war migrants, and 25% of them have a non-English speaking background. 12% of people in residential care are from culturally and linguistically diverse
backgrounds, with a variety of cultural customs, traditions and values. The composition of this group will continue to vary, from Eastern European, now at their age peak, to those from Southern Europe, the
Middle East and Asia, who will peak later. These Australians have equal right to access affordable, quality dementia assessment and care services, which can only be available for them if specialist
resources are developed to promote access. There is some evidence that people from some non-English speaking backgrounds may present later to services such as memory clinics, even if there is a
bilingual specialist available.
Peak community bodies: Community organisations such as Alzheimer's Australia and Carer
Associations are able to help meet a wide range of needs, including for information and resources about
understanding and managing dementia (libraries, pamphlets and electronic links), counselling (phone and face-to-face), support groups and membership benefits, programs for people living with early stage
dementia and for management of BPSD51 and so on, referral services, family carer education, training and support (through courses and seminars in community, hospital and residential settings), advice on
issues like driving, legal and financial planning for future health care needs, including preparing advance directives such as a living will, power of attorney, consent to participate in clinical trials, palliative care
and so on. Peak community bodies are also of key importance in advocacy and promoting public awareness, as for example 57% of adults are unaware of the links between cardiovascular risk factors
51 For example, the Alzheimer's Association's Safe Return Program, an identification program for memory impaired adults.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
and dementia.52 Peak bodies also deliver services such as mobile respite and federal programs.
Alzheimer's Australia manages the following national programs:
1. The Carer Education and Workforce Training Project: CEWT provides competency based
training and educational resources to families and carers and respite care workers.
2. The Dementia Education Support Program: DESP provides a basic level of support, education,
and short term counselling to people with dementia and their families and carers. Through the National Dementia Helpline (1800 639 331) this core program provides a key access point to
information, referral and counselling for people with dementia, their families and carers as well as other service providers.
3. The Early Stage Dementia Support and Respite Program: ESDSRP (usually referred to as the
‘Early Stage' program) provides people in the early stages of dementia and their families and carers
with information, education, counselling and support.
4. The National Dementia Behaviour Advisory Service: NDBAS is a national telephone service
designed to assist families and carers and respite care workers manage behaviours of concern.
"The course brought together people suffering from the same problem and there was an openness among us. Carers and sufferers were counselled in separate groups. People were able to discuss their
problems without embarrassment. Many realised for the first time that they were not freaks and that they were not alone. We saw our problems and frustrations mirrored in others. As our familiarity grew, there
was more chatter, laughter and, on some occasions, tears. At the end of the six weeks our understanding of the disease had increased and so had my confidence in my own ability to deal with it."
"I continued my membership with the Alzheimer's Association and became part of a small, local support
group. We met each month under the guidance of a professional social worker. We became a very close, caring group. We used to discuss very frankly what each member was going through. There was
always someone who had already experienced a particular phase and could enlighten the others. We managed to see the lighter side of Alzheimer's and would tell each other about any amusing events –
like the time Marjorie put the left-over roast through the dishwasher instead of back in the fridge. Our group continued to meet for eight years, after which everyone in the group apart from me had either lost
their relative or placed them in care."
Churches also provide a range of community services and support. Boden (1998) and others also point
to the peace found in personal faith. Hampson (2000) states that: "Faith can play a critical role for a person with dementia, and the opportunity to talk about God or faith may offer immeasurable comfort
and be life-affirming." "Everyone is going to ‘the other place' eventually; I want to do what I can to make my life as positive as possible. My friends have been terrific. The Christian community has been absolutely wonderful.
Everybody says to me, ‘You're so peaceful'. It's having God in my life that has made me that way. That's what gives me strength."
52 For details of this North American and European survey, see "Two thirds associate dementia with the ageing process",
www.NewsRx.com 23-9-02.

The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.2.7
Caring for families and carers
Carers Australia estimates there are at least 2.3 million Australians (one in every five households)
providing care for family members or friends with a disability, chronic condition or who are frail aged. Nearly 20% (450,900) of these are ‘primary' carers for people at home with severe or profound
disability. 70% are female and 90% are aged 60-69. Conservative estimates show that the ‘invisible workforce' saves the economy $16 billion annually and is the major provider of community care
services, delivering 74% of all services to people needing care and support (compared to the HACC Program, worth $1.1 billion in State and Federal funding, which meets only 9% of this need).
Most primary carers (78%) are of workforce age (aged 18 to 64 years) yet paid work is usually not
possible - 59% are not attached to the workforce. Over one-half of all full time carers reported incomes of less than $200 per week, while also experiencing the increased expenses of looking after another
person. 40% of primary carers have been providing care for a decade or more, and 68% for more than 5 years. 43% care for a partner, and 21% for a parent, and most primary carers (54%) said that they
provided care either because alternative care was unavailable or too costly, or because they consider they have no choice. Carers suffer from generally worse physical health, tiredness, stress, back/muscle
problems, depression, anxiety and lack of respite.53 For carers of people with dementia, specific additional stressors may also include:
□ difficult behaviours and symptoms, most commonly incontinence and the need for constant
supervision – days can be full of frustrations are repetitive chores;
□ broken sleep; □ the emotional involvement of the carer, for example, mourning the loved one's former competencies
and the loss of future hopes and plans;
□ ambiguities about their role as a carer – how long to continue, how and where to seek help,
(perceived) lack of support from other family members, "mistakes"/"failure" when there is no clear definition of "success", the impact of caring on the carer's life ("taking over");
□ impacts on the carer's relationships, eg. strain on marriages for carers of parents; and □ social isolation – friends disappear, it can be difficult to leave the house and social events are rare.
"The greatest cry I hear is that people feel they have no friends. Friends stop coming. I try to encourage people to keep going. Even if they just sit. Quite often there are things you can do to help."
Stressors tend to be lower, the better the quality of the past relationship between the person with dementia and their family
carer. Professional carers – service providers – can also, needless to say, experience considerable burnout and stress.
Counselling, regular medical checks, education, information, support and respite services are essential for families and carers,
result in improved health outcomes for families and carers and patients, and reduce or delay the demand on (more costly)
community and residential services. Carer programs are outlined in the previous section. Costs and benefits of dementia carers
programs are elaborated further in Section 3.3.
Above: Bill helps his wife Diane
with a card game.
53 Sources: AIHW, Australia's Welfare: 1999 Services and Assistance; Carers Australia, Caring Costs, 1998, Australian
Bureau of Statistics, Disability, Ageing and Carers: Summary of Findings, 1998. Cited on Carers Australia website.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
"It presents a challenge to a family to come to accept that this downhill course is pretty inevitable, and
yet may be slow, and that the caregiver's needs almost certainly will increase as time goes on," said Dr Williams, a geriatrician who formerly headed the National Institute on Aging. "And yet, the person who's
affected may still be functional in a number of ways and may still get some enjoyment out of things they enjoyed earlier," he noted. "It's a challenge to spot the things they still can get pleasure from… A former
housekeeper can contentedly fold the same laundry day after day. President Reagan's biographer reported that he enjoyed scooping leaves out of his swimming pool. Once he completed the task, Secret
Service agents accompanying him would surreptitiously add more and he'd keep going."
Rotstein (2000)
Care in the community
"Ageing-in-place" – bringing services and care to older people in their homes rather than moving them to
the services – has become a guiding social principle in most Western countries, including Australia since the 1985 Aged Care Reform Strategy, due both to concern for cost efficiencies as well as the
general premise that most older people prefer to remain in their own homes as long as they are able. Aged Care Assessment Teams (ACATs) – multidisciplinary teams linked with regional aged care teams and located in public hospitals (inpatient and outpatient areas) and community health centres – assess
and identify the physical, medical, psychological and social needs of older people and their families and carers, linking them to appropriate support services (eg, specialised rehabilitation services) and
managing comorbidities. ACATs generally include a combination of a geriatrician, nurse, social worker, occupational therapist and physiotherapist. They assess around 185,000 people a year, making
recommendations about whether the appropriate care setting for each individual should include additional community services and support, and which ones – a rising component in recent years as
shown in Chart 1 - or whether they are eligible for Commonwealth-funded hostel (low-care) accommodation or entry to a (high care) nursing home, these being fairly constant at 43-44% of
recommendations. Moving to special dwellings such as hostels of various forms (group housing for supported independent living) or residential nursing care may become desired as needs grow for
greater security, access to services and living comfort. The search for options between the extremes (home-based, nursing homes) is producing a spectrum of diverse alternative arrangements along the
care continuum.54
Chart 1: ACAT assessment rates and recommendations for services, Australia
H ig h care/nu rsin g h om e
L ow care/ho stel
C A C P s/C O P s
Source: Access Economics derived from appendix data in AIHW (2002a), Table A31.1
54 See Johansson, Chapter 1.4 in Wimo et al (1998).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
A range of support services is available in the community, both privately and publicly, including home
care, adult day care, day hospitals, and education and respite services for families and carers. The definition of community care is imprecise but includes personal care, health, accommodation and social
services for people with dementia and their families and carers, provided outside of formal institutions. The Department of Health and Ageing definition is:
"Community care describes a diverse range of services. Its main aim is to enable people to remain living in their own home and community. Community care is provided under a variety of
programs that are funded by both Federal and State Governments. Community care is accessed by a variety of people including: older people, younger people with disabilities, carers,
people with mental illness, people with acquired brain injury, people with chronic illness and people with dementia. Most community care programs charge their clients a fee for service.
The fee is often quite minimal."55
Memory clinics, first developed to provide outpatient services for people with mild dementia, are a
useful and important solution to coordinating dementia assessments and supporting the person with
dementia, the family carer and the GP. Some of these are State-funded, including 14 Cognitive
Dementia and Memory Services (CDAMS) in Victoria since 1997. CDAMs are multidisciplinary clinics including a specialist geriatrician, nurse, allied health professional and/or social worker and have access
to psychologists, psychiatrists, counsellors and other allied health professionals. Memory clinics have marked acceptability amongst doctors, people with dementia and their carers, and are especially useful
in improving assessment, with some randomised trial evidence for positive impacts on carer health. Community support services, such as Meals on Wheels, can be particularly important for single people living alone with dementia. Publicly provided community assessments for singles can make
recommendations and help with issues such as home modifications (eg, enclosing upper storey balconies), reminder alarms, lowering hot water temperature, removing electrical items from wet areas,
introducing a daily dose box for medication, changing bulbs and labelling essential items. It may be more difficult with singles for families to identify the right time to move into residential care. Children who
live elsewhere and phone or visit daily may not be on call to treat a fall or emergency immediately, precipitating an earlier entry into residential care than might be possible if co-located.
In Australia around half those diagnosed with dementia live in the community, assisted by a number of
Federal and State/Territory home-based and community care programs. Most notable is the Home
and Community Care (HACC) Program, whose services - in order of magnitude - include centre-based
services, domestic assistance (home help with cooking/meals, cleaning, errands, transport, home
maintenance and modifications), personal care, social support, home nursing and respite care (in-home respite is growing in popularity as the dislocation of day centre care can exacerbate disorientation for
the person with dementia). HACC provided 25.3 million hours of service to some 583,000 people including delivery of 8.4 million home meals in FY2001-02. The average age of HACC clients is 71.6
years, 66% are female, 93% are pensioners and 52% have a carer available to assist them. Up to one
in five HACC clients may have some form of dementia.
Community Options Projects (COPs) provide case management and individually designed service
packages, of which about 16% are for people with dementia. Community Aged Care Packages
(CACPs) were introduced in 1992, where a case manager provides a package of services to enable the
client to continue to live in the community. Of the 24,100 people who receive CACPs, 26% have mild dementia and a further 9% have moderate to severe dementia.56 These are like low level residential 55 See www.agedcare.org.au/factsheets/factsheet3_communitycare.htm 56 Data sources, also for HACC figures are AIHW (2002a) and DHA (2002a). The latter also states that ‘up to 5% of existing
low level residential care places may be converted to CACPs'. 1,150 new CACPs were released in 2002.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
care, but in the home, and are growing rapidly and also emphasising dementia. Extended Aged Care
in the Home (EACH) packages commenced in 1998, and are like high level care in the home and,
following trials, were granted additional extension funding in 2001-02 and 2002-03 Budgets. Other
Federal programs (some delivered through or in conjunction with Alzheimer's organisations, see Section 1.2.5 on Peak Community Bodies); include:
□ DESP - the Dementia Education and Support Program ($1.4m budget), including a helpline; □ the Carer Information and Support Program ($2m), for all carers; □ NRCP - the National Respite for Carers Program ($87.6m), including over 100 community respite
services for families and carers of people with dementia, plus three education and support
o CEWT - the Carer Education and Workforce Training Project ($1.1m) o the Early Stage Dementia Support and Respite Project ($1.5m) o NDBAS - the National Dementia Behaviour Advisory Service ($0.4m)
□ PGUs - Psycho-geriatric Care Units ($3.5m), with States; and □ Dementia Support for Assessment Program ($1.1m): rural and remote assessment and counselling.
Although fees are charged for community services, inability to pay does not preclude access. However, because demand outstrips supply, waiting lists are becoming problematic. More funding is required to
relieve the supply constraints in services that are provided through the formal sector.
Chart 2: Informal and formal caregivers for people with dementia in households
% with dementia needing assistance
Source: Access Economics based on ABS special data request, 1998.
Care from the informal sector, however, still exceeds that provided through programs. Chart 2 shows the proportion of people with dementia in Australian households who need assistance, who have carers
of various types in both sectors (the percentages are not additive). Over half have a child as a carer, while around 40% depend on a partner, on a for-profit organisation and on government. Around 5%
report having their care needs unmet. Chart 3 shows the proportion of people with dementia in Australian households who need assistance, by the area of the need as supplied by the informal and formal sectors (again the percentages are not
additive). Mobility assistance is the greatest need, required by over 80% of people, although the
requirement for assistance with property maintenance, health care, transport paperwork, meal preparation and housework are also very high (required by over 70% of people needing assistance).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Chart 3: Informal and formal types of care for people with dementia in households
th dementi
Source: Access Economics based on ABS special data request, 1998.
1.2.9
Residential Care
Even with the provision of the best home services, for most people there comes a time when the
transition to residential care is deemed appropriate. Entry into residential care is better predicted by
carer factors than by patient factors, possibility precipitated by an adverse event (eg, an accident or illness) or by carer burnout. It can be a difficult time for the individual and the carer(s), in terms of
confronting the terminal nature of dementia as well as the grief and other emotional and family upheavals that often transpire. Relinquishing full time care of a loved partner of many decades can be
traumatic, with mixed feelings of not being able to continue any longer, together with feelings of
desolation, guilt or failure and thoughts that the marriage is over (didn't their vow say "in sickness and in health?"), that they have deserted or been deserted by their spouse without consent or that they will be
perceived to be abandoning them, and fears that either they or their loved one will be unhappy, uncared for, lonely or alone. The family (particularly in some cultures) may not agree about the decision to place
the loved one in care, the timing of the move, or the particular accommodation, which can cause family stress.
As well as the emotional distress of placing a loved one in residential care, there are also well-
documented problems in gaining access to appropriate residential accommodation (see Section 3.2), and another key issue at the time of transition to residential accommodation is frequently money.
Weekly fees are means tested and limited to a proportion (85%) of the single age pension rate plus any income tested fee, and 16-40% of places must be for concessional residents, depending on the region.
However, there may be extra fees for certain therapies and the family home may need to be sold to pay for up-front costs (notably accommodation bonds), particularly if the desired accommodation provider is
an Extra Services Provider (ESP).57 Many families and carers (partners or children), seek levels of quality care that can be very financially challenging, either because they are unaware of the full costs, or
they feel bereft or guilty for placing their loved one in care, or simply because they want really good quality care for their loved one. Prudential protection (insurance) for the charges and bonds, either
through Medicare or private health insurance (PHI), might help to alleviate problems that sometimes arise in this regard.
There are two major divisions of residential care – low care facilities (formerly called hostels) and
high care facilities (nursing homes). High care facilities focus on the provision of continuous,
57 A maximum of 12% of places may be extra services places.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
intensive nursing care, while low-care facilities focus on personal rather than nursing services and
accommodate less impaired residents. For some families, great leaps must be made to accept the idea of changing from home help to residential care, and from hostel to nursing home care. Hostels provide downsized independent living;
they are homes away from home. They may offer comfy armchairs, bridge games and shopping expeditions. A nursing home is more hospital-like, perhaps with grey lino, crocheted rugs and walking
frames. Hostels lie somewhere between a retirement village and a nursing home. Some complexes provide all three levels of care… The quality of hostel accommodation ranges from Spartan to five-star.
Hampson (2000), p223.
Residents with dementia may be supported in either:
□ mainstream facilities, where residents with dementia and those without (frail aged) are integrated,
with no separate, locked or partitioned areas;
□ separated accommodation, where separation is achieved via dementia-specific wings attached to a
mainstream facility (with little or no contact with frail aged residents), dementia-specific units co-located on the same site as a mainstream facility, or in stand-alone dementia-specific facilities
(operating quite independently).
A small proportion of people with dementia are accommodated in psychiatric hospitals and, increasingly,
psycho-geriatric units. Chart 4, based on Gibson et al (1999) shows the distribution of people with dementia in various care settings – half in the community, one third in nursing homes, one in eight in
hostels and 4% in other facilities.
Chart 4: Care settings in Australia, % of total people with dementia
The community
Nursing homes
Supported
residential
geriatric
Source: Access Economics based on 1996 data from Gibson et al (1999).
There are currently 144,100 residential care places in Australia, of which 6,300 were released in
January 2002. The occupancy rate is 97% and the average age of residents is 83.2 years. About 64% of high level care residents enter from hospital, 26% from low level care and 10% direct from the
community. ALOS is 36 months with 35% staying less than 1 year and 22% staying more than 5 years.
Dementia-specific care: At least 60% of Australia's nursing home residents and 30% of our hostel
residents have dementia. Moreover, more than 90% and 54% respectively have an obvious cognitive
impairment (Rosewarne, 1997).58 Chart 5 shows the distribution of residential services, with mainstream nursing home beds dominant (nearly four in five beds). Moreover, dementia areas in mainstream 58 Levels of cognitive impairment for those in nursing homes were 10% none, 22% mild, 27% moderate and 41% severe,
while for hostel residents they were 46% none, 35% mild, 17% moderate and 3% severe.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
facilities account for another 15% of beds. Overall, however, only 5% of hostel and 6% of nursing home
beds are dementia-specific - mainly wings and co-located units.
Chart 5: Types of residential care services for people with dementia in Australia
Mainstream
Stand-alone
Mainstream,
dementia units
dementia area
Co-located specific wings
Source: Access Economics based on 1996 data from Gibson et al (1999).
Table 1 summarises care settings for people with dementia in Australia in 1996, based on Rosewarne et al (2000). This shows a slight fall since 1996 in the relative number of Commonwealth-funded high care
places, reducing the proportion of residential care in the total from 50% to 47.9%.
Table 1: Living arrangements for people with dementia, Australia, 1999
Commonwealth
Total living in
Supported
geriatric
residential Residential
The community
Dementia-specific beds
Mainstream beds
Co-located Stand-alone
Mainstream Mainstream with a
dementia area
Low-care
Source: Rosewarne et al (2000).
Dementia specific residential facilities have been very positive developments in the last two decades of
aged care in Australia. In the mid-1980s, large suburban houses were renovated and adapted, and early models emerged such as Aldersgate Village in South Australia and the CADE units of the NSW
Department of Health. In the 1990s, many ‘homely' dementia facilities sprung up, provided by Anglican Homes, Hammond Care, Frontier Services, Catholic Health providers and others. Capital costs were
higher (due to single rooms, ensuites), but the capacity to charge entry loans for most residents addressed this issue. Ongoing staff costs, however, were a real problem, to which the Commonwealth
Government responded with the Aged Care Act (1997) and single Resident Classification Scale across hostels and nursing homes. However, the decision later in 1997 (policy on the run) that no
accommodation bonds would be charged to nursing home residents is substantially reducing the incentives to invest in dementia specific care (see Section 3.2.2).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.3 PREVALENCE
1.3.1
Worldwide prevalence
As age advances, the risk of developing dementia rises sharply. Worldwide, the frequency of AD among
60-year-olds is about 1% after which the prevalence doubles about every 5 years, to around 2% at age 65, 4% at 70, 8% at 75, 16% at 80, and 32% at 85. It is estimated that as many as two-thirds of those in
their nineties suffer from some form of dementia.59 Table 2 shows the rising prevalence of dementia by
age-group over 60, for different continents, based on meta-studies to date.60
Table 2: Prevalence of dementia by age and continent
Age group
North America
Source: Wimo et al (1998), p14.
Prevalence is thus very dependent on the age structure of the population. Alzheimer's Disease
International (ADI) reports that in the year 2000 there were 18 million people in the world with dementia compared with 11 million in 1980. By 2025 ADI projects there will be 34 million with dementia of whom
25 million (71% of the total) will live in the developing world. Because developing countries are not so far along in their demographic transition, by 2025, there will be twice as many people with dementia in
the developed world as in 1980, but there will be four times as many people with dementia in the developing world.61 Where does Australia fit, now and in future?
Current prevalence in Australia
Australians in 2002
Table 3 shows the national estimated prevalence of diagnosed
dementia in 2002, by demographic cohort. The actual level (including
dementia, 0.8% of
a significant number of mild to moderate cases not diagnosed) is likely
to be much higher (see Methodology). It is noteworthy that current life
expectancy at age 65 for women is now 85 years, and for men is 82 years, and increasing.
Table 3: Prevalence of dementia in Australia, by age and gender, 2002 and 1993
Age group
Source: Access Economics, based on ABS special data request and international meta-analyses (see Methodology). Note
standard error may be relatively higher for the 25-64 age groups. Prevalence under age 24 was not statistically significant. 59 Life Extension Foundation (2002). 60 Differences between continents are due to methodological differences between studies, possible ethnic variations,
variation in diagnostic criteria, different survival rates and different geographical distribution of vascular risk factors. 61 ADI website.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Table 3 shows that in 2002 there were 162,300 Australians with diagnosed dementia of whom over
106,000 were women. Half of those with dementia were 85 years of age or older, and a further third were 75 to 84 years. Of those 75 or older, prevalence rates were higher for women than men, while in
younger age groups, prevalence was slightly higher amongst males. The higher prevalence for women in the age group over 85 years is partly attributable to the greater longevity of women who survive to an
age where the likelihood of dementia becomes extremely high. Similarly, in the 75-84 age group, the distribution for men is likely to be skewed more to the younger end than it is for women.
A comparison with the 1993 data, derived using the same methodology, is also of note, as the
prevalence has increased in all cohorts. This is partly due to increased longevity (particularly in the oldest cohorts) as well as increase in diagnosis (across the spectrum) over the past decade.
Another key issue is the significant number of younger people who have dementia, 6,600 in 2002 aged
under 65 (see Table 3). The impact on younger people can be even greater as they may be more financially exposed and have more children, family and career responsibilities. The services they need,
from diagnosis to residential care, are likely to be difficult to get or unavailable – because dementia care is still bound to aged care (Freeth, 1994).
A final point is in relation to indigenous Australians. Because fewer Aboriginal and Torres Strait Islander
people reach old age, there are fewer cases of dementia in these communities, in absolute numbers. However, the age-adjusted prevalence of dementia may in fact be higher in these communities than in
the Australian population as a whole – one study showed as many as 10% of indigenous people over 65 diagnosed with dementia, and another 10% with suspected dementia. Alcohol abuse and
cerebrovascular disease were found to be important causes of dementia, which are largely preventable (Henderson and Jorm, 1998; Pollit 1997).62
1.3.3
Projected prevalence in Australia
Prevalence of dementia is forecast to grow rapidly over
Over 580,000 Australians will
the coming decades due to population ageing. The
have dementia by mid-century,
projections in Chart 5 are based on ageing alone.
There is downside risk if new treatments, including
2.3% of the population.
pharmaceutical therapies and lifestyle changes, prevent
or postpone dementia.
Chart 6 : Projections of dementia prevalence and population growth, Australia, 2002-2051
Chart 6 shows projections of the prevalence of
dementia to 2051. By mid-century, the
Australian population is forecast by the ABS to
increase by 36%. The prevalence of dementia,
however, based on current prevalence rates by
demographic cohort, will increase nearly
% increase over 1998
fourfold, to 581,300 people. Prevalence will
reach the half-million mark around 2041.
Source: Access Economics projections.
62 1% of people in residential care are indigenous Australians.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.4 HEALTH AND SOCIOECONOMIC IMPACTS IN AUSTRALIA
1.4.1
The disability burden of dementia is severe – 98.5% of people with dementia are classified as disabled
compared with 19.3% of all Australians according to the definitions of disability in the 1998 ABS Survey of Disability, Ageing and Carers (see Methodology Section). Moreover, as Table 4 shows, 99.8% of
those with dementia who are disabled have specific restrictions, compared with 87.4% of disabled people generally. Even more telling, 94% of people with dementia who have restrictions are classified
as having "profound" core activity restrictions, compared with the average of 19%.
Table 4: Disability associated with dementia
core activity# restrictions
Total restrictions* disability
People (‘000)
60 4 0 0 64 64 64
mental/behavioural 158 92 53 93 396 480 529
Total with a disability
598 660 1,032 2,828 3,156
% of total**
93.9% 6.0% 0.0% 0.2%
100.0% 99.8%
mental/behavioural 39.8% 23.3% 13.3% 23.6% 100.0% 90.6%
15.6% 20.8% 25.0% 38.6% 100.0% 86.9%
19.0% 21.2% 23.3% 36.5% 100.0% 87.4%
#Core activities comprise communication, mobility and self-care. * Includes schooling and employment restrictions. ** First
five columns are relative to the total number of people with core activity restrictions; sixth column is relative to all those with a disability. Source: Access Economics, derived from ABS (1999), Table 10 for 1998.
1.4.2
Socio-economic status and rurality
People with dementia tend to have lower incomes. Over 70% of people with dementia have income in the lowest two quintiles – that is, compared with the lowest 40% of the general population (Table 5).
The distribution between those in capital cities and those in rural and remote areas, however, is roughly similar (Table 6).
Table 5: Income of people with dementia
% with dementia
Income quintile
in quintile
Total 100.0% Source: Access Economics based on ABS special data request, 1998.
Table 6: Urban-rural distribution of people with dementia
% with dementia
% of total
Balance of State
Total 100.0%
Source: Access Economics based on ABS special data request, 1998.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
1.4.3
People who have dementia are under-represented in Australian employment. Table 7 shows that only 2.3% of those aged over 65 who have dementia are employed, compared to 8.5% of the population as a
whole. The sample of those employed with dementia was too small to permit a statistically significant subset to establish absenteeism rates relative to the population as a whole. It is more possible to
remain employed for a time if the illness is in the early stages, if the work environment is supportive, if tasks are familiar or repetitive and if supervision and occupational health and safety arrangements are
adequate. Inadequacies in the latter for self-employed people may necessitate earlier retirement for them. For many employed people, workmates may be the first ones to notice changes pre-diagnosis in
gradual onset cases of dementia.
Table 7: Proportion of people aged 65+ employed, with dementia and total
All Australians
Australians with dementia
* Includes those not in the workforce and those looking for work.
Source: Access Economics, based on ABS special data request, 1998.
Christine Boden was 46 years old when diagnosed with younger onset AD, formerly a federal
government senior executive. She writes: "After the final diagnosis by the second specialist in mid-September 1995, I faced the task of seeking retirement on medical grounds… My battles with the
superannuation company epitomise the misunderstanding about Alzheimer's as a killer disease… The suggestion that I return to work for retraining [in a lower level job] appalled all the medical people
associated with my case, as well as my department and … the Alzheimer's Association. We all knew at least the basics of Alzheimer's: that the first capacity to be lost is holding a job and that, in particular,
learning any new tasks is almost impossible for someone with the disease. And here was the suggestion that I should not only continue to try to hold a job, but learn a completely new one, with a
whole range of new tasks, new places to find, new colleagues to recognise! … It would mean driving through heavy traffic… remembering a whole list of issues, learning (or rather coping with the
embarrassment of never remembering) so many new things. I became very distressed… with continual migraines again, and rapidly increasing confusion… The specialist warned that stress would
exacerbate the progress of the disease." Four months later, when the board agreed to retire Christine, she was "speechless with relief".
Boden (1998), p41-44.
1.4.4
Use of medical services
People with dementia go to the doctor more frequently than the average Australian, and also more than others their own age. Table 8 reflects that 36.6% of those with dementia visit their GP in a fortnight,
significantly more than the average for all Australians of 21.0%, and slightly more than those over 65 (35.6%). For specialist visits, the difference is even more pronounced, with more than double the
proportion of those with dementia (9.2%) visiting a specialist in a representative fortnight compared to the average 4.1% of Australians, and a third as much again as the average of those their own age.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Table 8: Proportion of people with dementia visiting the doctor, 1998
People with
All Australians
Visited GP in last 2 weeks
Visited medical specialist in last 2 weeks
Source: Access Economics, based on ABS special data request and ABS (1997), Table 14 for last two columns.
Epidemiological studies have confirmed the higher utilisation of health services, and hence higher direct
health costs, of people with dementia compared to those without, adjusted for age, gender, location and co-morbidity. Gutterman et al (1999) found that:
□ hospital stays were twice as long on average and emergency department costs 2.5 times greater; □ hospital, medical and pharmaceutical costs were 1.5 times higher (not including nursing home
costs), although pharmaceutical costs and outpatient costs were not significantly different;
□ 75% of the disparity was linked to greater inpatient care.
1.5 INTERNATIONAL COMPARISONS
"While Australia is
The dementia epidemic is worldwide. In demographic terms,
relatively young in an
Australia is quite "young" among developed nations – the
international context, it is
"oldest" countries being in Europe and, particularly
Scandinavia where although the proportion of those aged 65
is already over 15%, the growth of this age-group is
comparatively rapid rate of
stabilising (below 1%). In comparison, Australia, with only
population ageing."
12.5% of the population over 65, has the 65+ cohort growing
Gibson et al (1999)
at 1.8% p.a. and the 85+ cohort growing at 4.6% p.a., as our longevity is one of the highest in the world. Thus, Australia's
demographic transition is occurring relatively markedly.
Chart 7: People over 65 receiving home-based services and residential care, internationally
Source: Gibson, Benham and Racic (1999) for the year 1995.
The projected rapid growth of dementia prevalence depicted in Chart 6 is occurring throughout the
western world. However, the extent or type of care provided is not closely related to the stage of
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
demographic transition, as Chart 7 shows, although the Nordics still lead the way. The levels and mix of
home-based and residential care services provided varies greatly, with Australia in the middle of the range.
The proportion of national income spent on public programs for the aged is slightly more strongly
correlated with the stage of demographic transition, as shown in Chart 8. For a "young" country, Australia is spending close to the OECD average on the health and long-term care for the aged, aged
pensions, early retirement and other expenditure for the aged.
Chart 8: Age-related expenditure, % of GDP by OECD country, 2000
New Zealand
Percentage of GDP
Source: Access Economics derived from appendix data in AIHW (2002a), Table A4.2.
1.5.1
North America
In the US, the number of people with AD is forecast to increase from 4 million in 2002 to 14 million by mid-century. Dementia care costs are also increasing rapidly, with the total direct and indirect cost of
AD alone estimated to exceed US$100 billion each year – US$25,000 per person with dementia on average.
This figure includes care expenses and lost earnings both of the person and family members.63 More
than 70% of people with AD in the US live at home and almost 75% of the home care is provided by family and friends (valued at US$34,518 pa in 1990 by Rice et al, 1993 – see Chart 9). The remainder is
formal sector care costing an average of US$12,565 per year, which families pay almost entirely out-of-pocket (neither Medicare nor most private health insurance covers the long-term care most people
need). Half of all nursing home residents in the US suffer from dementia. The average cost for nursing home care is US$42,049 per year but can exceed US$70,000 per year in some areas of the country.
The person or their family provide a further US$5,542 in additional goods and services while the resident is in care. Leon et al (1998) showed annual costs of caring for a person with mild, moderate or
severe AD to be US$18,408, US$30,096 and US$36,132 respectively, with 21% of the total costs being for informal care (half the Rice proportion). The average lifetime cost per person was estimated as
US$174,000 in 1991, including US$47,581 in direct costs. Spending on AD research was US$600million in FY2002.
63 Alzheimer's Association of the United States, www.alz.org
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Chart 9: Cost of dementia care per person, United States
Nursing home
Source: Rice et al 1990 study reported in Wimo et al (1998) p200.
A summary of cost of illness studies in the US is provided by Max in Wimo et al (1998, p200). Even the
data above shows there is some divergence in US cost estimates, which range from US$20,000 to US$25,000 per person64 per annum (around A$40,000 to A$50,000 at 2002 exchange rates).
Two recent studies that have looked at costs of informal care and to business are described below:
1. A large 2001 University of Michigan study estimates that informal care costs for dementia in the
US are $18 billion a year, based on observations of families and carers of over 7000 Americans
aged 70 or more, 10% of whom showed cognitive impairment consistent with dementia (43% mild, 27% moderate and 30% severe). Time spent on assistance with ADL - dressing, bathing,
eating and so on - increased from 4.6 hours (no dementia) through 8.5 hours a week extra (mild) to 41.5 hours extra with severe dementia. Time spent managing the BPSSD was not
included. The hours of care given was multiplied by the average weekly wage of a home health aide. Most of the care burden was found to be borne by elderly spouses. 65
2. The second study, of the cost of dementia to US businesses, showed an estimated $61 billion
spent on AD, which had doubled between 1998 and 2002 (Alzheimer's Association US, 2002b).
The cost breakdowns show costs of health care at 40% ($24.6bn) and carer costs at 60% ($36.5bn), including productivity losses (30%, $18bn,) absenteeism (17%, $10bn), worker
replacement costs (10%, $6bn) and continuing insurances and temporary replacements (3%, $2bn).
The prevalence of dementia in Canadians aged 65 and over has been estimated at 8% (5% with AD), amounting to over 250,000 people. Projections indicate that by 2021, there will be almost 600,000
Canadian seniors with dementia, increasing to 778,000 in 2031. As in Australia, half of those with dementia live in the community and half are institutionalised; with the former generally with less severe
forms of dementia. 64 Using the data above, 75% (3m people) live at home costing $12,500 per person = 37.5bn plus 1m at $42,000 each = US$79.5bn, suggesting US$20,000 per person for 4m people. Alternatively, lifetime costs of $174,000 with average life
expectancy of eight years suggest average cost of US$21,750 per person. $100bn in total with 4m people suggests average
costs of US$25,000 per person. 65 Dr Susan Aldridge, The cost of dementia, on www.healthandage.com. For the full article, see Journal of General Internal Medicine, November 2001. These care hours may be quite conservative – a 1985 US study showed the average care hours
for mild and moderate dementia to be 22 and for severe dementia to be 56. An Italian study showed 45 hours of personal
care required and 18 hours of other non-medical services (Lowin et al, 2000).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
In a 1991 study by the Canadian Study of Health and Aging (CSHA) published in the November, 1994 issue of the Canadian Medical Association Journal, annual net costs for people 65 years of age and
older were very conservatively estimated at $3.5 billion (A$3.9 billion), or about C$14,000 (A$15,575) per person with dementia per year.66 The total figure comprised community costs of almost $1.3 billion
(33%), costs to long term institutions of almost $2.2 billion (56%), drug costs of $60.6 million (1.6%) and diagnostic costs of $13.5 million (0.3%). The total annual net costs for people under age 65 were $389.2
million. Dementia was estimated to be 4.9% of health costs in 1991 but 5.8% by 1994. Net average cost of community care for moderate and severe patients was 2.27 times more than for mild patients.
Research for both groups accounted for only $9.8 million – A$10.9m.67
1.5.2
In the UK, over 700,000 people have dementia, with prevalence of 1 person in 120, estimated as 1 in
1000 for people aged 40-65, 1 in 50 for people aged 65-70, 1 in 20 for people aged 70-80 and 1 in 5 for
people over 80. 68 There are 18,500 people under the age of 65 in the UK who have dementia, with the prevalence between 30 and 60 years of age 67.2 per 100,000.69 AD is estimated to cause 55% of
dementia, vascular dementia 20%, dementia with Lewy bodies 15%, fronto-temporal dementia 5% and other forms 5%. By 2010 there will be about 840,000 people with dementia in the UK, expected to rise
to over 1.5 million by 2050. 70 The annual cost of dementia in the UK was estimated in the 1993 to be between £5.4bn and £5.8bn. Of this, £1bn were direct health and social services costs to the public sector. The direct cost of younger
people with dementia was estimated at £132 million per year.71 By 2000, cost estimates of AD in the UK had increased to between £7.1 billion and £14.9 billion (A$20.2 billion to A$42.8 billion) or A$44,473 per
person on average72, excluding costs of mortality and lost productivity. The NHS and local authorities pay for about 42% of total costs, the rest being borne by the Department of Social Security or people
with dementia and their families. Costs of formal care are dominated by institutional care, particularly in hospitals and nursing homes where one estimate puts the full costs of care at £278.86 per week for mild
to moderate illness (A$41,625p.a.) and £338.38 per week (A$50,510 p.a.) for severe illness; while the person is at home, informal care costs are typically much larger than the paid cost of formal care. Costs
are estimated to increase to £10.7bn to £20.7bn by 2021. Research costs are only £5.6m per annum for AD (Lowin et al, 2000).
O'Shea (2000) showed the costs of caring for a patient with AD in Ireland in 1996 were £328m to £453m
or between £10,933 and £15,100 per person per annum, equivalent to A$31,385 and A$43,345 respectively. He notes that these estimates "come at the lower range of published estimates in the
international literature". The division of costs in this study (for the lower end of the spectrum) was: carer costs £154m (47%), residential care £82 (25%), GPs and community care £16 (5%), psychiatric
hospitals £14m (4.3%), acute hospitals £5m (1.5%), and other costs £57m (17%).
66 Østbye T and Crosse E (1994) "Net economic costs of dementia in Canada" Can Med Assoc J 1994;151(10):1457-64. 67 Larry Segel The Underwriting Edge, on www.marketingoptions.com/c_ls124.htm . 68 Bosanquet, May, Johnson (1998) "Alzheimer's Disease in the United Kingdom - Burden of Disease and Future Care". 69 Harvey, (1998) "Young Onset Dementia: Epidemiology, clinical symptoms, family burden, support and outcome" 1998. 70 The Alzheimer's Society web site, www.alzheimers.org.uk . 71 Bosanquet et al (1998) ibid and Harvey (1998), ibid. Also Alzheimer's Europe (2002) for the cost per person. 72 Lowin, McCrone and Knapp (2000) "Cost of Alzheimer's Disease and Level of Research Funding". Souetre et al (1999)
estimated the total cost per patient over three months as an enormous £6,616 (mild), £10,250 (moderate), and £13,593
(severe) – equating to A$75,966, A$117,693 and A$156,078 per person with dementia p.a. respectively!
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Costs of dementia in other European countries range considerably, from 19% of total health care costs
in Sweden, by far the highest, to around 5.6% in the Netherlands (close to the average). Chart 10 shows the Dutch direct health costs predictably dominated by nursing homes (around two thirds of direct
costs), followed by hostels (30%), with specialist psychiatric services, hospital costs, home-care, GPs and pharmaceuticals together accounting for less than 5% of total heath system costs.
Chart 10: Costs of Dementia in the Netherlands
Specialist
Source: Access Economics derived from Koopmanschap et al in Wimo et al (1998).
In terms of per capita expenditures in Europe, studies in France and Germany show direct costs in the order of US$6,778 and US$11,661 respectively for 1991 and 1995, although different methodologies
and variable exchange rates make close comparisons of these low estimates difficult. Costs in Europe are projected to grow on average in real terms by around 1.9% p.a. for 1985-2020 and 2.6% p.a. for
2020-2040 (Koopmanschap et al in Wimo et al,1998). Perhaps the most frightening statistic in recent research in Europe was that 41.8% of people diagnosed with AD did not receive further information on the disease or on existing services and treatment.73
Within this international context, we now turn to cost estimates for Australia.
1.6 SUMMARY OF CHAPTER ONE
Dementia is a disabling organic brain syndrome characterised by progression from mild, through
moderate, to severe illness, with death after an average of eight years. Symptoms include loss of
cognitive abilities, behavioural and psychological symptoms, and functional disability. Diagnosis can be
complex. There are many diseases that cause dementia with varying symptoms and progression, the
most common being Alzheimer's disease (AD), vascular dementia, dementia with Lewy bodies and fronto-temporal lobe dementia. The most established risk factor is age; others include family history,
gender and cardiovascular risk factors, while protective factors may include use of anti-inflammatories, oestrogen and statins as well as intake of antioxidants.
Prevention of dementia is currently focused on postponing the onset of symptoms to later in the
lifespan, increasing healthspan and potentially preventing tens of thousands of institutionalisations per
annum. Research is promising – with the best chances for AD elimination possibly related to an
73 Alzheimer Europe (2002), p1.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
immune system response that destroys beta-amyloid plaques in the brain. Research is also vital to find
more effective models of care for people with dementia. Early diagnosis and intervention are
paramount, ensuring the person and the family can benefit from the many advantages of drug
treatments, support and planning, which improve coping and quality of life.
Pharmacological management includes cholinesterase inhibitors (CEIs), which ameliorate the
symptoms of illness but do not reverse disease or prolong life. Three of these – Aricept, Exelon and
Reminyl – are available on the PBS for mild to moderate AD under certain conditions, including demonstrated improvement. Other pharmacotherapies can include aspirin and blood thinning agents,
anti-psychotics, memantine (not yet TGA-approved) and a range of natural treatments such as Ginkgo biloba, Vitamins C and E and folic acid.
GPs play a key role in medical treatment – recognising, assessing, planning, managing, referring and
supporting the person and their carer. However, only half of GPs are able to recognise mild dementia and more information and resourcing is required. Neurologists, psycho-geriatricians and other
specialists also have a key role in assessing, treating and prescribing. Acute hospital care for people
with dementia has four times the ALOS (average length of stay) of the general population.
Multidisciplinary memory clinics are a useful, important and accepted new community solution (with
specialist input) to coordinating dementia assessments and supporting the person with dementia, the
family carer and the GP.
Psychosocial interventions are very important for disease management and quality of life, including
counselling, psycho-education, understanding of behavioural and psychological symptoms of dementia
(BPSD), problem-solving strategies, person-centred care, modelling and specific therapies such as physical, occupational, diversional, reminiscence, validation or music therapies. 25% of Australian older
people are from non-English speaking backgrounds, requiring special consideration or services.
Community bodies, such as Alzheimer's Australia and Carer Associations are able to meet a wide
range of community needs including information, resources, support, education, counselling, referral, legal and financial services, advocacy and program delivery. For example, Alzheimer's Australia
delivers Commonwealth-funded national programs that include the Dementia Education and Support Program (DESP), which includes the Dementia Helpline service; Carer Education and Workforce
Training (CEWT); Early Stage Dementia Support and Respite Program (ESDSRP); and the National Dementia Behaviour Advisory Service (NDBAS). Private and public community support services are
also available, although not equitably or comprehensively, including personal, health, accommodation and social services such as home care, adult day care and a variety of respite services.
"Ageing in place" is a fundamental element of dementia and aged care generally in Australia, where
community-based aged care assessment teams (ACATs) assess needs and recommend appropriate
care services and settings in the community or in residential care. 52% of people with dementia live in
the community and are key users of services such as Home and Community Care (HACC), Community Aged Care Packages (CACPs), Extended Aged Care in the Home (EACH), psychogeriatric units
(PGUs), the Carer Information and Support Program, the National Respite for Carers Program and the Dementia Support for Assessment Program. Over half of people with dementia have a child as a carer,
while 41% depend on a partner and 35% on another relative. 40% use for-profit care services and 40% use government services. Greatest needs are for mobility, property maintenance, healthcare, transport,
paperwork, meal preparation, housework, self-care and communication. Informal (voluntary) families
and carers – the invisible multi-billion-dollar workforce – provide a huge contribution, which often may
take a heavy toll on their own health, wellbeing and income.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
As dementia progresses, and depending as much on carer as patient factors, entry to residential care
may become appropriate – either low-care (hostel) or high care (nursing home). Quality of care remains an issue, with physical and chemical restraint still used by a majority of providers, and a long way to go
in achieving widespread person-centred care strategies. Two thirds of people with dementia in residential care are in nursing homes, one quarter in hostels and 8% in psychogeriatric facilities or other
supported residential services. ALOS is 3 years. Although 60% of nursing home residents and 30% of hostel residents have dementia, and over 90% and 54% respectively have an obvious cognitive
impairment, 79% of residents are supported in mainstream facilities. Only 6% of beds are dementia-
specific, with the remainder being dementia areas in mainstream facilities.
In Australia there were over 162,000 people with dementia in 2002, including 6,600 under 65 – with
‘younger onset' dementia. Age-standardised prevalence for indigenous people may be higher. Prevalence of dementia in older people doubles every five years from 1% at age 60, to 2% at 65, to
32% by 85 and to two thirds of those in their nineties. The prevalence of dementia is growing rapidly –
reaching the half-million mark around 2040 and 2.3% of the population by mid-century.
The socio-economic and disability burden of dementia is severe – 98.5% of people with dementia
are disabled. People with dementia also tend to have lower incomes, with 70% represented in the lowest two income quintiles. Rural and urban prevalence distribution is similar, although access to
services is more difficult in the bush. People with dementia are under-represented in Australian
employment – 2.3% compared to the Australian average of 8.5% for people over age 65. People with
dementia also have higher than their age-average use of medical services including doctor visits and specialist visits, as well as longer hospital stays and higher age-standardised pharmaceutical costs.
The dementia epidemic is worldwide. As demographic ageing progresses, we witness another
epidemiological transition. The management of neurodegenerative disease is the major challenge of health care systems all around the globe. Costs in the United States are estimated at between
A$40,000 and A$50,000 per person per annum - US$100bn in total each year. North American and
European studies point to the concentration of huge costs in residential care services as well as on
informal family carers, and potentially enormous cost-savings of postponing the severity of disease.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
2. THE DEMENTIA BURDEN FOR AUSTRALIAN PEOPLE
There are three types of costs associated with dementia (see also the Methodology for this chapter):
□ Direct financial costs to the Australian health system include the costs of running nursing homes
and hospitals (buildings, nursing, consumables), GP and specialist services reimbursed through
Medicare and private funds, the cost of pharmaceuticals (PBS and private) and of other medications, allied health services, research and "other" direct costs. The latter category includes
institutional and non-institutional expenditures (such as day-care programs, home-based care and respite) and health administration. These are analysed in Section 2.1.
□ Indirect financial costs (Section 2.2) tend to be borne primarily by people with dementia and those
who care for them. These are dominated, in the case of dementia, by the costs of care – including
the value of all care whether it is provided through the formal or informal (voluntary) sector. The income forfeited by people with dementia and their families and carers, due to absenteeism and
early retirement, is also significant. Other costs include equipment and devices that are required to help cope with the illness, and transfer costs such as welfare and disability payments.
□ Non-financial costs (Section 2.3) are also very important—the pain, suffering and premature death
that result from dementia. Although more difficult to measure, these can be analysed in terms of the
years of healthy life lost, both quantitatively and qualitatively, known as the "burden of disease".
2.1 DIRECT HEALTH COSTS
Direct health system costs estimated in this paper are based on DCIS prevalence-based methodology
developed by the Australian Institute of Health and Welfare for the year 1993-94 and currently being
updated. This report extends and projects the AIHW work to estimate those costs attributable to dementia in CY2002 (see Methodology).
2.1.1
Direct costs in 1993-94 and 2002
Table 9 shows the AIHW 1993-94 data, where dementia is already the most costly of mental health
disorders at $714 million, accounting for nearly one quarter of all mental health system costs in 1993-94. Spending in the ‘other direct' category ($582m), mainly nursing homes and hostels, dwarfs that of other
mental illnesses and is still grossly under-estimated (see Methodology). Community care was separate spending under the Aged Care program budget in 1993-94.
Table 9: Comparison of the direct health system costs of mental disorders, $m, 1993-94
health Other
Hospital Medical ceuticals services direct Total
9
582
Affective disorders (inc. depression)
Substance abuse disorders
Anxiety disorders
Behavioural syndromes
Other non-drug psychosis
Stress and adjustment disorders
Disorders of childhood and adolescence
Other disorders, prevention & screening
334 1110 3022 100.0%
Source: Mathers, Vos and Stevenson(1999), p90, Table 6.6, condensed.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
By 2002, the costs of dementia were estimated as $3.2 billion, due to a 62% increase in the number of
people with dementia over the period, a 37% increase in costs, and an original underestimation of the residential care component (see Methodology). The distribution of these costs across the health system
is shown in Table 10.
Table 10: Components of direct health costs for dementia, 2002
Direct health cost
% of total
Nursing homes and hostels
Public hospitals
Psychiatric hospitals
Private hospitals
GPs and specialists
Outpatients & other ambulatory services
Pharmaceuticals and allied health
Other direct costs
Source: Access Economics, based on AIHW special data request.
Chart 11 illustrates the breakdown of cost components for dementia. Residential care costs dominated the profile at $2.8 billion (88% of the total). This represents 66% of total Commonwealth residential care
subsidies in FY2002-03, estimated to be $4.3 billion, which fits well with Rosewarne data, while not attributing all costs of people with dementia to dementia74. Second are public hospital costs at $141m
(4.4%) followed by psychiatric hospital services ($75m or 2.3%). Private hospital services ($28m), medical services ie, GPs and specialists ($24.5m), outpatient and ambulatory services ($20.6m),
research ($19.2m) and pharmaceuticals and allied health ($13.2m) were each less than 1% of the total. Other direct costs, including health administration, were $67m (2.1%).
Chart 11: Components of direct health costs for dementia, 2002
Nursing homes and
Other direct costs
Pharmaceuticals and
GPs and specialists
Outpatients & other
Source: Access Economics based on AIHW data. 74 In Section 1.2.6 we saw that Rosewarne's data suggests 60% and 90% of nursing home and 30% and 54% of hostel
residents are effectively the minimum and maximum with dementia. Gibson's data show that weightings for nursing homes
and hostels in total residential care are 70% and 30% respectively for people with dementia (see Chart 4). The weighted averages are thus 51% and 79%, with the mean 65% of total residents having dementia. Costs per patient, however, are
higher for dementia patients – hence 66% is conservative, although ballpark if an allowance is also made for those with
multiple disorders. These figures conservatively concord with international data from Section 1.5.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
2.1.2
Projections of direct costs
Section 1.3.3, particularly Chart 5, depicted the rapid growth of dementia
prevalence over the coming decades. Given these demographic growth
The health care
trends, together with growth in health care costs (based on trends in the
costs of dementia
Health and Community Services GDP deflator), the direct health costs of dementia are estimated to grow by 82% by 2011 (see Methodology). If
will nearly double
we also make an allowance for increased spending on research, GPs
this decade.
and pharmaceuticals, then direct health costs are estimated to grow by
84% to $6.0 billion. This ignores the potentially even faster growth of home-based aged care spending on dementia, which may need to reflect increased women's labour force participation resulting in a
reduction in "free" caregiving. Table 11 shows a breakdown of projected costs for 2011.
Table 11: Projected components of direct health costs for dementia, 2011
Nursing homes and hostels
Public hospitals
Psychiatric hospitals
Private hospitals
GPs and specialists
Outpatients & other ambulatory services
Pharmaceuticals and allied health
Source: Access Economics projections.
It is always difficult to predict technological change, and it should also be noted that any increase in
pharmaceutical spending, as new therapies become available, could be expected to have an offsetting effect on other medical costs, and also on indirect costs. Also important in projections is the policy
response to the current inadequacies of residential and community care, carer programs, early intervention and research programs. If spending on these components is addressed in a significant way,
there may be compositional and other effects on projected direct and indirect costs. We now turn to current estimates of the home and community care costs of dementia.
2.1.3
Home and community care costs
Home and community care costs (not included in direct costs for reasons given in the Methodology
section) are derived from the proportion of the HACC program that is estimated to be spent on care for people with dementia – 20% of current Federal spending ($674 million) or $135 million75 – plus
spending on other dementia-specific programs (such as funding for Alzheimer's Australia) which is estimated as $40m in 2002.76 The total, $175 million, represents $2,071 per person at home with
dementia (52% of the total prevalence, or 84,394 people). Taking account of those who may not access the services (about 19%), the average cost is $2,554 per person p.a. for those receiving them. This
amounts to 16% of Department of Health and Ageing (DHA) spending on home and community care.
75 The total HACC program, including State and Territory spending, amounts to $1.1 billion. 76 Unpublished DHA estimate.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Home and community care provision is significantly less costly to the public purse than residential care,
as expected, which from Section 2.1.1 amounted to $2,847 million or $36,547 per person in residential care in 2002. This is, as expected, above the DHA published estimate of $28,796 per person for all
people in residential care, with or without dementia. The spending represents around 66% of aged care
spending on residential care, $4.3 billion in 2002-03. A summary is provided in Table 12 below.
Table 12: Dementia Formal Care Costs, 2002
per person
per person at
receiving
services % of total DHA
Home-based Aged Care
DHA av. cost
per person in per occupied
place % of total DHA
Residential Aged Care
per person
per person
receiving
$m with dementia
services % of total DHA
Source: Access Economics
2.2 INDIRECT FINANCIAL COSTS
2.2.1
Lower workforce participation of people with dementia
People over 65 with dementia have lower rates of employment than healthy people of the same age (as
noted in Section 1.4.3), due to functional and cognitive disabilities. Table 7 showed that the employment
rate for those with dementia is 2.3% compared to 8.5% in the general population. If older people with dementia achieved the same employment rate, there would have been an extra 9,612 people in the
workforce in 2002, earning an average of $696 per week, all other things being unchanged (see Methodology). This would have produced $348.8m in extra income.
This figure may be a conservative estimate of the true loss as many people (particularly those under 65
who have not been included here) may reduce their workload rather than stop work completely, as a result of the health impacts of dementia. Income losses of families of people with dementia who reduce
or give up work in order to care for the person with the illness are identified in the next section. "Mavis and I looked forward to the day I would retire. We had so many travel plans. We wanted to do so much when that time came. Unfortunately, retirement came too early and was unplanned. All our
dreams have receded and we now deal with the reality of Alzheimer's."
Margaret and Bill Carmen had been married for 19 years. At only 43, Margaret suddenly began to show
signs of dementia and was diagnosed with Alzheimer's disease. A high school biology teacher, she had to give up work. Later her husband gave up his job to care for her full time.
Hampson (2000), p18.
Absenteeism: There were an estimated 3,606 people employed, over age 65, with dementia in 2002,
earning an estimated $130.8m. Although data on absenteeism rates for Australian people with dementia
who work are not available due to small sample size, a conservative estimate is likely to be around 5%
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
of work time lost (based on 8% lost for people with psychotic illnesses with similar cognitive and
functional impairments). The cost of absenteeism would thus be a further $6.5m.
In total then, the loss of earnings from loss of employment and absenteeism is estimated for 2002 as
$355.3m.
Potential tax revenue foregone: There are two sources of lost tax revenue that result from the lower
earnings above—the potential income tax foregone and the potential indirect (sales) tax foregone. The
latter is lost because, as income falls, so does consumption of goods and services. Table 13 summarises the tax losses of $100m in 2002, comprising $77m of personal income tax and $23m of
indirect tax.
Table 13: Potential earnings and tax revenue lost due to dementia, 2002
Potential Earnings Lost
Average personal income tax rate#
Potential personal income tax lost
Average indirect tax rate#
Potential indirect tax lost
Total potential tax revenue lost
# Source: AEM Model, Access Economics.
Mortality burden: In addition to the income foregone due to those with dementia in the community who
are unable to work due to their illness, there is also the income foregone of those who have died
prematurely due to dementia. Deaths from dementia in 2002 are estimated as in Table 14. These are
likely to be significantly under-estimated (see Methodology) so the cost estimate of the mortality burden is very conservative. Assuming that if those who died prior to retirement age had lived and not had
dementia, they would have been employed at the same rate as the general population over 65 – 8.5% (39 people in all would have been employed who were not because they died from dementia). The
average age of death for those people aged 15-74 is 64.2 years (i.e., with 5.8 years to ‘average' retirement) and the income stream is discounted at the average real growth rate in AWE (0.8% p.a.).
Table 14: Deaths from dementia, Australia, by age and gender, 2002
Total deaths
1,716
3,411
Source: Access Economics, based on Annex Table E from Mathers, Vos and Stevenson (1999).
This yields the net present value (NPV) of the mortality burden as $8.8 million. The NPV of taxation revenue sacrificed for the mortality burden is $2.5 million.
2.2.2
Family and carer costs
As we have seen in Section 1.2, most people with dementia receive care at home initially, with day-to-
day personal needs and support left very much to family and friends. Society, and our public sector health and welfare budget, relies increasingly on the support that such families and carers provide.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
The approach adopted here is one of replacement cost (see
The value of informal
Methodology), where the value of the hours of care is imputed as if a paid care worker provided them. Three tiers of care are
care of people with
modelled, based on the University of Michigan average hours of
dementia was over
care for people with mild, moderate and severe dementia (see
$1.7 billion in 2002.
Section 1.5.1). The imputed carer rate is $19.25 per hour, based on the Community and Aged Care Services (ACT) Award, 2002
(AW817098) for a Care Worker Grade 3, with adjustment for leave loading and after hours. Most of those with mild dementia (23% of total prevalence), about half of those with moderate dementia (22% of
the total), and one quarter of those with severe dementia (7.5% of the total) are assumed to live at home, noting that many are in nursing homes for reasons other than dementia. The results are in
Table 15, with the total value of families and carers for people with dementia estimated as $1.71 billion in 2002. Associated tax foregone equates to $489.7m.
"I have been looking after Marjorie for 16 years but she has only required more personal care with
things like eating, showering and toileting for the past five or six years. Until two years ago I used to spend three days a week in the office, but this is now one day only. Everyone said that I should retain
an interest in my work as it would be a respite for me, and I certainly agree with that."
Table 15: Value of families and carers of people with dementia, 2002
No. of people
Hours per
with dementia week of care
Moderate 35,705 25.0
Total 84,394
Source: Access Economics estimates. Part of the value of informal care is compensated through Federal
Family carers provide
Government Programs, notably Carer Allowance ($42.65 weekly in
80% of the value of
September 2002) and means-tested Carer Payment ($214.70 weekly for singles). The means test (income and assets) is
informal care without
modelled to exclude the top 30%, and there is an allowance of
25% "wastage" (people who do not claim the payment for a variety
of reasons). The value of the ‘transfer payments', designed so that the burden of informal care is not borne wholly by the families and carers themselves, is thus estimated
in Table 16 below as $324m or 19% of the total burden.
Table 16: Value of Carer Payment and Carer Allowance for people with dementia, 2002
No. of people with dementia at home
After means test and
transfer
Before means wastage ie, receiving payments, $m
Source: Access Economics estimates.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
2.2.3
Cost of welfare payments
Many people living with dementia are reliant on welfare benefits as their main source of income.
However, in most cases, this is the means-tested Age Pension, paid to eligible men over 65 and eligible women aged over 60-65, depending on their birth date (by 2014 the age will be 65 for everyone). Since
the Age Pension would be paid to eligible elderly regardless of dementia, it is not included in modelling here.
People under retirement age with dementia may be eligible for the Disability Support Pension (DSP) and
in some cases, Sickness Allowance. The DSP is the main means of income support in Australia for people aged 16 years and over whose physical, intellectual or psychiatric impairment prevents them
from working, or for people who are permanently blind. There were some cutbacks to the program in the May 2002 Budget. Sickness Allowance provides assistance for people who are employed and who are
temporarily unable to work (or study) due to a medical condition. It is not significant in the case of dementia so is not modelled here.
There are also entitlements to concession cards – Pensioner Concession Card (PCC) & Health Care
Card (HCC), which may result in concessional transfers such as prescription medicines, transport fares, rates, power bills and car registration – and to Rent Assistance, for people who get a payment such as
the Carer Payment and pay rent for private accommodation. Although insufficient data precludes a firm estimate of many of these transfer payments (and they are likely to be relatively small as a proportion of the real total indirect costs anyway), a conservative
estimate of welfare payments which includes the main items – DSP, Rent Assistance and Pharmaceutical Allowance – is provided in Table 17 below, totalling $52.0m of which $47.7m is DSP.
Table 17: Cost of welfare payments
weekly receiving total cost
$ 196.95 4,653 47.7
Rent Allowance (weighted)
$ 48.83 1,396 3.6
Pharmaceutical Allowance
$ 2.90 4,653 0.7
Source: Access Economics estimates utilising Centrelink rates of 20-Sept 2002.
2.2.4
Modifications and aids
People with dementia and their families and carers may require a variety of additional equipment, aids
and home modifications in order to continue living at home safely. These include memory aids (such as large-face clocks, signs and identifiers), bathing and toileting aids (eg, shower accessories, incontinence
pads), safety aids (such as gas detectors, wandering/occupancy alarms), adapted cutlery and common items (eg, clothing with Velcro), daily pill boxes, mobility/transport aids (eg, walking frames, special
shoes for "walkers"), nursing aids (eg, pressure-relief mattresses), grab rails, and so on. There are a number of public programs for older people, people with a disability and their families and carers to assist them to make home modifications and provide aids and equipment that will help them to
remain living in their own home avoid having to go into a residential care facility. The Home Maintenance and Modification Program is funded by the Commonwealth and State Governments under
the HACC program, with two levels of assistance. The lower level of assistance is the Home Modification and Maintenance Services program, which includes installation of rails, provision of secure
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
rugs, hand showers, grab rails, moveable ramps and taps, as well as with minor home maintenance and
repairs. Assistance with major work over $5,000 is through the Home Maintenance Scheme, with the cost up to 20% of the total cost of the job.
The Program of Appliances for Disabled People (PADP) provides equipment and appliances to disabled
people and some others, who are financially disadvantaged, including adjustable beds, hoists and mechanical lifters, shower chairs and bath seats. Access to continence aids – such as pads, uridomes,
kylie sheets, commode chairs and toilet seats – is variable by State/Territory, with a summary of national, State and Territory programs provided in Continence Foundation of Australia (2000).
The Independent Living Centre is a non-profit organisation that provides information about equipment,
building design and other resources, as well as a display centre for people to view and sample a wide range of products and equipment, including aids for communication, lifting and transfers, continence,
leisure and recreation, mobility, seating and transport. Whether paid for privately or publicly, all these items incur additional indirect financial costs. Frisch (2001, Table 1, p18) undertook detailed survey work of the costs of aids, equipment and modifications in
Australia, as shown in Table 18, averaging $738.40 per person. Across all those people with dementia, the total cost in 2002 was $119.8m.
Table 18: Costs of aids, equipment and modifications, 2002
Mean cost pa
Annual cost
per person ($)
all dementia ($m)
Housing modifications
Aids and appliances
Consumables $299.00
Source: Access Economics based on Physical Disability Council of DC Australia (Frisch, 2001) data.
2.2.5
Summary of financial costs
Table 19 and Chart 12 show the real indirect financial costs of
The total financial cost of
dementia as $2.2 billion, around two thirds of the direct health
dementia in 2002 was
and ageing costs. Total real financial costs (direct and indirect)
were $5.6 billion. Interestingly, this is roughly equivalent to total
$6.6 billion – over
Federal Government outlays for aged care services
$40,000pa per person
administered by the Department of Health and Ageing,
estimated to be $5.5 billion for 2002-2003 (about 0.77% of
GDP).77 In addition, there were $968 million of transfer payments – both lost revenue (tax foregone for people with dementia and their families and
carers) and expenditure (welfare and carer payments). In total, indirect
dementia's financial
costs were $3.17 billion (roughly equivalent to direct health and ageing
costs). The total financial costs of dementia (direct and indirect,
impact will total
including additional net transfer payments) were $6.58 billion in 2002.
77 As quoted in DHA (2002a) Attachment C.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
In per capita terms, the indirect financial costs of ageing are approaching $20,000 per person with
dementia p.a., while the direct health and ageing costs of dementia are over $20,000 per person p.a., including home and community care of just over $1,000 per person with dementia in 2002 (but $2,554
per person receiving the care). Relative to national income, total financial costs are already approaching 1% of GDP and are set to reach 3.3% of GDP by mid-century78. Direct costs alone will reach 1.6% of
GDP.
Table 19: Summary of direct and indirect financial costs of dementia, 2002
$ million
Transfer
Real cost payments
dementia
Direct health costs
Including residential care
Home and community care
Indirect financial costs
Lost earnings (patients)
Mortality burden
Tax foregone (patients)
Tax foregone (carers)
Welfare payments
Aids & modifications
Subtotal indirect financial costs
Total financial costs
*The averages per person with dementia in residential care and per person with dementia at home receiving formal services are $36,547 and $2,554 respectively (see Table 12). Source: Access Economics.
Chart 12: Distribution of the financial costs of dementia, 2002
Carer costs
Transfers:
Other health system
Transfers:
Home-based aged
Lost earnings &
patient/carer tax
Source: Access Economics.
2.3 THE BURDEN OF DISEASE
In 2002, over 5,000 Australians died from dementia (Table 14 Section 2.2.1), while thousands of others
suffered from its disabling and distressing symptoms and its pervasive impacts on loved ones. Dementia 78 Assuming ultra-conservatively only demographic growth and no increase in the real cost of care per person.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
imposes burdens on people and their families and carers that go well beyond the financial costs. There
is no objective way to ascertain a financial value for the pain, suffering and premature death from illnesses like dementia for all those involved. However, the internationally developed ‘Burden of
Disease' methodology (see Methodology) has earned recognition in Australia and overseas as a useful way of estimating the years of healthy life lost due to a condition. This method uses DALYs—or
‘disability adjusted life years'—as the measuring stick. DALYs have two components:
□ the years of life lost (YLL) due to premature death—the mortality burden; and □ the years of healthy life lost due to disability (YLD)—the morbidity burden.
DALYs, YLLs and YLDs provide indicators that are useful in measuring the impact of disease and exploring the effectiveness of health Dementia cost over
spending in terms of purchasing years of healthy life. The Australian
117,000 years of
Institute of Health and Welfare has provided some excellent analysis in
healthy life for
this area. Mathers, Vos and Stevenson (1999) estimate the burden of disease in 1996 for a variety of disease and injury categories. Table 20
Australians in 2002.
extrapolates their estimates for dementia to 2002 using prevalence and demographic data.
Table 20: Burden of disease from dementia, 2002
DALYs YLL YLD
Males 44,039
Females 73,043
Total 117,083
Source: Access Economics, utilising data from Mathers, Vos and Stevenson (1999). In Australia in 2002, the burden of disease attributable to dementia was estimated as 117,083 DALYs.
Morbidity was the major source of burden (85,651 YLDs were 73% of the total) while mortality accounted for 31,432 YLLs or 27%. Females bore 62% of the overall burden of disease and the same
proportion was borne by people aged over 75. It is noteworthy that the disability weights for dementia are 0.27 for mild cases, 0.63 for moderate cases, and 0.94 for severe dementia. The latter is the highest
disability weight for all illnesses, equal with severe rheumatoid arthritis and higher than that of final stage terminal cancer (0.93). This shows the extent of the disability burden for dementia compared with
other illnesses. The next section provides further comparison with other diseases.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3. COMPARISONS, CONSTRAINTS AND SCENARIOS
3.1 COMPARISONS WITH OTHER DISEASES
Dementia is one of the leading causes of health system costs and disease burden in Australia. National
Health Priority areas, which account for over 70% of the total burden of disease (DALYs), are currently:
□ Cardiovascular disease □ Cancers
Dementia is more
□ Mental health
□ Injury □ Diabetes
epilepsy or skin
□ Arthritis and musculoskeletal disease
While dementia falls within the Mental Health priority area, the main policy focus within mental health so
far has been on depression. This section compares the prevalence, health costs and disease burden of dementia with other illnesses, including the National Health Priority areas.
3.1.1
Comparisons of prevalence
Chart 13 compares the prevalence of selected disorders in Australia according to the latest data from
the National Health Survey, released in October 2002 and relating to the year 2001. National health priority areas are asterisked. Musculoskeletal disease, of which arthritis is the largest component,
dominates the profile, followed by circulatory disease. Asthma is also very common, affecting over 2m Australians, while 1.8m have mental disorders and around 1.4m suffer injuries (including poisoning).
Diabetes affects over half a million Australians. The prevalence of dementia is of the same order of magnitude as partial and complete blindness, and cancers (excluding skin cancer, the most common
form) and slightly less than dermatitis and eczema combined. Dementia is more common than epilepsy or skin cancer, and the NHS data also indicate higher prevalence than alcohol and drug abuse.
Dementia is more common than any other neuro-degenerative condition, including Multiple Sclerosis.
Chart 13: Prevalence of selected conditions, 2001
All musculoskeletal disease *
All circulatory disease *
Arthritis *
All mental disorders *
All injuries and poisoning *#
Diabetes *
Dermatitis and eczema
Other cancer *
Alcohol and drug abuse
Skin cancer *
Number of persons ('000) reporting condition
Source: Access Economics based on ABS (2002) 2001 National Health Survey data. # estimated from ABS (1997) 1995 NHS data. * = National health priority areas.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3.1.2
Comparison of financial costs
Table 21 compares the direct health system costs of dementia with those of other disorders, including
the national health priority areas, according to Mathers and Penm (1999)79. Circulatory disease was the most costly, as a result of its impact on the hospital system. Digestive diseases (largely dental
problems, ulcers and hernias) are second highest because of their dental costs. Musculoskeletal disease is third, due mainly to the various impacts of arthritis and osteoporosis across the health
system. Injuries (including self-inflicted injury) also have high hospital costs, just tipping them above mental illnesses in the year of comparison. Mental illness is next, representing over 8% of total health
costs. Dementia is the most costly component of mental health, as noted in Table 9 (Section 2.1.1). Of all expenditure on health, dementia was already 2.3% by 1993-94, 20% of nursing home costs. As
noted in Section 2.1.1, the nursing home costs of dementia were likely underestimated by half in 1993-94, putting the probable contribution of dementia closer to $1.4 to $1.5 billion.
Table 21: Comparison of direct costs, 1993-94
Disease category (ICD-9
allied Nursing
chapter)
Costs Hospitals Medical ceuticals
health homes
Musculoskeletal*
of which dementia
Respiratory (inc. asthma*)
Complications of pregnancy
Endocrine (inc. diabetes*)
Dementia as % of total
2.3%
0.1%
Source: Mathers and Penm (1999), Table 1, p2 and special AIHW data request for dementia.
However, it is noteworthy that circulatory and digestive disorders, as well
as cancer, injuries, diabetes and asthma, are likely to have smaller indirect
costs since the requirement for ongoing carers is not so high. With cancer
every $40 in the
and circulatory disease, this is unfortunately because of their high fatality
Australian health
rate, while in the others it is because treatment and management enable
lower levels of disability and care or, in the case of injuries, a higher rate of
recovery. Because of the substantial carer costs for dementia, it is likely to
rank extremely highly in indirect costs, although insufficient comparable
data are available to draw sound conclusions. Musculoskeletal disease would probably rank highest due to both high prevalence and high disability burden.
79 Although this data relates to the year 1993-94, it is the most recent available. Updated cost data are expected from the
AIHW in June 2003.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3.1.3
Comparison of disease burden
It is in terms of the burden of disease from disability that dementia is most
costly. More years of life are lost due to disability (YLD) from dementia (5.6% of
the total) than from every other national health priority area, second only to
depression (8.0%), as shown in Chart 14. Asthma ranks third (4.8%), followed
closely by osteoarthritis (also 4.8%), hearing loss (4.1%) and diabetes (3.8%).
Cardiovascular disorders (such as stroke and ischaemic heart disease) also
rank in the top ten. Dementia is the second highest disability burden for women
and the fourth highest for men (Mathers, Vos and Stevenson, 1999, p51, T4.3).
health priority.
Chart 14: Ten leading causes of years of life lost due to disability (YLD), 1996
Hearing loss
Ischaemic heart disease
Generalised anxiety disorder
Age-related vision disorders
YLD as a % of total YLD
Source: Mathers, Vos and Stevenson (1999), Figure 2, pxxv.
In terms of total DALYs, including the YLL or mortality burden,
dementia ranks fourth highest for women and tenth for men, of all
Dementia carries the
disorders. For older Australians, these rankings rise to third (8.9% of
greatest burden of
the total disease burden) and fifth respectively (5.3%). Table 22 shows the contribution of dementia to the total burden of disease for
disease for older
older Australians. The only greater threats to older Australians are
Australians, unrelated
smoking-related – ischaemic heart disease, stroke, lung cancer and
chronic obstructive pulmonary disease (the latter two for men only).
Table 22: Contribution to the total burden of disease for older Australians
1 Ischaemic heart disease
1 Ischaemic heart disease
3 Dementia
8.9
5 Dementia
5.3
6 Prostate cancer
6 Colorectal cancer
7 Colorectal cancer
8 Diabetes mellitus
8 Age-related vision disorders
9 Adult-onset hearing loss
9 Diabetes mellitus
10 Benign prostatic hypertrophy
10 Osteoarthritis
Source: Mathers, Vos and Stevenson (1999), Table 5.9 p73.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3.2 CONSTRAINTS TO SERVICE DELIVERY
This section identifies constraints to current service delivery and to extending service provision to meet
projected need, including medical and hospital services, pharmaceuticals, research, residential care, home and community programs, and demand/distributional issues in the health financing system. A
solution-focused approach is adopted, which is developed further in the following chapter on strategies.
3.2.1
Medical and hospital services
Early detection: As noted in previous sections, although GPs are often the first contact for people with
dementia and their families and carers, they are often not equipped to carry out the more
comprehensive psychometric screening nor have the skills to diagnose the early stages of dementia or complex and unusual dementias. Interventions are required to assist GPs (and others) in detecting
dementia. Extension of specialist services for early detection of dementia, for example through memory clinics, is important.
The General Practitioner Assessment of Cognition (GPCOG), a recent screening tool, has been
recommended by Professor Henry Brodaty as valid, reliable, quick to administer (less than 4 minutes for
most), easy to use and acceptable to GPs and their patients, representing an advance over former screening tests – performing as well as the Abbreviated Mental Test and at least as well as the MMSE.
Many GPs require more information about how to administer the GPCOG and differential diagnosis of cognitive impairment, although MMSE should also continue to be encouraged.
Using PET scans in the early stage diagnostic process for AD has been found to reduce the false-
positive rate by half and the false-negative rate by 60%. This new analysis, presented by University of California (Los Angeles) researcher Dr Silverman at the American Academy of Molecular Imaging in
October 2002, suggested that patients could be kept out of nursing homes for 9 to 18 months longer through such early diagnosis and the use of early treatment of AD with cholinesterase inhibitors. He also
found that early diagnosis and treatment could substantially reduce medical and hospital costs. Expanded use of PET scans may not be possible in Australia in the near future however.
Supplementary education of GPs and primary care workers is also required to assist them in caring
for patients subsequent to screening. This should include dementia management principles with the
goal of recognising highly trained GPs as ‘dementia-accredited GPs'. This is in keeping with the de-
institutionalisation of mental health care over the past two decades, the burden of which has fallen largely to GPs. Increased remuneration is indicated for the higher skills levels required for such
accreditation, perhaps in the style of current Enhanced Primary Care (EPC) Medicare items. There are also constraints to GPs attending patients in nursing homes, in part due to the remuneration structure.
New information technology initiatives such as teleconferencing may provide support for GPs who are more isolated. Information technology may also be of use in GP education and referencing programs.
Acute care hospitals: Acute hospital costs could be reduced by reducing the time (four times the
ALOS) that dementia patients are hospitalised awaiting transfer to a high care facility. Such transfers comprise nearly two thirds of entries to high care. Ongoing monitoring is required to assess potential
mechanisms for reducing these wait times, and the cost-effectiveness, appropriateness and equity considerations of such interventions. Access to dementia-trained nursing staff should be available also
in acute care hospitals for the period of the ‘wait'. Acute care providers report that they need more training, resources (including geriatricians) and strategies to manage people with dementia (secure
environments, appropriate assessment tools, care and discharge planning). These issues are being addressed in some States through "Innovative Places" and similar models.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3.2.2
Early access to medications at an affordable price is another constraint for people with dementia and
their families and carers. Access is currently constrained by:
□ an overly rigid definition of 'acceptable benefit' (which excludes maintenance of existing cognitive
function in a progressive condition, and also excludes improved social functioning, which reduces
carer burden and delays institutionalisation);
□ the exclusion of people with non-AD forms of dementia; and □ administrative arrangements that can result in unintended and adverse outcomes.
Disadvantaged groups include people with non-Alzheimer dementia and all people with dementia who need anti-psychotic treatments.
PBS ‘cost-cutting'
measures could be
Moreover, such cost-cutting measures – targeting pharmaceutical
expenditures – have been found in numerous studies to be ineffective in
increasing overall
reducing overall health costs. Rather, they have been found to increase
health care costs
overall health costs by 30-50%. Horn (2002) summarises current
research, which has shown that:
□ limiting doctors' prescribing choices was found to be associated
with increased overall utilisation of pharmaceuticals;
□ there are significant associations between formulary restrictions in a drug class and higher health
care utilisation (GP or emergency department visits, additional prescriptions, hospitalisations);
□ the negative effects of formulary restrictions lead to particularly suboptimal therapy and outcomes
for older people;
□ patients with pharmaceutical capitation had 14% higher total
"Rising drug costs
health costs than non-capitated patients and 29% higher
pharmaceutical costs (although this is not currently important for
are, in general, part
the Australian system);
of the solution, not
□ newer drugs are often those targeted for cost-control because
part of the problem."
they can be most expensive; yet these can offer the best
outcomes as they are likely to have fewer side effects, improved safety and efficacy, greater ease in use, increased compliance
and be better tailored to individual needs;
□ best practice drug use can result in lower carer absenteeism, lower employee turnover and greater
labour productivity;
□ if the only options are to control or not control drug access, then not controlling is the better choice.
There is a third option, however – discovering, through clinical practice improvement (CPI) studies what
the best treatments for specific types of patients are, and implementing them as guidelines. CPIs can uncover important, sometimes surprising and cost-saving results. Kleinke (2000) concludes that the best
strategy for preventing over-use and inappropriate use of pharmaceuticals is to tie utilisation of drugs to best practice research and established clinical guidelines.
One example is the treatment of agitation in dementia. Cost-cutting regulation has aimed at
discouraging the use of psychiatric medications in the treatment of dementia in nursing homes and the limitation of pharmacotherapy to monotherapy. However, CPI studies have shown that this intervention
has in fact increased overall costs relative to combination therapy.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Another example studied limiting both access to psychiatric drugs and visits to mental health providers. This was associated with higher total health care costs. In contrast, unlimited and early access to best
practice mental health care for another firm (Merrill Lynch) was shown to reduce costs per employee by 25%.
Dr Horn provides other examples for treatment of depression, asthma, arthritis, ulcers, hypertension and
antibiotics. She concludes that drug costs are not a cost item to be managed, but a health maintenance item to be leveraged.
"Curtailing access to medications via cost-control mechanisms can adversely affect other health costs
and increase total health care utilisation".
Section 2.1.1 on direct costs showed that, projecting official AIHW estimates of public research on
dementia in 1993-94 of $8.4m, Australia in 2002 spent around $19.2 million on such research. This equates to $118 per person with dementia per annum, or $1 on research for each $342 of the total
costs of dementia (0.29%). However, Jorm et al (2001) and Maller and Rees (2002) note that this growth (the ‘normal' for the sector) has not occurred for dementia and that in fact, official money spent
on dementia research may be as little as $2.5m in 200080 – less than 1% of all NHMRC research expenditure ($15.40 per person with dementia and $1 for every $2,630 that dementia costs).
Alzheimer's Australia generates from trust funds a mere $40,000 annually to extend towards research grants, compared with US$120m (A$240m) that the US Alzheimer's Association has granted since 1982
– over 25 times the annual per capita level in Australia.81 Other international comparisons (summarised in Table 23), while not directly comparable, suggest that:
□ Spending on AD research in the United States is A$300 per person (A$1.2billion in total), with calls
from stakeholders to increase it to US$1bn (A$2bn or A$500 per person).
□ In the UK, research funding on AD is trivial – 60% of the amount spent on stroke, less than 10% of
the amount spent on heart disease and only 3% of the amount spent on cancer (Lowin et al, 2000).
□ In Canada, the 1991 data are similar to the AIHW data for Australia in 1993-94, around 0.25% of the
cost of the disease.
Table 23: Comparisons of costs and research allocations, Australia, Canada, US and UK
Comparisons
Australia,
Australia,
UK, Canada (1991,
Jorm, 2000
People with dementia
Total costs ($Am)
Cost per person ($A)
Research costs ($Am)
Research (A$/person)
Total costs: research costs
Source: Access Economics using exchange rates of A$1=$US0.50 = C$0.8989 = UK£0.3484.
80 A search on keywords ‘dementia' and ‘Alzh' showed $5.36m in NHMRC grants for 2002 and $42.4m for 1995-2002. 81 A$240m / 14 (population factor) / 20 (years) / 30,000 ($A in Australia) = 28.6 times larger
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
In Australia, if we took the current US level as a comparator ($300 per person), we should be spending
$49m per annum on officially funded dementia research; if we used the US goal as a comparator, we should be spending $81m p.a. As middle ground, if we aimed to make research 1% of the total costs of
dementia each year, we should be spending $66m p.a. Australia, as a ‘knowledge nation', has comparative advantages in innovative research and development, and should be pulling our weight internationally in this critical area. Large pharmaceutical
companies are already spending substantial resources on medications and vaccine research. However, there is a critical gap both in Australia and overseas for research into better clinical practice and care, in
a country whose aged system is in many ways world class. Less than 10% of our research on dementia involves the investigation of services, and this knowledge is less importable because there is so much
that is unique to the Australian situation (Jorm, 2001). In the area of dementia services, research should focus on:
□ the key factors that make staying at home more or less likely - including understanding better the
role of psychosocial approaches to keeping people with dementia at home;
□ the importance of new technology in the design and modification of homes; □ the importance of autonomy in user satisfaction with long-term care and the role of the consumer as
□ the evidence available for achieving better co-ordination of services - in the community and at
discharge from hospital in particular;
□ the meaning of ‘domestic'/ ‘homely' in the context of residential care; □ the advantages and disadvantages of early diagnosis for a consumer and the role of memory
□ the profile of the minority who will need dementia specific care.
In sum, Australia has fallen behind substantially in dementia research. Greater investment in research is imperative in meeting the challenges presented by the dementia epidemic, with priority accorded to
research on care practices and the delivery of services as well as bio-medical and medical research. "Given the magnitude of potential savings – including savings to public health care programs – if Alzheimer's disease could be prevented or arrested at an early age, a substantially increased federal
commitment to Alzheimer's disease research is clearly warranted… There are few signs that public or private research is being undertaken at a scale warranted by the magnitude of the disease's costs."
Hay and Ernst, quoted in Lowin, McCrone and Knapp (2000)
3.2.4
Home and community care
Constraints arise in community care in two areas - in-home support services and support for families
and carers. For in-home support services, the barriers are primarily financial. Many people cannot
adequately access home-based maintenance and support through HACC and more intensive support, such as CACPs. Recent increased HACC budget allocations in FY2002-03, while welcome, have fallen
short of addressing unmet need. Additional funding would ease these constraints. Steps also need to be taken to ensure that all HACC, CACP and EACH services are capable of supporting people living in the
community with dementia. As with the residential sector, this will require additional training for staff, beyond its current respite worker focus, to ensure that all staff in services that have contact with older
people are in a position to understand the needs of people with dementia and how those needs impact on service delivery. While staff training is normally an employer responsibility the structure of the
community services sector makes it very difficult for organisations to meet the costs of additional

The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
training. Accordingly Government support for the cost of this training should be provided. The existing
CEWT program is a cost-effective model that could be expanded to meet this need.
In terms of family and carer support, the issues are
not just financial – innovative models are required.
The 2002-03 Federal Budget included an extra $80 million to help families and carers over the next four
years, with $30 million to expand the number of respite services, assist with the cost of equipment and
transport and provide emotional and psychological support for families and carers.82 A further $20 million
is to help families and carers of people with dementia to obtain residential respite and increase access to
specialist psychogeriatric advice and support. An
additional $30 million will support ageing families and carers of people with disabilities by providing
education and training for volunteer carers, targeted care packages and assistance with purchasing care services and equipment. A Commonwealth Carer Resource Centre in each capital city acts as a
single contact point for carers seeking information and advice about the full range of services available to them. The Government is also funding the development and distribution of some carer resource
materials.
While these measures provide a good basis there remain large gaps in the following three key areas.
1. Respite
Funding for the National Respite for Carers Program has
Respite is an essential part
increased from $19 million in 1996-97 to an estimated $88
of dementia care. It must be
million in 2002-03. This represents a good start, however,
tailored, timely, linked with
much existing respite care is not appropriate for carers of
people with dementia, who require regular respite care that
other types of support and
is responsive to key changes in their situation, with the
provided by knowledgeable,
capacity to also support them in emergencies. Respite care
skilled and flexible helpers.
for younger people with dementia can be particularly
inappropriate. The quantity of residential respite care available is capped at 63 days maximum in a financial year (one day in six, with an additional 21 days in special circumstances). More in line with other work weeks
would be two days in seven (including nights) – 104 days per FY – plus annual holidays. However, the existing places are in fact under-utilised (64% of available allocated respite days in residential facilities
are used), with the 2002 Budget including funding to increase the take-up rate of residential respite. As a consequence the Commonwealth is utilising such funds increasingly through brokerage.
Funding for the Early Stage Dementia Support and Respite program (currently being evaluated) needs
to be extended, or new funding provided for a new program for support and respite for people with mid-stage dementia. Additional funding for support is likely to be particularly cost-effective in reducing carer
burden and delaying institutionalisation (see Section 3.3.2). 82 Carers Australia (2001) identified transport and equipment costs as one of a number of priority areas for the 2002-03 Budget. Regarding emotional support for carers, Carers Australia seeks to develop ongoing partnerships for a range of
counselling models (including personal and relationship counsel ing, family conferencing and telegroup counselling services)
for carers and their families, including subsidising carers who are unable to meet the user charges for counselling services.

The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Moreover, more flexible models of respite care are needed, including overnight and weekend support, cottage style accommodation, extended hours at day centres and extension to many areas where there
are access problems and service gaps.
2. Carer education
"Most carers do not have access to appropriate education programs to assist them in their caring role… In a recent national health and wellbeing survey, 33% of respondents reported physical injuries as a
result of providing care, but 49% of respondents had never received information or practical training."
Carers Australia (2001)
There remains a lack of access for family carers to informal, practical, age-appropriate and culturally
sensitive instruction and advice tailored to their immediate and continuing needs. This need must be met with the assistance of people with first hand experience
of dementia care. Additional funding is required, ideally channelled through Carer's Associations and Alzheimer's
□ subsidise respite care and other participation costs for
family carers who need financial assistance to take advantage of the education program;
□ expand national Alzheimer's Australia programs to
enhance support groups, counselling, training and ‘living
with memory loss' programs;
Above: Donald, 29, assists his
grandmother, Mary, with all of
□ expand dementia specific and quality person-centred
care programs to respite service providers and residential
her basic needs
care staff.
The pioneering work of the late Professor Tom Kitwood of the Bradford Dementia Group has contributed
significantly to quality of care outcomes for dementia care, including carer training programs based on his person-centred principles (Kitwood, 1997). The University of Bradford (2001) has instigated the first
UK undergraduate degree in Dementia Studies based on his work, including distance learning and key techniques such as Dementia Care Mapping, devised by Kitwood as a way of consulting with people
with dementia who may not find it easy to comment through questionnaires or focus groups.
Dementia Care Mapping is a method of evaluating and improving the care given to people with
dementia in home-based, respite and institutional settings. 'Mappers' make detailed observations of
people with dementia in a particular setting, recording what they see on a grid. Observations are carried out over a prolonged period of 6 - 8 hours covering the full waking day of residents. The resulting data
offers a 'map' which shows in summary how each resident fared - what they did throughout the day, what they enjoyed and what caused them distress. It shows how care is distributed among the group,
notable characteristics of the style of care as well as an overall index of the general quality of the service. It can highlight individual needs of residents that have perhaps gone unrecognised as well as
'high spots' in a person's day that indicate particularly good practice. Ongoing training with staff on site by the Dementia Team can enhance the good practice and help make necessary improvements.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3. Workforce opportunities to assist families and carers in being able to maximise employment
Currently there are few initiatives that target employers of family carers. The goal would be to enable
them to develop strategies for more flexible work practices in order to retain participation rates of trained workers. As the demographic transition continues, participation rates – particularly of women – will
become increasingly important in maintaining economic growth as well as sustainable public sector revenues from taxation. These factors were noted in the Federal Government's InterGenerational
Report, launched with the May 2002 Budget. Possibilities might include part-time home-based work, work-based adult day-centres, or access to work-based services for family carers such as counselling or exercise programs. In addition, dementia
awareness and destigmatisation courses could be introduced in workplaces. A few pilot trials of such initiatives should be implemented, based on international pilots.
3.2.5
Residential care
After an ACAT has made a recommendation for transition of a person with dementia to appropriate
residential care, it will often provide a list of local facilities, although in many areas in Australia the ‘good ones' are likely to have waiting lists exceeding a year. Even if a place becomes available, it may not suit
the individual (eg, same gender preferences for shared rooms in some low-care facilities). Moreover, the accommodation provider may be seeking a person without challenging behaviours, yet the reason for
seeking care may have been that the family carer is unable to cope with a demanding phase of BPSD. Often decisions are made under pressure, and the family carer takes whatever becomes available,
which can result in deep dissatisfaction, particularly if promised services (such as specific therapies) are not forthcoming or if the quality of care is not up to expectations.
Nursing and personal care staff are not well remunerated. There has been exposure in recent years of a
number of cases where residents have been inappropriately drugged, restrained or neglected. Rosewarne et al (2000) found that half of all high care facilities reported regular use of ‘chemical'
restraint and one third reported regular use of ‘physical' restraint. Across all facilities, chemical and physical restraint were used rarely or never in 48% of facilities, sometimes in 36%, and often or
regularly in 16%. Facilities that had a ‘no restraint' policy found that if restraint was not an option, staff tried much harder to find other more appropriate solutions. The Australian government has recently
funded a national project to provide education and training materials for aged care staff regarding the appropriate use of restraints.
Existing dementia-specific care
With the number of high care beds strictly controlled since ACATs were established, although waiting
lists83 for nursing homes are reduced, the impairment of those admitted and consequent nursing requirements have increased. Although a large and growing proportion of high care residents have
dementia, the design, staffing and management of nursing home services have been geared more to physical disabilities with limited scope to manage the particular BPSD needs of dementia residents.84
This has led to greater demand for dementia-specific care facilities, although policy remains to
83 Entry period (the days between ACAT assessment and entry into residential care) has increased however, and is a poor
proxy for waiting time. For more detail, see AIHW (2002c). 84 One example is the ability to manage late afternoon restlessness common among people with dementia, often termed ‘sundowning'. The reason for this behaviour is thought to be past history of busy-ness with children and meals, and many
dementia residents still feel an unclear call to action, leading to agitation and often wandering. Specific therapies and skills
are required to caringly manage these behaviours, as well as fairly high staff-to-resident ratios.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
accommodate mobile people with dementia in low care facilities, reflected in the allocation of a large
proportion of the low care places in recent Aged Care Approval Rounds to people with dementia, even though their ACAT assessment may be ‘high care'. ACAT assessments do not reflect the optimal type of
environment for the person, and therefore the type of accommodation payment that is most appropriate. For low care facilities, 85% of residents with dementia are supported
in mainstream areas (15% in dementia-specific areas); for high care
facilities, the comparable figure is 92% (and 8%). Hostels have, since
specific places are
the termination of Dementia Grants85, struck funding problems, mainly
needed, particularly
because recurrent costs are higher due to the special requirements of
for those who are
dementia care, yet residents must be assessed as ‘low-care' (which
often they are not) in order to gain a place. Conversely, there are
ambulant and have
disincentives to invest in high care facilities because it is so difficult
for providers to cover the capital costs (without accommodation
bonds), and this may not be appropriate for mobile people anyway
who need personal rather than nursing care. There is the option of becoming an ESP, although these places are too limited to be able to adequately cross-subsidise, which
in any case is sub-optimal and potentially inequitable.
Recurrent costs constrain
As noted earlier (Section 1.2.9), over 90% of people in high
‘low care' dementia places.
care and 54% of people in low care facilities have dementia
Capital costs constrain ‘high
or cognitive impairment, yet only 6% of residential care beds are dementia-specific. The capacity for residential care to care' dementia places, even
support people with dementia (both facilities and workforce
when these are appropriate.
training) is a serious constraint. There are too few places
specifically designed to support people with dementia with challenging behaviours or other special needs, and inadequate training for staff caring for these people.
It is estimated that at any time 10% of residents with dementia will require special support. A final issue is care for people with severe (physically aggressive or violent) BPSD. These 1% of people with dementia who need mental health and aged care services may be unable to access either state
mental health of Commonwealth funded aged care. This represents a significant gap in the care system. Finding care for the person with dementia can be extremely challenging. It is widely acknowledged that there is a nationwide shortage of dementia-specific residential accommodation. Such homes require a
higher staff-to-resident ratio and a higher level of security, and they need to offer appropriate therapies and facilities, such as safe walking areas for residents. Ideally they are smaller, with only 10-15
residents – a comfortable number of new faces for the person with dementia to deal with.
Hampson (2000), p227.
Summary of issues for existing residential facilities
□ increased ongoing training for all care staff in dementia-specific and quality person-centred care
□ staff-to-resident ratios that address understaffing, with guidelines on the appropriate mix of nursing
and personal care staff;
□ tighter accreditation and monitoring of standards to actively ensure quality care, with restrictions
placed on chemical and physical restraint practices;
85 Dementia Grants Program funding was made available to all low care facilities for a period of eight years from the mid-
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ review of remuneration for nursing and personal care staff; □ planning ratios need to make provision for dementia care and challenging BPSD; □ descriptors in the RCS should concord with ACAT assessments; ‘high care' should include the need
for behaviour management and environment, not just the need for nursing care;
□ potential perverse incentives in the RCS relating to behaviour need to be addressed with increased
rating/funding also attached to interventions which will prevent challenging behaviours rather than rating/funding solely favouring managing challenging behaviours;
□ overall numbers of places and sustainable funding mechanisms (see Section 3.2.6 below); and □ greater access to care for people with severely aggressive behaviours.
New models of residential care
Suppose we were starting from scratch and knew what we know today. To promote ageing-in-place, we would want to have integrated facilities that could cater for a range of different needs as a person ages,
rather than having to move them to a new location. We would want to be able to cater for the specific needs of the large proportion of residents who have dementia or cognitive impairment, or could develop
these in later years. We would want to have staff who were trained in dementia-specific and quality aged care principles, as well as facilities that were appropriate for the various stages of ageing as well
as the mild, moderate and severe stages of dementia – including secure walking areas, a few segregated areas for people with highly challenging behaviours, low care areas for mobile people and
high care nursing areas for those less mobile.
Rosewarne et al (2000) proposes the ‘Cluster house campus model' – separate buildings (‘houses')
each with around 15 beds within a single complex (‘campus') of around 90 beds. The houses would
operate largely as independent care units with a caregiver supported by an on-staff visiting registered
nurse. "The campus could have houses for the more behaviourally disturbed, for those with high physical care needs and for those who require secure wandering areas… The care follows the resident,
ie, residents do not have to be moved to an entirely new location as they become more dependent. The necessity for developing specialised stand-alone dementia facilities is becoming less critical as this
mixed campus approach becomes more widely adopted" (p51). The diagram below illustrates current models of care facilities, compared with a cluster house campus.
Models of residential care
Mainstream units
Co-located units
Stand-alone facilities
H high nursing care
L low nursing care
M ‘mainstream' residents
D residents with dementia
SW secure walking areas
B residents with BPSD
Cluster Housing
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
For care assessment and placement purposes, behaviours might be stratified as B1, B2, B3 and B4,
based on Rosewarne et al (2000) descriptors, with: B1: problem behaviours requiring basic management and occasional intervention; B2: episodic problem behaviours requiring frequent intervention and expert management; B3: continuously disruptive problem behaviours requiring frequent intervention and expert management; B4: continuously disruptive problem behaviours requiring management in specialist psychiatric facilities. There is also broad concordance with the seven tiers of descriptors offered by Brodaty et al (2003), although tiers 6 and 7 (the ‘tip' of the Brodaty triangle) would be captured together within B4:
□ 1 no dementia (M) – 93.4% of older Australians; □ 2 dementia no BPSD (D) – 39% or 63,000 people with dementia; □ 3 mild BPSD (DB1) – 29% or 47,000 people; □ 4 moderate BPSD (DB2) – 21% or 34,000 people; □ 5 severe BPSD (DB3) – 10% or 16,000 people; □ 6 very severe BPSD (DB4) – 0.9% or 15,000 people; and □ 7 extreme BPSD (DB4) – 0.1% or 200 people.
Scenario: Rose is aged 75. Since her husband died five years ago, she has lived with her youngest daughter
(aged 39) who works full time and has three school-age children. Rose's other children live interstate. Two recent
falls have resulted in osteoporotic vertebral fractures, and Rose also has osteoarthritis and mild cognitive
impairment. Her daughter has begun to suffer from stress-related illnesses, and there are tensions with her son-
in-law. Together with other factors, she is assessed by an ACAT as eligible for low care accommodation, and is
offered a place in a new local facility, ‘21st Century Homes'.
Rose takes up residence in Lively Marigold (LM) Cottage and makes some new friends, including a former
neighbour. She continues to drive to go to bridge games with her old friends, and for special events. A few years
later, she is diagnosed as having mild dementia due to Alzheimer's Disease, and six months later a place
becomes available next door in Lazy Daisy Cottage, where she transfers. Together with her family, she decides
to sell her car, although she still enjoys regular shopping excursions utilising the Century bus with her Century
friends. Older friends pick her up for special events. Her youngest daughter and her family continue to visit
regularly. She finds support amongst residents as they talk together about dementia and its impact on their lives.
After her 81st birthday, Rose's wandering develops into agitated walking, she loses many language skills, and her
GP and specialist describe her dementia as ‘moderate' and her behaviours as ‘B1'. She strides for some hours
each day in the beautiful adjacent secure walking area, Serene Way. She also enjoys looking at photos with her
family, and listening to her granddaughter playing the flute. However, she has been gradual y developing some
worsening behaviours that are disturbing other residents of Lazy Daisy. While some of these have been
understood and addressed, others remain, including screaming at night (B3) and verbal aggression requiring
frequent expert intervention (B2), for which family, staff and specialists have been unable to find any solutions.
Rose is provided with the next available place in an adjacent cottage, Little Dainty Bluebell. Her walking can be
accommodated in a less accessible secure area, very similar to Serene Way. However, she becomes incontinent
over the following year and the level of nursing that she requires necessitates a further transfer, at age 84, to a
high care cottage for people with dementia and challenging behaviours, Heavenly Daffodil Bank. The aggressive
behaviour and screaming stage gradually subside, becoming more infrequent and low-key. Then Rose falls and
fractures her hip. After a 5-week hospitalisation, she has lost a lot of her mobility and ceases both walking and the
disturbing behaviours.
Rose is resettled from acute care to Century, this time in Hydrangea Dusk cottage, where she spends her time in
sedate activities including listening to music and massage therapy. At age 86, Rose develops a persistent
infection and a palliative care specialist spends some time with her and her family during her final weeks. She
dies peacefully at home in Hydrangea Dusk cottage with her daughter and granddaughters beside her.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3.2.6
Health financing and cross-cutting access issues
Chart 15: Ageing in Australia: Population
For the 400 years prior to 1920, for which British data are
by age, 1971, 2001, 2041, dependency
available, the proportion of the population over 65
ratios and budget impacts
hovered around 8% of the total (Broe, 2002). From 1920,
rapid population ageing in developed countries has
begun. Australia has already seen significant
demographic change – birth rates are lower, life
expectancy is higher, family size has fallen and more
people live alone. The change in the age structure from
1971 to 2001, together with the ABS projected change to
2041, is shown in the top three panels of Chart 15 at left.
By 2041, people aged 65 and over will represent 25% of
the population compared with 8% 30 years ago and just over 12% currently. The fourth panel of Chart 15 shows
how this cohort of the population is expected to surge as
a percentage of the total, increasing the ‘dependency'
ratio of older people to those of working age.
The implications of the demographic transition for health
and aged care spending are substantial. Medical, hospital
and pharmaceutical expenditures are all substantially
higher per capita for older people than for younger
people. Welfare (disability and carer) payments and aged
care services will also burgeon. Moreover, in addition to
demographic factors, changing technologies and baby
boomer expectations will put sustained pressure on
demand for services – both quantity and quality.
The impact on Federal budget balances, from both
spending growth and a relative contraction of the work-
force tax base, is shown in the final panel of Chart 15.
The InterGenerational Report, released in May 2002,
highlighted these topical issues, concluding that careful
planning will be required to meet the future challenges,
and accompanied by a sharp cut in the PBS budget.
Rather than targeting pharmaceuticals growth, which
Projections from ABS Cat. No. 3222.0.
may well have a negative overall impact on national
wellness as demonstrated in Section 3.2.2 above, more
attention might better be directed at devising savings
Commonwealth Budget Spending Less Revenue (no change)
vehicles for health and ageing. These could include
superannuation-type contributions (1-3% of income)
acting as insurance against future residential or even
home-based care costs, together with public safety nets to ensure equity of access. Other options could include
incentives to extend unsubsidised private health
insurance and review of copayments to ensure that
marginal prices are sending appropriate demand signals.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
The issue of pricing of aged care services is indeed a complex area, with subsidies for residential aged
care currently under federal review. The May 2002 budget included a two-year ($7.2m) review of pricing for RAC subsidies and also took a step in the right direction by delivering the election-promised $50m
indexed annually (totalling $211.1 million over the four-year forward period) into RAC subsidies, as well
as a sizeable package for capital development in rural and remote areas (see Table 24).
Table 24: 2002-03 Federal Budget measures for residential aged care
2002-03 2003-04 2004-05 2005-06
Measures
Capital assistance for aged care in rural & remote Australia
Increased RAC subsidies
Allowing new aged care residents a 28 day grace period from
Review of pricing arrangements for RAC subsidies
Enhanced assessment of concessional residential status
Sub-total residential care
However, existing Alzheimer's Australia national programs appear under-funded. There has been no real increase in core DESP funding since 1997 and funding was cut with the implementation of DESP
compared to its predecessor program funded under the National Action Plan for Dementia Care. Demand for services is outstripping supply, with long waiting lists for CEWT courses building up in many
parts of the country. At current levels of funding, Alzheimer's Australia services reach only 5-10% of the target group, with even lower penetration in rural and remote areas. Alzheimer's Australia has an
unparalleled reputation for delivering high quality and cost-effective dementia specific services, in part due to the use of well-trained and highly committed volunteers. As such, this delivery vehicle is being
under-utilised – a critical mistake in the current climate. Bird and Parslow (2001), in reviewing Alzheimer's Australia services, proposed that federal funding should be increased from $4m to $13m
p.a. within three years. In 2001-02 funding was roughly $5m. Financing of dementia care will not be just an ageing issue. Being a younger person with dementia can be even more difficult and costly. Dementia care should not be linked exclusively to aged care. In
addition to ACATs, DCATs (Dementia Care Assessment Teams) or even ADCATs (Aged and Disability Care Assessment Teams) should be available to include younger people with dementia, and suitable
accommodation should also be available – perhaps cluster cottage style – for younger people. Another access issue relates to the fact that dementia is increasingly multicultural. Dementia policy and services
should be increasingly multicultural too, and this requires specialist resources. In particular, there is a need for assessment tools that can be used for people from different backgrounds. Moreover, a lot more
still needs to be done to destigmatise dementia.
There is scope for increased use of information technology in improved models of care. One example is
the completion of a US pilot program for an Alzheimer's Caregiver Support System (ACISS), recently
announced by Healthvision Inc. ACISS is a web-based program including information and resources to support family caregivers and improve the care delivery process for key stakeholders. Communication
between clinical professionals, caregivers and patients included videoconferencing and web-based messaging, moderated chats and forums. Caregivers could have their questions answered remotely by
medical professionals, or communicate with their peers without leaving home.86 General practice is another target area for IT-based solutions, as observed in Section 3.2.1 above.
A final consideration is the nature of generations of families and carers of the future. Many
demographers are questioning whether the ‘selfish generations' (baby busters, Generation X, Y and on)
86 See www.healthvision.com
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
will continue to provide the sacrificial home-based care of the past. It seems unlikely that attempts to tip
the balance towards reliance on home-based and community services will continue to reap significant savings. There comes a time where, if families and carers are no longer prepared to provide voluntary
services, home-based care may become as expensive – perhaps more so – than good residential care models. This should be recognised particularly in dementia care strategies of the future.
The fate of many elderly people today is to spend their last years alone, ill and in poverty, segregated
from a society that prefers to turn away from distressing sights. It is a society that believes we are responsible for creating our own success and has little patience with those on whom fate has bestowed
anything less… Devotion is not a word that sits comfortably anymore. We see independence as our birthright. With the long shadow of Alzheimer's stretching in our direction, I wonder how we will cope
with a partner who can no longer ‘do his own thing' or ‘get a life'. Will we care for each other in the way our parents have? And if we don't, who will?
Summary: Intergenerational planning needs to acknowledge the need for health and aged care
spending to grow in real and relative terms, with strategies for successfully managing the change.
These strategies will include minimising inter-generational transfers (fewer young people financing the growing number of elderly), maximising intra-personal transfers (savings schemes), coming to
consensus on the private-public mix of care provision, improving models of care to promote both cost-efficiency and quality and providing safety nets for disadvantaged groups. Access for such groups,
including people with younger onset dementia and people from culturally and linguistically diverse backgrounds, should also begin to be addressed now. More needs to be done to destigmatise
dementia. Better use should be made of Alzheimer's Australia and of new information technologies in delivering services. We should not assume that future generations would provide the levels of voluntary
care that previous generations have provided.
3.3 SCENARIO ANALYSIS OF VARIOUS INTERVENTIONS
This section provides some brief scenario analysis of the potential benefits and cost impacts of various
interventions in dementia care. The cost analysis in the preceding chapter, and indeed cost studies
around the world, have identified a number of principles in prioritising dementia interventions: (1) the financial cost of care for people with dementia, whether provided formally or informally,
increases with disease severity – care needs to be taken not to just transfer financial costs to family carers (indirect costs) in an effort to reduce government (direct) costs;
(2) the financial cost jumps considerably when the person is institutionalised. Policy-makers have
concluded that more efficient outcomes are achieved by supporting home-based care (through
services and financial assistance) for as long as possible, to lengthen the "optimal" level of care;87
(3) any intervention that prolongs life will incur additional costs, in which case the most cost-effective
interventions are ones that ‘buy' the greatest number of DALYs (both through deferred mortality as well as reduced morbidity) for each dollar spent;
(4) big savings in prevention only come from eliminating diseases which cause major disability, of
which dementia is the giant – in which case research is the compelling investment area.
87 In general, a net burden of care is placed on an informal carer if this exceeds the carer's "optimal" level, which may vary
from person to person and often depends on the level of support that carers receive through financial assistance and service provision. More study needs to be conducted in Australia on optimal levels of care, which could perhaps be based on data
from ACAT assessments. At the moment, many indicators seem to suggest that informal carers are either providing longer
than optimal care levels or, to say the same thing another way, receiving insufficient services.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
"With indicated prevention, as pointed out above, prevention may actually cost more money. So why should we bother with prevention? The primary factor to consider is whether people have more
satisfying years of life, which are free from disability, rather than saving the government money."
Three scenarios are analysed – pharmaceutical interventions, participation in family carer support
programs, and research resulting in a cure.
3.3.1
Pharmaceutical interventions
Pharmacotherapies using cholinesterase inhibitors (CEIs) may have three important impacts:
1. permitting a delay in the institutionalisation of a person; 2. reducing the number of hours of informal care-giving required in the short run; and 3. improving the quality of life for patients and caregivers.
There are other beneficial effects – for example, using CEIs may save costs by reducing the use of
other drugs such as antipsychotic medications, of reducing the need for other therapies (such as GP visits, hospitalisations) and of enabling people to continue working – however, these are not included
here due to lack of sufficient large trial data. As noted in Section 1.2.2, treatment of AD with CEIs delays progression of symptoms for nine to twelve months and possibly longer. CEIs have proved effective in 12, 24 and 30 week trials, some studies have
shown that there is no loss of benefit after one year of treatment, and extension studies of placebo-controlled trials have shown that the effects of CEIs may last more than a year.88
88 Studies 1-7 show improvements in nine months of treatment, 8-11 in twelve months, and 12-13 more than twelve months.
(1) Farlow M, Gracon SI, Hershey LA et al (1992) "A controlled trial of tacrine in Alzheimer's disease" The Tacrine Study
Group, JAMA, 268:2523–9.
(2) Rosler M, Anand R, Cicin-Sain A et al. (1999) "Efficacy and safety of rivastigmine in patients with Alzheimer's disease: international randomised controlled trial", BMJ, 318:633–8.
(3) Tariot P, Solomon P, Morris J et al (2000) "A 5 month, randomized, placebo-controlled trial of galantamine in AD"
Neurology, 54:2269–76.
(4) Rogers SL, Doody RS, Mohs RC et al (1998) "Donepezil improves cognition and global function in Alzheimer disease" Arch Intern Med, 158:1021–31.
(5) Thal L, Ferguson J, Mintzer J et al (1999) "A 24 week randomized trial of controlled-release physostigmine in patients
with Alzheimer's disease" Neurology, 52:1146–52.
(6) Rogers S, Farlow M, Doody R et al (1998) "A 24 week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer's disease" Donepezil Study Group, Neurology, 50:136–45.
(7) Qizibash N, Whitehead A, Higgins J et al (1998) "Cholinesterase inhibition for Alzheimer's disease: a meta-analysis of the
tacrine trials" JAMA, 280:1777–82.
(8) Rogers S, Friedhoff L (1998) "Long-term efficacy and safety of donepezil in the treatment of Alzheimer's disease: an interim analysis of the results of a US multicentre open label extension study" Eur Neuropsychopharmacol, 8:67–75.
(9) Winblad B, Engedal K, Soininen H et al (2001) "A 1 year, randomized, placebo-controlled study of donepezil in patients
with mild to moderate AD" Neurology, 57:489–95.
(10) Raskind M, Peskind E, Wessel T et al (2000) "Galantamine in AD: a 6 month, randomized, placebo-controlled trial with a 6 month extension" Neurology, 54:2261–8.
(11) Mohs R, Doody R, Morris J et al (2001) "A 1-year, placebo-controlled preservation of function survival study of donepezil
in AD patients" Neurology 57:481–8.
(12) Doody R, Geldmacher D, Gordon B et al (2001) "Open-label, multicenter, phase 3 extension study of the safety and efficacy of donepezil in patients with Alzheimer's disease" Arch Neurol, 58:427–33.
(13) Rogers S, Doody R, Pratt R et al (2000) "Long-term efficacy and safety of donepezil in the treatment of Alzheimer's
disease: final analysis of a US multicenter open-label study" Eur Neuropsychopharmacol, 10:195–203.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
In the following analysis, the work of independent and award-winning researchers Lopez et al (2002) in
assessing the effects of these improvements on traditional milestones for AD have been utilised, and applied to the Australian situation. Lopez et al (2002), in an open label study, assessed cognitive
function using the MMSE (endpoint less than 9), ADL using the Blessed Dementia Rating Scale (BDRS, endpoint 12 or more), and institutionalisation based on admission to a ‘nursing home' (including US
‘personal care' and ‘healthcare' facilities ie, the equivalent of either low or high care Australian facilities). The results (see Table 25) showed that people who used CEIs:
□ improved on all measures, with fewer than controls reaching the end-points (MMSE <9, BDRS 12+,
institutionalisation);
□ had significant difference in the rate of change in MMSE (16.3 the average for CEI users compared
to 6.2 for non-users) – expected average decline 2.5 points for users and 3.5 points for non-users;
□ had significantly higher BDRS scores for ADL (4.7 compared to 7.3 for non-users, and a significant
difference in the rate of change);
□ had significantly less institutionalisation (6% after three years compared to 41% for non-users) – this
is supported by other studies, for example Knopman et al, 1996);
□ no significant association was found between CEI use and time to death.
Table 25: Outcomes of patients using CEIs compared to controls after 36 months
% total # Controls
Institutionalisation
Source: Lopez et al (2002).
The research team concluded:
"Whereas short term benefits in cognitive and functional competence with CEI use are to be expected, it is the longer term outcome (the delay of entry into a nursing home) that demonstrates
the powerful effect of these drugs. This suggests that physicians should be cautious in judging the medication response after only a few months of treatment, as the full benefits of CEI use take place
over a longer time frame."
An implication for Australia is that the six-month review period required by the PBS for access to subsidised CEIs is too short. Furthermore:
"The fact that the use of CEIs delays time to nursing home admission and does not affect physical
survival has important scientific and public health implications. The CEIs seem to allow patients to maintain relatively normal activities of daily living for a longer period of time, but to do so without
significantly prolonging life."
1. Delay in institutionalisation
Chart 16 illustrates the delay in institutionalisation, with the ‘survival rate' for CEI users significantly
higher even after 84 months. Clearly it is the area between paths A and B that represents the potential
saving in institutional costs, with differences emerging from early on. It is interesting to note that in the first 24 months, nearly 20% of the control group had been institutionalised whereas none of the CEI
users had found this necessary at this stage.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Chart 16: Kaplan-Meier plot of time to nursing home admission among patients with AD
(A) taking and (B) not taking cholinesterase inhibitors.
Notes: A: n=135, B: n=135. 130 patients took donepezil, 22 took tacrine and were switched to donepezil, and 6 took rivastigmine. Nursing homes include the equivalent of Australian low or high care facilities. Source: Lopez et al (2002).
There are a number of possible approaches to modelling the effects of delays in institutionalisation due to use of CEIs. In submissions to the PBS, applicants are required to adopt a dynamic modelling
approach where the number of people in the target group are identified; adjustments are made for those refractory to treatment, who die during treatment (eg, from a stroke or heart attack) or who for some
other reason discontinue treatment; as well as individualistic (probability/risk) modelling of entry into residential care. Adjustments are made for changes in prevalence of the condition as well as the various
impacts of the drug usage over time, with savings then identified in the initial and subsequent years until a steady state is reached.
An alternative approach, and the one adopted here, is to model steady state equilibrium positions with
and without the intervention – like a ‘before' and ‘after' snapshot picture – but assuming the final steady state occurred in relation to the current prevalence pattern, to enable a ‘what if' comparative analysis.
Such an approach would not necessarily need to be limited to the populations for approved use as per PBAC rulings; in this case the modelling is applied to the population of all people with dementia, rather
than just those with AD (the current PBS restriction) due to the growing evidence noted earlier that other non-AD forms of dementia may also respond similarly to treatment with CEIs. As such, this might be
considered an ‘extreme' scenario of maximum leakage from a PBS perspective. Applying the Kaplan-Meier plot in Chart 16 above to a comparative steady state model, and as noted in Table 25 above, the difference between the CEI users and the control group was 35% at 36 months, or
an average delay in institutionalisation of 12.71 months. This is also in line with the wealth of other literature noted earlier showing an average impact of improved symptoms of 12 months.
A delay in entry to residential care has three impacts – savings in residential care cost, increased
expenditure on formal community care costs, and increased expenditure of informal care resources. Note this is just the isolated cost of not being in an institution, not the other advantages of wellness,
which include lower carer burden and improved quality of life (being able to work, lower healthcare usage), which are addressed below. The costs of residential and formal and community care per person
per annum have been estimated in Chapter 2.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
A 12-month delay in institutionalisation would effectively mean that 12% of people with dementia
(19,476 people) would not go into residential care that would have otherwise, as illustrated below:
Steady State 1 Community Care – 52%
Residential Care – 48%
Steady State 2 Community Care – 64%
Residential Care – 36%
It is assumed that all people are treated in the community while their dementia is still in the mild to
moderate stage, but people who are already in residential care due to reasons other than their dementia are not modelled as being treated with CEIs. This approach is adopted in order to quarantine the effect
of the dementia treatment, rather than the more complex interactions of other factors also. Results are depicted in Table 26. In this comparative static analysis, the Federal government would be $597 million better off if residential care could be delayed for a year. Family carers, however, would be
$320 million worse off. Overall, there would be a net real economic saving of $276 million ($1,701 per person with dementia or $14,178 per entry avoided) from delaying institutional care for one year.89
Table 26: Savings, residential care deferred one year, Australia, 2002,
Steady State 1
Steady State 2
Type of cost
$/person p.a. No. people Total ($m) No. people Total ($m)
Residential
Residential care
Community
Formal (Fed) comm. Care
Informal community care
Net difference
Savings per entry avoided (Fed)
To Fed government
Savings per entry avoided (total)
To informal carer*
Savings per person with dementia
Total 276
* Not including gaps (residential care fees, community care payments). Source: Access Economics
From where does the net saving derive? It is speculated that residential care involves higher costs per unit due to additional capital and administrative costs – there are no tiers of management for the home
carer. Certainly the finding is common to international studies. In Italy for example, Trabucchi and Bianchetti found savings of around US$4,000 (A$8,000) per
person per annum through preventing a 4-point/year decrease in
Delaying residential
MMSE score in a year (the equivalent of CEI therapy). Leon et al
care for one year saves
(1996) estimate average total monthly cost of caring for an AD
government $600m but
patient in 1996 was US$2,306; US$1,827 formal services and
US$479 of informal care, of which US$2,029 can be saved if
makes family carers
disease progression can be slowed – 88% of the total or nearly
$320m worse off.
US$25,000 per person p.a. Rice et al (1993) estimate that average annual formal carer costs for institutionalised persons
89 Note that this is not the same as simply subtracting total community costs ($510m) from residential care costs ($712m) –
which would suggest only a $202m saving – because carer payments are a transfer cost. Delaying residential care causes
$75m to be gained by informal carers but lost to Federal government, thus the net effect is $202m plus $75m = $276m.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
with AD amounted to US$42,049 per patient, more than three times the cost for non-institutionalised
persons, suggesting savings in the order of US$30,000 per entry avoided. On this scenario there are likely to be additional savings due to the reductions in informal care hours required, to which we now turn.
2. Reduction in hours of informal care required
If delaying residential
care for one year is
From the analysis above (Table 26) we saw that, if there were
no change in health level, family carers bear the brunt of care in the community rather than in an institutional setting.
reduced care hours,
everyone is better off.
However, because of the better outcomes in both cognitive
function and ADL (nearly 50% better in each case), it is postulated that the hours of care required for the year of residential care avoided would actually be able to be costed at the level for mild dementia. The
reduction in hours of informal care can be measured, once again adopting the replacement cost approach. This results in a 16.5 hour per week saving, using the University of Michigan Study results
(see Sections 1.5.1 and 2.2.2), only 34% of the hours of care of moderate dementia. Thus the replacement cost would also be 34% and, in similar vein, the carer payments and formal care service
hours required. The savings under this scenario are modelled in Table 27 below. Once again, it should be noted that this is a comparative static analysis of the whole population of people with dementia,
rather than a dynamic analysis of just those eligible for PBS-listed drugs.
Table 27: Savings, one year deferred residential care, symptoms improved, Australia, 2002
Steady State 1
Steady State 2
Difference
Type of cost
$/person p.a. No. people Total ($m) No. people Total ($m)
RESIDENTIAL
36,547 77,902 2,847.1 58,427 2,135.3
Community
Formal (Fed) comm. care
Informal community care
7,307 44,394 324.4 54,638 236.0
Net difference
Savings per entry avoided (Fed)
To Fed government
Savings per entry avoided (total)
To informal carer*
Savings per person with dementia
Total 959
* Not including gaps (residential care fees, community care payments). Source: Access Economics
Table 27 shows that, if residential care is delayed together with reduced care hours, equating to
delaying the progression from mild to moderate dementia for one year, then net savings in a year are nearly $1 billion – $276m from delaying institutionalisation, and $683m from reducing the extent of
informal and community care services needed. Smaller packages are being provided to more people. The benefit here is that there is ‘Pareto optimisation' – nobody is made worse off in buying an overall
economic gain. Indeed, benefits under this scenario are now $5,906 per person with dementia p.a. (closer to the Italian savings estimate also).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3. Improved quality of life
Moreover, CEI use
Finally, if progression of dementia to the moderate stage is deferred
increases Australia-
for one year, a person's quality of life is improved. Section 2.3 showed that the disability weightings for moderate dementia are 0.63,
wide ‘health-span' by
compared with 0.27 for mild cases. The disability burden of the
over 15,425 DALYs
severe cases does not change (still 48,689 people). However, more
people move from the ‘moderate' burden (now 22,072) into the ‘mild' burden category (now 91,535). For 42,846 people, then, there is an
extra 0.36 DALY each. Australia-wide, the gain is 15,425 extra years of healthy life! "Within the next 20 years, Alzheimer's disease will likely surpass heart disease and cancer as the most costly disease in America… Medical interventions are becoming more promising, and with them comes
the possibility that the economic burden of the disease may be lessened and, more important, clinical benefits realised. By improving cognitive function with pharmacotherapy, it is possible to reduce
caregiver time, delay nursing home placement, and improve quality of life."
Meek et al 1998, p72
And the cost of the treatment? Treating all Australians with
Returns to investment in
mild dementia, as cases arise (ie, incidence), and assuming that the drug cost is $160 per month, would yield a total cost of
CEI use are 7:1, plus a
$39m in the first year. However, to reach the steady state
equilibrium as modelled above, the ongoing annual drug cost
healthspan for people
would be $139m. In terms of cost: benefit ratios, there would be a return to Federal government of around 6:1, and an
overall return of at least 7:1.
3.3.2
Support for family carers
Benefits of support programs have been researched in a number of studies. One study, the Mittelman study from New York, showed that family carers of people with AD who received family and individual
counselling were able to give care for almost a year longer than those in the control group. In Australia, Brodaty has shown that involvement in a ten-day training course, with follow-up from a key worker for at
least twelve months, lowers levels of stress and depression in family carers. The cost of the Early Stage Dementia Support and Respite Program in Australia, in terms of providing 1:1 support, is estimated as $37.50 per hour provided or, assuming the equivalent of weekly one-hour
sessions as the model of care, $1,950 per person per annum. Alzheimer's Australia has suggested in its 2003-04 Budget Submission that spending of $300,000 is indicated to extend this program in the
community to meet current demand. This level of funding would provide 8000 hours of care or help 154 people according to the scenario modelled here. From the previous scenario, we know that savings per
nursing home entry avoided would be $14,175 after compensating families and carers, even if there were no net benefit to health. This saving for all 154 people would result in overall savings of $2.18m, or
a cost: benefit ratio of 1:7. This might be taken into consideration in the current evaluation of the program, and might even suggest a larger budget for the program than the proposed additional
$300,000. The outcomes are summarised in Table 28.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Table 28: Returns to Support Spending, ESDSRP, 2002
ESDSRP new spending
investment in support
Hours of support
programs may also
Per carer 1hr/wk, 52wks
be in the order of 7:1,
Numbers of people helped
plus increased in
Savings per entry avoided
154 people not institutionalised
healthspan for family
Return to $1 p.a.
$7.27
3.3.3
Research resulting in a ‘cure'
The magic bullet. It may not be as long a shot as it appears90. Hatfield, Sonnenschein and Rosenberg (2000) summarise the research of Murphy and Topel on the economic value of investment in medical
research over the longer term. Some of their findings include:
□ roughly one third of the total health savings are a result of medical research that led to new drugs
and treatment protocols, with 3:1 consistent average long term returns;
□ the order of magnitude of savings for ‘big' diseases are huge – the savings from prevention and
treatment of cardiovascular disease over the 1970s and 1980s were US$1.5 trillion, representing an average return of US$500 billion per annum, while research success that spared just 1 cancer
death in 1000 would be worth US$46 billion p.a. (the total US research budget – private and public
is US$45 billion);
□ small programs can also reap exceptional returns – for example a 17-year program which invested
US$56 million in research on testicular cancer led to a 91% cure rate and ongoing annual savings of US$166m;
□ the economic value of longevity rises as society becomes more prosperous and the value of curing
or preventing chronic diseases of ageing such as dementia, is rising as average age of the
population rises;
□ progress in research against one illness increases the value of progress against another; and □ these estimates are purely financial – they exclude the benefits of increased healthspan.
Applying these principles to dementia research in Australia, the case for higher funding levels is even more compelling. Table 29 summarises the issues. The real cost of dementia is $5.6 billion, while our
current Federal investment in finding a ‘cure' is around $2.5m p.a. (see Section 3.2.3). This is compared to a suggested investment of $49m p.a., which would bring Australia in line with current US spending.
On the basis of the long term average for medical research investment, $1.9 billion of research would be required to find a ‘cure'. At the current investment level, we won't find a ‘cure' for 748 years. If we spent
at target, we would find a ‘cure' by around 2040. The magnitude of health savings in current dollars would be around A$4 trillion.
90 It should be noted in this scenario that what is being modelled is the extreme case of a prevention or treatment being
discovered that is able to completely eradicate dementia, as with polio, and such as might be promised by a future ‘vaccine'. In reality, the multi-causal aspects of dementia diseases might mean that ‘cures' form a spectrum of outcomes including
disease reversal or significant delay of onset, substantial reduction of symptoms and extension of quality life through
improved management (as with AIDS), and the like.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Table 29: Returns to research investment in Australia
Real cost of dementia ($m)
Investment in cure (current)
Increasing research
Investment in cure (target)
to $49m p.a. could
Ratio of returns
Implied research level required ($m)
save Australians
Years to cure (current)
$4 trillion in future
Years to cure (target)
Difference in years
Potential cost savings ($m)
3.3.4
Summary of scenario analysis
1. Delay of institutionalisation for 12 months saves the Federal government $600m but makes
families and carers $320m worse off, with net overall savings of $14,175 per entry avoided;
2. Delayed progression of illness – mild rather than moderate – together with delayed
institutionalisation is preferred, as families and carers would be $136m better off and the Federal
Government $823m better off, with overall savings of $49,219 per entry avoided.
3. use of CEIs achieves both the above outcomes with returns of 7:1 on investment, as well as saving
15,425 DALYs – a 13% increase in healthspan for people with dementia.
4. support programs for family carers – such as delivered through the ESDSRP, also accrue
returns of around 7:1 on investment, together with valuable health outcomes for families and carers.
5. research resulting in a cure – increasing research funding to $49m p.a. from the current 2.5m
could generate a cure by 2040 and save Australians $4 trillion in future health costs.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
4. OPTIONS AND CHALLENGES
"While much has been done to assist people with dementia and their families and carers, much remains
to be done. Given the scale and progression of the epidemic, simply doing whatever the community is already doing means going backwards and going backwards at an ever-increasing rate."
Alzheimer Australia's submission to the 2003-04 Federal Budget
4.1 SETTING THE SCENE
4.1.1
National Action Plan for Dementia Care
This section briefly outlines where we have come from in strategic planning for the dementia epidemic. The five-year National Action Plan for Dementia Care (NAPDC) was instituted in 1992. It set a strategic
direction for dementia care designed to strengthen the capacity of the aged care system to better meet the needs of people with dementia and their families and carers. Rather than advocating a separate
stream for dementia care services, it aimed to integrate the various aspects of dementia care through the aged care sector and programs. The Action Plan set targets and actions for achievements between
1992-93 and 1996-97 in seven key areas, namely:
□ diagnoses and assessment; □ services for people with dementia; □ services for families and carers of people with dementia; □ quality of service; □ community awareness; □ research and evaluation; and □ policy and planning.
Midterm review of the NAPDC identified the priority need for a more coordinated approach to dementia
care training for all staff working in residential aged care facilities. The National Residential Dementia Training Initiative (NRDTI) was thus established to provide systematic training for staff in
Commonwealth funded residential aged care facilities in order to improve dementia care practice. The NRDTI also aimed to facilitate the longer term capacity of the aged care industry to sustain dementia
care training beyond the Initiative. Other challenges highlighted by the NAPDC included special problems in rural and remote communities
and continued harnessing of political will, particularly at State and Territory government level. The NSW Government implemented the five-year NSW Action Plan on Dementia 1996-2001 and has recently
released the next plan "Future Directions for Dementia Care and Support in NSW 2001-2006".91 Victoria has also produced an excellent policy statement, "Dementia Care and Support in Victoria: 2000 and
Beyond." 92 All States and Territories have to some extent either produced dementia-specific strategic plans and/or incorporated dementia aspects into mainstream service planning.
The 1997 Aged Care Reforms were introduced in part to improve the structural service delivery for older
Australians with complex physical, mental and psychogeriatric needs. Fine-tuning continued through the National Strategy for an Ageing Australia93 (2001), towards the thematic goal of ‘world class care'.
91 The NSW strategy is at http://www.add.nsw.gov.au/PDF/Future%20Directions%20CD%2010.9.pdf 92 Victorian Government Department of Human Services, November 2000, available on www.dhs.vic.gov.au/acmh 93 The National Strategy is available on www.health.gov.au/acc/ofoa/documents/pdf/nsaabook.pdf
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
4.1.2
Aged care reforms and the Two Year Review
Professor Len Gray reported specifically on dementia care in the Two Year Review of Aged Care
Reforms, which was finalised in 2001. He stated that the government is working towards a national dementia policy framework, with first steps being the August 1999 Dementia Forum, additional DESP
funding, expansion and enhancement of respite services including Carer Respite Centres, carer training, new funding for the Early Stage program and the national helpline, growth in PGUs and training
in dementia care for people from diverse cultural and linguistic backgrounds. He noted that the former Personal Care Assessment Instrument (PCAI) and the Resident Classification Instrument (RCI) had not adequately recognised the amount of staff time required to care for residents
with dementia, as also recognised by Rosewarne et al (1997). Also, because funding levels were not linked to the severity of behavioural problems of people with dementia and did not recognise the
resource intensive nature of dementia-appropriate care, he concluded that "a major disincentive to caring for these residents was built into the system" Gray (2001, p214). Gray noted that Cuthbertson,
Lindsay-Smith and Rosewarne (1998) found that the ‘new' Resident Classification Scale (RCS) introduced in 1997, increased funding for residents with cognitive impairments and behavioural needs
by some 20%. While in theory this might be true, critics argue that it does not occur in practice and that, as validated by the RCS assessors, the RCS is hostile to dementia care. This is because questions 8-14 of the RCS,
the behaviour questions that most likely relate to dementia specifically, constitute as little as 16% of funding and that Q 8 and 12-14 are four of the six most downgraded questions by validators. Moreover,
negative incentives occur since the system rewards perverse behaviours, rather than rewarding quality care that effectively prevents and manages those behaviours.
The Two Year Review noted "some participants considered that access to care for people with
behavioural problems has not improved, as some providers are reluctant to admit residents who exhibit difficult behaviours and are unable to provide secure accommodation." Gray (2001) also concluded that:
□ there is a lack of data regarding dementia in residential care, although proxies can be derived from
RCS weighted scores of those who probably and possibly have dementia; these data showed that
91% of residents in high care homes and 58% in low care homes fell into either category, including almost all RCS1 (99%) and RCS2 (95%) residents;
□ the consultation process highlighted a lack of specialised and secure accommodation for people
with moderate to severe dementia, and insufficient financial support for providers to supply it;
□ there was insufficient data to comment on the need for secure and segregated accommodation,
although noting that the government identified priority pockets of need for dementia-specific care for
the first time in the 2000 capital works Approvals Rounds;
□ priority in Approval Rounds and the changes in the RCS will not necessarily deliver an appropriate
quantum of dementia specific homes in every region of Australia.
□ It is recommended that further investigation be undertaken into the needs for and provision of
accommodation and care options for people with dementia. Such an investigation should include a focus on infrastructure and options for addressing identified deficiencies.
For a two-year review, this single recommendation for ‘further investigation' is insubstantial. One would
hope that such investigation was ongoing anyway. In the discussion, there also seems to be little appreciation of the problems related to the various capital and recurrent funding issues for high care and
low care facilities respectively or the problems in the RCS, which had the opportunity to identify and provide for dementia behaviours and environments and did not. Rather, although the ACAT/RCS
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
instruments have improved on the former PCAI/RCI instruments, they have not addressed the key
issues as they continue to classify and weight needs primarily in terms of nursing needs, provide insufficient data for the evaluation of dementia outcomes, and fail to address the issues associated with
financing capital costs. The review also failed to look at particular non-residential care needs for people with dementia.
The fairly blunt industry response to the review is summarised in Aged and Community Services
Australia (2001), including a number of ‘real world aged care economics' examples and case studies precipitating negative returns on investment, concluding (p10) that:
"The Report… leave[s] the reader with the view that the reforms have fixed all the significant
problems in aged care and that all of the measures introduced since 1997 are working smoothly and effectively. As this Industry Response has shown, nothing could be further from the truth.
The aged care industry is fast reaching a crisis point in terms of its ongoing viability. It is unable to
gain access to the capital required to make necessary building improvements or to finance the new beds needed. The industry is drowning in an increasing volume of red tape and is facing increasing
difficulty in recruiting staff it needs to provide quality care… Older people still suffer the consequences of poor coordination between the health and aged care systems. They still experience significant problems in gaining access to the services they need.
They still suffer from failures in the quality of care. Older people deserve better. Resting on its laurels is not a viable option for any Federal Government. That should be the real conclusion of the Two Year Review of Aged Care Reforms and the basis for a genuine Government
In its response to the Two Year Review, the government accepted the recommendation and pointed to:
□ Claims that average funding per dementia resident had increased 124% since 1997 (no data
provided, and no description of how dementia residents were identified);
□ $92.5 million over 4 years to expand respite for families and carers of people with dementia;
□ establishment of a working group to consider the care and accommodation needs of people
The Report of the Working Group on Dementia Specific Aged Care has just been released, concluding
that there is scope for improvements to accommodation and care options across all tiers of dementia needs. Specific conclusions and departmental responses are94: 1. More research and evaluation is needed on effective care services for people with dementia. Response: Making services more effective for people with dementia will be considered further in the
Community Care Review. 2. Joint Commonwealth/State/Territory action is required for people with extreme or severe
behavioural and psychological symptoms of dementia.
Response: The Commonwealth Government will discuss options with the State and Territory
94 Department of Health and Ageing (2002b), p21.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
3. While appropriately structured residential aged care services are sufficient for many people with
dementia, planning should take account of the need for dementia specific care, both residential and community.
Response: The needs of people with dementia will be considered in the Review of Pricing Arrangements of residential aged care and the current review of RCS funding options. 4. Access to respite care for people with behavioural and psychological symptoms of dementia needs
to be enhanced.
Response: The needs of people with dementia will be considered in the Review of Pricing Arrangements of residential aged care and the current review of RCS funding options. It should also be
noted that the 2002-03 Federal Budget provided $10m for Commonwealth Carer Respite Centres to top-up payments to facilities offering dementia specific accommodation. Additionally, the 2002 Budget
includes $10 million over four years to expand the Psychogeriatric Care Units to achieve national coverage as a Commonwealth only program. 5. A greater emphasis is needed in community care on the provision of dementia specific programs
delivered by trained staff.
Response: This will be considered further in the Community Care Review. 6. There are gaps in the early intervention services for people with dementia and their families.
Depending on the outcomes of the evaluation, the Alzheimer's Association Australia Early Intervention project (funded by the Commonwealth) may be a model for such a service.
Response: This will be considered in the evaluation of the Early Stage Dementia Support and Respite Project.
4.2 THE FUTURE VISION
Disease and disability associated with dementia are not inevitable consequences of ageing. The
challenge of the dementia epidemic that is now, in 2003, becoming increasingly evident, is to attain declining disease and disability rates amidst a steep rise in the number of older people. The task is
urgent. But there is broad scope to implement a positive agenda that can sustain an effective response over the coming decades.
In Australia, our mental health and broader health goals should be aimed primarily at increasing
‘healthspan' – years of healthy, active life expectancy. To this end, we must adopt a longer term national vision about future action – not just in terms of disease management, but also in terms of action that
government, academia and the private sector can jointly pursue to prevent and ultimately cure dementia.
A national vision requires a nationally coordinated approach. Commonwealth and State and Territory
governments must come together with health professionals, people with dementia and their families and carers to acknowledge and plan for the demands of an illness that is poised to become Australia's
number one health issue in the next two decades. Secure political commitment and consensus among stakeholders is essential.
With the first wave of baby boomers commencing retirement in 2005, the demographic transition is now
firmly underway. In that fiscal context, it is crucial to not simply put more money into ineffectual systems but rather to shift health spending from acute to chronic care models to maximise returns from limited
resources and to utilise evidence based approaches. Moreover, many interventions to date have been suboptimal, if not myopic, focusing on direct costs rather than the enormous benefits of investments in
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
wellness. Whole economy analysis, including impacts on the labour market and other sectors, must be
considered from now on in policy development for healthy ageing and dementia care. Strangely, the enormity and priority of the dementia epidemic has not yet been acknowledged in national policy making. Dementia is already intricately linked with recognised national health priorities
including cardiovascular disease, diabetes and depression, and it is the mostly costly area of mental health. Dementia prioritisation, and a national strategy to realise the vision, is long overdue.
Five key elements of the future strategy must involve:
□ a significant investment in research for cause, prevention and care; □ early intervention through improvement in diagnosis, and the provision of cost-effective
pharmacotherapies;
□ comprehensive provision of support, education and respite services – in place in the community as
far as is optimal;
□ quality residential care, appropriately financed, that are centred on the person with dementia and
their family/carer; and
□ provision for special needs, including people with younger onset dementia, people with special
BPSD needs, people from culturally and linguistically diverse backgrounds, indigenous Australians and people in rural and remote areas.
If, starting today, we embark on such positive strategies, Australia can lead the way in effectively and
smoothly managing the dementia epidemic transition. "Thanks to the efforts of thousands of carers, the last 20 years have seen the stigma of dementia at best reduced but not removed. A positive approach to planning dementia care now will ensure that in
twenty years time the quality of life of people with dementia, their families and carers will be much improved – a society truly committed to the prevention of dementia. That is the vision of the Alzheimer's
Association Australia."
Alzheimer's Australia,
Submission to the Parliamentary Inquiry on the Ageing of the Australian Population, 2002
4.3 STRATEGIES AND RECOMMENDATIONS
4.3.1
Prioritisation of dementia
Dementia should be a
national priority. It is
Because of the impact of demographic ageing and the importance of dementia in overall health costs and disease burden, dementia
set to become the
(and the nexus between ageing and mental health more generally)
Number One cause of
must be incorporated in Australia's priority setting for health and
disability burden in
Australia by 2016. It
Most telling is that dementia, after depression, is already the
will touch many of us
second largest cause of disability burden in Australia (ahead of
directly of indirectly.
diabetes, asthma, osteoarthritis and the other health priority areas), and it is growing much faster than depression so is set to become
the number one cause of disability burden by 2016.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Chart 15: Burden of disability of dementia and depression, ‘The Big Two', 1996-2031
YLD - ('000) 60
Source: Access Economics projections, based on AIHW and ABS data.
The issue is how and where to prioritise. Dementia does not fit completely comfortably in either the aged
care of mental health portfolios. Currently dementia care is funded primarily through aged care programs and the risk of dementia increases sharply with age. Moreover, some stakeholders are not
comfortable with the mental health categorisation of dementia in international and disease classifications given remaining stigma.
Although mental health is one of Australia's seven national health priorities, together with cardiovascular
disease, cancer, injuries, diabetes, asthma and chronic musculoskeletal disorders (notably arthritis and osteoporosis), the National Mental Health Strategy has not embraced dementia. The mental health care
resources list on the federal departmental website has 666 words, none of which is ‘dementia' or ‘Alzheimer's' (see www.mentalhealth.gov.au/resources/). Searching the mental health home page for
the word ‘dementia', yields no hits at all (www.mentalhealth.gov.au/index.htm). Whatever decision is taken on the most effective point of coordination of planning dementia, it is clear that a whole of government approach is needed. This is because dementia care is so broad ranging,
covering aspects of aged care, community care, residential care, medical services, psychiatric and specialist services, pharmaceuticals, workforce and housing.
Recommendation 1: Dementia should be a national health priority. Because dementia issues are so
broad ranging – covering aspects of aged care, community care, residential care, medical services, psychiatric and specialist services, pharmaceuticals, workforce, housing, research, technology, finance
and so on – a coordinated sector-wide approach needs to be adopted in addressing these recommendations. It is vital that dementia initiatives are no longer lost between bureaucratic divides or
governmental tiers, being referred from one review to the next without concrete action. Rather, priority should be accorded within public sector programs, resources and funding in a coordinated and
comprehensive manner. The current National Mental Health Strategy review and the Residential Aged Care Pricing Review should provide concrete proposals for addressing the issues raised in this report. Consideration should
be given to including a central coordination point for future ongoing dementia planning and care, perhaps as part of a more strategic approach to neurodegenerative disease.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
4.3.2
Recommendation 2: The funding of dementia research should form an essential part of the
government's response to the dementia epidemic, as well as forming part of a more general
reprioritisation of health research resources on the basis of projected prevalence, costs and disease burden. In view of Australia's international comparative advantages in health research investment, as
well as the potentially enormous cost-effective returns (potentially saving up to $4 trillion in Australia in long term health costs), urgent action should be taken to substantially boost the level of research
funding for dementia including:
□ Official research funding for dementia should be increased to $49m per annum within three years,
with prioritisation of specific projects determined in conjunction with Alzheimer's Australia.
□ Research priorities should be directed towards:
• Cause: Understanding of the biomedical causes of dementia, including epidemiological
(population-based) medical risk factors and public health research95;
• Cure: Measures that prevent or postpone the onset of dementia, or that slow or reverse disease
progression96;
• Care: Effective models of care (best clinical practice) for people with dementia, including ways
to enhance primary care, dementia services (as per Section 3.2.5) and effectiveness of training
interventions.97
□ Research should be collaborative and multidisciplinary, including the interaction of other conditions
on dementia (eg, diabetes), and the interconnections between different types of dementia, with emphasis on prevention, healthy brain ageing and effective quality care.
4.3.3
Prevention and early intervention activities
Recommendation 3: Promotion of dementia prevention activities should be initiated, targeting the
community and health professionals (particularly in primary care), possibly in conjunction with other
stakeholders including consumers groups (such as the Heart Foundation) and official bodies, including:
□ addressing cardiovascular risk factors – reducing hypertension, cholesterol and homocysteine
(folate) and anti-platelet treatments;
□ promoting good diet, exercise, quitting smoking, and drug and alcohol programs as dementia
prevention activities as well as promoting health generally;
□ promoting ongoing awareness to reduce other dementia risk factors such as head trauma (eg, seat-
belts, helmets etc), occupational hazards (eg, exposure to electromagnetic fields) and others as
revealed or confirmed by ongoing research.
95 This research, together with awareness campaigns, has enabled diseases such as lung, skin and breast cancer to be seen
as conditions with preventable elements subject to a public health approach. 96 Specific research priorities might include amyloid-based treatments (including immunisation), new drug treatments
(including with memantine), anti-inflammatories, oestrogen therapies, anti-oxidants and nerve growth factor supplementation. 97 Specific priorities include research on diagnosis, effects of care standards (community care, long term care, terminal care,
care needs and planning), carers' support, alleviating distressing behavioural symptoms and pain for non-verbal patients,
medication for nursing homes and research into true levels of awareness (insight) in dementia (Maller and Rees, 2002).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
4.3.4
General practice
Recommendation 4: To address the gaps and unmet need in current service provision, measures to
enhance GP services should be initiated or expanded, including:
□ GP education and support in implementing models of care that include early diagnosis, care
planning and information about the support available for people with dementia, their families and
□ GP training and appropriate remuneration for ongoing management of dementia;
o introduction of a program for ‘dementia-accredited' GPs
o review the rebate scheme for GPs visiting patients in residential care;
□ teleconferencing and other initiatives to support more isolated GPs in diagnosis and treatment.
4.3.5
Other medical and acute care services
Recommendation 5: To address quality, cost and workforce issues in acute care, measures are
required to:
□ ensure quality person-centred dementia care is available throughout the acute care system; □ prevent admission to the acute care system through better treatment of people with dementia in
their own (family or residential) home, including possibly psychogeriatric services to complement ACATs;
□ assessment of acute care hospital waiting times for transfer into residential facilities, relative costs
and potential mechanisms for reducing these, such as ‘Innovative Places' or similar models; and
□ measures to enhance recruitment, retention and training of nurses in dementia care, possibly
utilising moneys from the $47.5m (2002-03 to 2005-06) announced last budget for aged nursing;
□ workforce measures to increase training, recruitment and retention of specialist geriatricians; and □ greater investment in specialist referral services (such as memory clinics) to support GPs in
diagnosis and management of people with early stages of dementia.
4.3.6
Recommendation 6: Affordable access to medications appropriate to their diagnosis should be
expedited for all people with dementia. Current PBS arrangements should be replaced by a simpler
access regime comprising:
□ diagnosis confirmation by a specialist or by a dementia-accredited GP; □ ongoing access predicated on best clinical practice, which might involve, for example:
o regular monitoring of broad patient outcomes such as maintenance or improvement in cognition
and/or social functioning, including for people who have non-Alzheimer dementia;
□ access to telephone approval of authority scripts.
Pharmaceutical expenditures should not be seen as a cost but rather as an investment in wellness:
□ PBS cost-cutting measures that are not evidence-based should be avoided;
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ subsidies should encourage pharmaceutical interventions for dementia based on Clinical Practice
Improvement studies, and noting that this study shows returns to investment in cholinesterase inhibitors of 7:1 due to delays in institutionalisation and reduced carer burden, together with
improved quality of life;
□ treatment of agitation in dementia and access to anti-psychotics should reflect existing evidence;
□ longer term differences, rather than just those limited to six months, should be considered.
4.3.7
Home and community support services
Recommendation 7: While much has been done to enhance home and community services in recent
years, remaining priorities include:
□ a one-off 20% increase in the Home and Community Care (HACC) program funding; □ 6% growth per annum in HACC funding (to cover demographic ageing based prevalence increases)
plus an indexation amount that more adequately covers increased costs in service delivery, to be negotiated in consultation with key stakeholders;
□ greater inclusion of the voluntary sector (including families and carers) in the formulation and
implementation of policy with respect to people with dementia and their families and carers.
4.3.8
Families and carers
Recommendation 8: Family and carer support, education and respite remain an ongoing challenge, as
well as one of the most important aspects of managing the epidemiological dementia transition. A long term strategy is required to be developed by key stakeholders. There have been advances in family
and carer services in recent years, but current evidence suggests that care support remains sub-optimal (ie, an undue burden on families and carers). Additional measures should include:
□ consideration of "optimal' informal care levels with a view to setting guidelines and targets for long
term planning purposes;
□ additional recurrent funding to promote best practice in respite care including:
o incentives for implementation and diversification of 'carer friendly' models of respite care,
including facility-based respite services, building on pilot studies; and
o respite services which cater for people with the specific behavioural and psychological
symptoms of dementia (BPSD);
□ applying best-practice carer education and support models identified by research, pilots, trials and
evaluations which, as with cholinesterase inhibitors above, show potential average returns around 7:1;
□ improve incentives to encourage increased employment participation and retention of families and
carers, including flexible work practices such as part-time home-based work, work-based adult day
programs, workplace dementia awareness and destigmatisation.
Please remember this: Community care is good policy – but only if it acknowledges that the home-
based care of a person with dementia can be a skilled, exhausting, costly, long-term, lonely job for the
person doing the caring. It must be properly resourced to be accessible to all Australians.
Alzheimer's Australia (2001a)
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
4.3.9
Strengthening community services provided though Alzheimer's Australia
Recommendation 9: Any strategic national plan to address the dementia epidemic in Australia must
include nationally consistent and longer-term funding arrangements between governments and the
voluntary groups providing services to people with dementia, notably Alzheimer's organisations, which are cost-effective and high quality delivery vehicles, due in part to the dedication of volunteers. Long
term recurrent funding arrangements need to be negotiated with Alzheimer's Australia, including:
□ a one-off increase in funding for Alzheimer's Australia from $5m pa in 2001-02 to $13m by 2003-04,
with annual indexation reflecting both cost-price factors and increases in numbers of older people, to enable:
extension of Carer Education and Workforce Training (CEWT) courses, accredited courses for workers in residential care, and to meet special needs of families and
increased Dementia Education Support Program (DESP) funding for national
expansion of counselling services, including additional full time counsellors in NSW and Victoria and part time staff in other States and Territories;
expansion of the Early Stage Dementia Support and Respite Program (ESDSRP) (currently being evaluated), and/or additional funding provided for a new program for
support and respite for people with mid-stage dementia, based on the results of successful pilot projects undertaken by State and Territory organisations;
additional funds to meet the specific requirements of people with dementia and their families and carers with special needs, including people from culturally and linguistically
diverse backgrounds, indigenous people and people with low levels of literacy, and people in rural and remote communities;
expanded information resources projects including on Down's Syndrome and dementia;
dedicated funding to build infrastructure for national data collection.
□ an expansion of psycho-geriatric units (PGUs) has been funded by the Commonwealth. This will
follow a review of the operation of current projects. The expansion of PGUs on a national basis
using a consistent behaviour advisory model and focusing on meeting the needs of staff working with people with challenging behaviours would form a useful part of the overall service network.
4.3.10
Residential care
Recommendation 10: Residential dementia care remains problematic. In general, the principles of
ageing in place and including dementia care within mainstream aged care are desirable, however the
mechanisms for addressing identified constraints need to be addressed within the context of the current Pricing Review. Priorities include to:
□ incorporate behavioural and environmental recommendations in Aged Care Assessment Team
(ACAT) assessments, so that people with dementia and the nature and stage of that dementia are identifiable;
□ revise the Resident Classification Scale descriptors to accord better with ACAT assessments,
reflecting behavioural and environmental care needs as well as nursing and personal care needs,
so that people with dementia and the nature and stage of that dementia are identifiable;
□ in the context of the federal Review, and in close consultation with providers and other key
stakeholders, review and make recommendations to implement changes to subsidies and possibly
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
accommodation bonds and other funding vehicles in ways that remove the disincentives to provision
of quality dementia residential care, in particular addressing:
o capital constraints to high care facilities for people with dementia, including with BPSD; and
o recurrent funding constraints to low-care facilities for people with dementia/BPSD.
□ joint review by government, providers and stakeholders of the long term capital requirements for
new dementia facilities based on better models of dementia care, with consideration of a full range of finance vehicles including insurance mechanisms;
□ change the residential care planning guidelines to ensure that all facilities have the capacity to care
for people with dementia and that at least 10% of residential care places are dementia specific for
those with special support needs;
□ assess supply and demand factors driving growth in overall numbers of places and ensure that
supply growth is adequate and sustainable to meet demand growth over the longer term;
□ promote and fund new aged care facilities built on the cluster campus model on a provider-
government partnership basis;
□ extend the number and diversity of newer models of quality care to help residents with dementia,
with ongoing cost-benefit evaluation in particular in relation to quality of life;
□ increase ongoing nursing training in dementia-specific and quality person-centred care principles,
ensuring that all residential care staff have completed formalised competency based training at the Certificate III level in Aged Care, and understand the needs of people with dementia and how that
impacts on service delivery;
□ increase specialist geriatrician input into diagnosis, management and training; □ introduce government support for the cost of staff training in facilities with limited financial resources
or whose ability to provide staff training is otherwise constrained;
□ ensure guidelines are developed that identify appropriate staff to resident numbers linked to
dependency that address understaffing;
□ tighter accreditation and monitoring of standards to promote quality care, with restrictions placed on
chemical and physical restraint practices;
□ review of nursing and personal care worker remuneration; □ improved access to specialist behaviour advisory services; □ greater access to care for people with dementia with serious psychiatric symptoms, as well as those
with serious mental health problems who develop dementia.
4.3.11
Cross-cutting issues
Recommendation 11: Issues that cut across all aspects of dementia care, reflecting the different
needs of different groups of people, and that require intervention include:
□ improved access to community, residential and medical services for people with younger onset
dementia, including separate strategic planning to meet their specific needs outside the aged care
□ improved access for people with dementia and their families and carers who are from culturally and
linguistically diverse backgrounds, including improved assessment tools;
□ improved access to services for indigenous Australians living with dementia; □ greater public efforts to destigmatise dementia; and
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ smarter use of new information technologies in delivering services, particularly to people in rural and
remote areas, including cost-benefit studies of information technology instruments such as web-based information resources and messaging, moderated chats and forums, videoconferencing and
clinical communications.
4.3.12
Health financing
Recommendation 12: Intergenerational planning needs to acknowledge the need for health, aged and
dementia care spending to grow in real and relative terms, with strategies for successfully managing the
change. Various tiers of government are already taking steps in this direction. Action-oriented planning,
integrally involving stakeholders, needs to address:
□ appropriate savings or insurance schemes to provide for future health, ageing and dementia needs,
including consideration of quarantined increases in the Superannuation Guarantee levy;
□ consensus on and planning for the future private-public mix of care provision and of insurance
provision.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
METHODOLOGY
Prevalence
The prevalence estimates are obtained from two data sources, a special data request from the
Australian Bureau of Statistics Survey of Disability Ageing and Carers together with international meta-analyses from which Professor Anthony Jorm98 and others have derived previous Australian prevalence
estimates. There are weaknesses with both data sets. The ABS data are likely to contain considerable under-statement of prevalence, as it is a household survey (including ‘establishments') that relies on
self-reporting (including by others in the family) and therefore is likely to have downward bias in reporting dementia, particularly in single-person households. It does, however, contain data across all
demographic groups and regions with no a priori reason why there would be more bias in one group compared to another. Indeed, both 1993 and 1998 data were purchased to confirm the integrity of the
demographic splits (see Table 3, Section 1.3.2). The international (Jorm) data provides a much better estimation of total prevalence, which is quite robust for age cohorts over 60 worldwide. Its limitations are that it does not reflect the gender
breakdown and does not comment on prevalence for people under 60. The two data sets were reconciled by applying the demographic splits of the DAC Survey to the overall prevalence estimates of
the international data. The estimates for 2002 were thus based on the prevalence rates per 1000 for each demographic cohort projected to the estimated population in each cohort in 2002, as per ABS
(2000). The prevalence estimates will be conservative as they will not capture people whose dementia has not been diagnosed.
Projecting prevalence to 2051 (Section 1.3.3) to derive the function in Chart 5 was achieved by applying
the prevalence rates for each of the demographic cohorts to the cohorts as projected by the ABS for 2011, 2021, 2031, 2041 and 2051 (Series II, ABS, 2000), fitted with a smoothed curve. Once again the
prevalence estimate may be conservative as diagnoses may occur earlier in the future, in line with the current trend.
Disability and socio-economic impacts
Section 1.4.1 uses the International Classification of Impairments, Disabilities and Handicaps 1980 as a
framework to identify whether a person has a disability and the associated level of restriction. People in
the 1998 DAC Survey were defined as having a disability if they had one or more of the following impairments that had lasted, or were likely to last, for a period of six months or more:
□ loss of sight (not corrected by wearing glasses or contact lenses); □ loss of hearing, that restricted communication or resulted in the use of an aid; □ speech difficulties in preferred language; □ chronic or recurring pain, that restricted everyday activities; □ breathing difficulties, that restricted everyday activities; □ blackouts, fits, or loss of consciousness; □ slowness at learning or understanding; □ incomplete use of arms or fingers; □ difficulty gripping or holding things; □ incomplete use of feet or legs; □ a nervous or emotional condition that restricted everyday activities; □ a restriction in physical activities or in doing physical work;
98 Director, Centre for Mental Health Research, Australian National University
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
□ a disfigurement or deformity; □ need for help or supervision due to a mental illness; □ long-term effects of head injury, stroke or any other brain damage; □ treatment or medication for another long-term condition or ailment, and still □ restricted in everyday activities; □ any other long-term condition resulting in a restriction in everyday activities.
The flow-chart below shows how the population is subsequently categorised, with 3.61 million Australians in 1998 having a disability, including 98.5% of people with dementia almost all of whom
have specific restrictions, and so on as per Table 4.
With core activity
restriction 2 828 000
Without specific
Without disability
With schooling or
(a) Includes 1,332,500 persons with core activity restrictions.
The ABS included all people who reported having either dementia or Alzheimer's, regardless of other
conditions; if someone reported having both conditions, they are only counted once. For the rural-urban comparisons in Table 6, unfortunately data were not available by RRMA group – only the geographic
‘section of state' classification. For further descriptions of the ABS methodology see ABS (1999).
Direct health system costs
Direct health system costs can be estimated in one of two ways—the ‘bottom up' approach, calculated
by adding actual (or imputed) costs for a representative cohort of patients, or the ‘top-down' approach, which attributes total health expenditures to disease based on available information on the mix of
diseases treated and the costs of treatment. While the former is sometimes more accurate in giving up-to-the-minute estimates for specific diseases, there can be problems in obtaining representative
samples and representative cost patterns, and the advantage of the latter approach is that there will be consistency of coverage and estimates across diseases, which is more helpful for policy makers.
In this study, the top-down approach is adopted, based on the methodology developed by the Australian
Institute of Health and Welfare (AIHW), in collaboration with the National Centre for Health Program Evaluation (NCHPE) for the Disease Costs and Impact Study (DCIS). This major study measures health
services utilisation and expenditure for specific diseases and disease groups in Australia, in accordance with the Ninth Revision of the International Classification of Disease (ICD-9) published by the World
Health Organisation (WHO). The DCIS methodology has been gradually refined to estimate direct costs of hospitals, GP and specialist medical services, allied professionals, pharmaceuticals, nursing homes,
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
research and other costs (such as administration), primarily from hospital morbidity data, case mix data
and the National Health Survey (NHS), as well as other sources. DCIS methodology is detailed in Mathers et al (1998), while results are provided in Mathers and Penm (1999).
As noted in Section 2.1 (Table 9), the direct health system costs were estimated by the AIHW in 1993-
94 as $714 million. However, this is almost certainly an under-estimate in that only 17 per cent of nursing home costs were attributed to dementia although at least 60% of residents in nursing homes
have this condition. The AIHW is currently in the process of reviewing their costings and new estimates are expected in mid-2003. In this paper, the conservative 1993-94 figures were used as a base for
projections to 2002. However, the nursing home component was adjusted by a factor of 2.2 to take account of the AIHW's initial substantial under-estimation and to correlate better with expected average
costs per resident as provided from other sources. The additional breakdown provided in Table 10 was obtained through a special data request from the AIHW.
Cost projections to 2011 were based on prevalence changes due to demographic ageing (30.2%)
together with projected growth in the Health and Community Services GDP deflator. The average growth in this deflator over 1993-94 to 2000-01 was 3.8% per annum. The growth projected in the
deflator over 2002 to 2011 was 39.8%, resulting in overall growth of 82%. To this, an adjustment was made to reflect recent large institutional changes, such as the introduction of the three cholinesterase
inhibitors on the PBS, as well as highly desirable changes, such as higher levels of research expenditure and spending on primary care (GP education, training and remuneration). The total value of
all these factors was only $69.8m, however – quite small although representing significant growth (an additional 67% over the decade) from a low base for these three items. There are still considerable
upside and downside risks – even small percentage changes in the RAC component would change the projection considerably. RAC costs could go down if, for example, pharmacotherapy is effectively
administered or could go up if, for example, there are substantial injections to the RAC subsidy or capital costs. Similarly, hospital costs may be lower if waiting times into residential care are reduced,
while technological change – always the rogue variable, could either greatly increase or greatly reduce the totals.
Home and community care costs
These were not included in direct costs for historical reasons, although they are very similar in nature. In
the 1993-94 AIHW data, nursing homes were part of ‘health' expenditures (see Mathers et al, 1999, p6) whereas ‘community and public health' programs had only just begun to emerge and were considered
more part of ‘aged care' expenditure. Today the distinction seems less appropriate but is adhered to on the basis of tradition, and for comparability with most other health spending analyses, which generally
do not include home and community care costs.
Indirect costs
The World Health organisation and cost of illness studies in the past have typically classed indirect
costs as all those costs that are not direct health system costs, the approach adopted here (except for
the special case of home and community care). More recently, there is a trend to separately identify costs that are borne by government as opposed to costs to individuals or society. While this distinction
is not made in this paper (except in the scenario modelling) it can be derived from the analysis. However, the economic distinction between real and transfer costs is made, where real costs represent
real goods and services whereas transfer costs simply represent money that is transferred from one income unit to another. Transfer costs are interesting in terms of the overall government budget
composition. Measurement of indirect costs remains a matter of some debate and controversy.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Lost earnings and production (‘human capital'): This focuses on the loss of production or earnings
associated with illness and premature death. The higher end of such estimates includes absenteeism
costs plus the discounted stream of lifetime earnings lost. The lower end might include only the ‘friction' period until the worker can be replaced, which would be highly dependent on labour market conditions
and un(der)employment levels. The intermediate approach adopted in this paper comprises the lost production of one period due to exit from the workforce and absenteeism. In this case, it is reasonably
assumed that, in the absence of illness, people with dementia would participate in the labour force and obtain employment at the same rate as other Australians, and earn the same average weekly earnings
(based on ABS Average Weekly Earnings AWE 6302.0 August, released 14 November 2002) of $696 per week, including full and part time earnings across all occupations and regions. The implicit and
realistic economic assumption is that the numbers of such people would not be of sufficient magnitude to substantially influence the overall clearing of the labour market. The estimate of 5% absenteeism for
people with dementia is based on costings and data from Access Economics (2002).
Mortality burden: The mortality burden makes similar assumptions to those above if, in the absence of
the illness, those people with the illness did not die in 2002 but rather were well and participated in the
labour force similarly to average Australians, and for the same expected duration. The average age at death of 15-74 year olds with dementia (64.2 years) is derived from the demographic profile of
dementia, together with the assumption that an insignificant proportion would work after age 75. The discount rate for the net present value (NPV) of the future income stream – 0.81% – is based on the 30-
year average growth of real AWE (with the Consumer Price Index as the deflator) for the period 1981-82 to 2011-12, including forecasts from the Access Economics Macroeconomic Model. A long-term
average is required due to the sensitivity of the results to the discount rate. Then: NPV = ΣY(1+r)i = $0.22m where Y=$36,282, r=0.81% and i=0,1,2…6 The number of people who died (463) is then multiplied by the employment rate (8.5%) to give the number of people (39) who died who would, if they were alive and well, have been employed. Overall,
39*$0.22m = $8.8m, the mortality burden. Under-estimation derives from the official mortality rate – for over 162,000 Australians with dementia and average life expectancy of 8 years, one would expect a priori that the number of deaths would be
closer to 20,000 than 5,000 in 2002 as extrapolated from the 1996 AIHW data. However, the conservative approach was adopted and the official estimate used.
Potential tax revenue foregone: People with dementia or their families and carers who work less or
retire early will not only forego income, but will also pay less personal income tax. The income tax
foregone is a product of the average personal income tax rate and the foregone income. With dementia and lower income, there will be less consumption of goods and services, estimated up to the level of the
disability pension. Without dementia, it is conservatively assumed that consumption would comprise 90% of income (the savings rate may well be lower than this). The indirect tax foregone is a product of
the foregone consumption and the average indirect tax rate. Average tax rates (2002) as shown in Table 13 are derived from the AE macroeconomic model incorporating changes from A New Tax System from
1 July 2000. Tax revenue sacrificed is included as a transfer payment (not a real economic cost).
Family carer costs: Placing a value on the cost of unpaid family care is the one of the most difficult
aspects of disease costing. It is nonetheless a hugely important indirect cost, and becoming more so as,
in Australia, we increasingly accommodate people with disabilities and frail aged people in the community.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
There are three potential methods of estimating the cost or value of families and carers: 1. an opportunity cost approach – the value of the work (earnings) and/or leisure they sacrifice
(possibly also including the health and emotional wellbeing that they sacrifice);
2. the replacement cost approach – what the government would have to pay if a family carer were
3. what family carers themselves feel they should be paid (eg, as in the O'shea 2000 Irish study, which
interestingly provided an estimate of only £2 to £4 per hour).
There is no data on the latter in Australia. Moreover, a comprehensive "bottom-up" opportunity
assessment of carer costs in Australia would also require additional detailed survey work to assess care needs of all levels and types of people with dementia, as well as resolving the contentious issue of
valuing lost employment and leisure (particularly when many families and carers are retired). Hence the replacement cost approach has been adopted here, taken as the cost of outsourcing the equivalent care
hours at standard remuneration rates for care workers. The calculation using the replacement cost methodology to derive the total carer costs is detailed in section 2.2.2.
Social welfare payments: The disability pension, sickness benefits and various allowances paid to
those suffering from disease are costs to the tax-paying community, which could be put to alternative
use. These are also income transfer payments rather than real economic costs, but again relevant to the public financial position. The Disability Support Pension is the main item here for dementia – this
pension was previously known as the invalid pension and was introduced in 1910 as a result of the Invalid and Old-age Pensions Act 1908.
The weighted average payment per week in Table 17 is derived from the Centrelink website
(www.centrelink.gov.au) for each of the various payments, with weights split equally between singles and couples and between the various categories of Rent Assistance. The number of people receiving
DSP and pharmaceutical allowance (4,653) is the total number of people with dementia under 65 (6,635) multiplied by the number estimated to be in the lowest two income quintiles (70.2% from
Table 5). The people eligible for Rent Assistance is assumed to be only 30% of these (1,396), assuming 70% average home ownership Australia-wide.
Modifications and aids: Since these are also not included in the AIHW 1993-94 data, and can be quite
substantial, they were included in these costings utilising the Frisch (2001) data, as detailed in Section 2.2.4 and Table 18.
Burden of disease
In recent years, the World Health Organisation (WHO), the World Bank and Harvard University have
developed a methodology that provides a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020 (Murray and Lopez, 1996). This
approach has been adopted and applied in Australia by the AIHW with a separate comprehensive study in Victoria.
Mathers, Vos and Stevenson (1999) estimate the burden of disease for dementia in 1996 in Annex
Tables F, G and H. The YLD, YLL and total DALY elements were then extrapolated to 2002 on the basis of projected growth in the prevalence of dementia over the period. The disability weights used by the
AIHW team were 0.270 for mild dementia, 0.630 for moderate dementia and 0.940 for severe dementia.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
BRODATY TRIANGLE
SEVERITY vs TYPES OF CARE FOR PATIENTS WITH BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA
See Brodaty, Draper and Low (2003).
Description
Tiers 2-7 percentage and
Level of Disturbance & Intervention Use Cumulative
number of the estimated
162,000 people with dementia
Strategies to prevent dementia remain unproven, although some evidence exists for the protective effects of Vitamin E, Vitamin C,
statins, antacids, low cholesterol, hormone replacement therapy, education, increased social, mental and physical activities, treatment of vascular risk factors and prevention of hypertension.
Interventions not widely researched. Medications slowing progression of dementia may also prevent emergence of BPSD. For example
galantamine has been shown to lower rate of emergence of BPSD. There is evidence that environmental modifications, higher staff
ratios and staff training, may prevent emergence. Early intervention programs for dementia such as Living with Memory Loss program
run by the Alzheimer's Associations may also prove effective.
Night time disturbance, wandering, mild depression, apathy, repetitive questioning, shadowing. Management through caregiver, staff
and general practitioner education, environmental modifications, general activity programs e.g. education of caregivers, multi-sensory
stimulation; abilities-focused program; enhanced nursing home environment; education & environmental modifications; client centred
care; visual barriers; activities, medication guidelines & educational rounds.
Major depression, verbal aggression, psychosis, sexual disinhibition, wandering. Management through psychogeriatric consultation –
medications, behavioural management, e.g. physical activity programme; individualised Music; stimulated presence; behavioural
management techniques; bright light therapy; outdoor environments; increased environmental quality; Alzheimer's Australia South
Australia's hotline for BPSD.
Severe depression, psychosis, screaming, severe agitation. Management in dementia specific nursing homes or by psychogeriatric
team e.g. dementia special care units; individually tailored psychogeriatric management.
Physically aggressive, severely depressed, suicidal. Management in psychogeriatric or neurobehavioural units e.g. CADE units;
psychiatric hospitalisation.
Physically violent. Management in Intensive Specialist Care Unit.
Please note Tiers 2-7 only included in the estimated 162,000 people with dementia in Australia in 2002 + In 2002 there are approximately 2.5 million people aged 65 years and over in Australia and some 162,000 of them have some form of dementia. People with dementia represent 6.6 percent
of this population.
*Statistics based on clinical observations
♣ Statistics based on Lyketsos et al (2000).
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
GLOSSARY OF COMMON ABBREVIATIONS
Aβ beta-amyloid ABS
Australian Bureau of Statistics
Aged Care Assessment Team (in Victoria: ACAS – Aged Care Assessment Service)
AD Alzheimer's Disease ADAS-Cog Alzheimer's Disease Assessment Scale – cognitive subscale ADL
activities of daily living
Australian Institute of Health and Welfare
average length of stay
amyloid precursor protein
Behavioural and Psychological (Signs and) Symptoms of Dementia
Community Aged Care Packages
Cognitive Dementia and memory Services
cholinesterase inhibitor
Carer Education and Workforce Training (project)
Community Options Projects
Clinical Practice Improvement (study) or Consumer Price Index (context-dependent)
CT computed tomography DAC
(ABS Survey of) Disability Ageing and Carers
disability adjusted life year
Education Support Program
Department of Health and Ageing
dementia with Lewy bodies
diagnostic and statistical manual – version four
Extended Aged Care in the Home
Enhanced Primary Care
Early Stage Dementia Support and Respite Program
extra service provider
EU European Union FTD
fronto-temporal (lobe) dementia
fiscal (financial) year (1 July to 30 June)
gross domestic product
general practitioner
General Practitioner Assessment of Cognition
Home and Community Care (program)
ICD-10 International Classification of Diseases – tenth revision IT information
mild cognitive impairment
mini-mental state examination
magnetic resonance imaging
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
National Action Plan for Dementia Care
National Dementia Behaviour Advisory Service
nerve growth factor
National Health Survey
National Respite for Carers Program
National Residential Dementia Training Initiative
NSAID non-steroidal
anti-inflammatory
Personal Care Assessment Instrument (pre-1997)
positron emission tomography
psycho-geriatric (care) units
private health insurance
residential aged care
Resident Classification Instrument (pre-1997)
Resident Classification Scale
UK United Kingdom US
United States of America
vascular dementia
years of healthy life lost due to disability
years of life lost due to premature death
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
REFERENCES
Access Economics (2002) Schizophrenia Costs: An Analysis of the burden of schizophrenia and related
suicide in Australia, Report for SANE Australia, July 2002. Aged and Community Services Australia (2001) Response to Two Year Review of Aged Care Reforms,
available on www.anheca.com.au/pdf/joint_response_8_01.PDF Ajmani D (2002) "Using Shunt Technology to treat Alzheimer's Disease" Frost and Sullivan, available on
www.medicaldevices.frost.com Alistair et al (2002) "Sensory stimulation in dementia: an effective option for managing behavioural problems"
British Medical Journal 325 (7376): 1312-1313. Allen, J (2002) "Shunt shows promise against Alzheimer's" Los Angeles Times, 24 December 2002 available
on www.post-gazette.com/healthscience Alzheimer Europe (2002) Newsletter, Autumn 2002. Alzheimer's Australia (2003) "Quality Dementia Care" Position paper, January 2003. Alzheimer's Australia (2002a) "About Non-steroidal Anti-Inflammatory Drugs" Factsheet, September 2002. Alzheimer's Australia (2002b) "Aluminium and Alzheimer's Disease" Update sheet, October 2002. Alzheimer's Australia (2001a) "Please remember this" Educational booklet, August 2001. Alzheimer's Australia (2001b) "Drug Treatments for Alzheimer's disease currently licensed in Australia" and
"Subsidies for Aricept, Exelon and Reminyl: What are the conditions?" Update sheets, October 2001. Alzheimer's Association of the United States (2002a) ‘Neuroscientists Gather for World's Largest Alzheimer
Research Conference', Conference Highlights from Stockholm July 2002, on www.alz.org Alzheimer's Association of the United States (2002b) "Alzheimer's Disease Costs Businesses $61 billion a
year in caregiver time, productivity loss and medical expenses, study shows", Media Release, 27 June 2002,
on www.alz.org Alzheimer's Association of the United States (2002c) "Statistics about Alzheimer's Disease", on www.alz.org Australian Bureau of Statistics (2002) National Health Survey 2001: Summary of Results, Cat No 4364.0,
October. Australian Bureau of Statistics (2000) Population Projections Australia: 1999 to 2101, Cat No 3222.0, August
2000. Australian Bureau of Statistics (1999) Survey of Disability Ageing and Carers: Australia, Summary of
Findings, Catalogue No. 4430.0, April 1999. Australian Bureau of Statistics (1997) National Health Survey 1995: Summary of Results, Cat No 4364.0,
August 1997. Australian Institute of Health and Welfare (2002a) Older Australia at a glance, third edition, AIHW Cat No
AGE 25, Canberra. Australian Institute of Health and Welfare (2002b) Mental Health Services in Australia 1999-00, AIHW Cat
No HSE-19, Canberra. Australian Institute of Health and Welfare (2002c) Entry period for residential aged care, AIHW Cat No AGE
24, Canberra. Barclay L (2002) "Low-Flow CSF Shunt Tested in Alzheimer's Disease" Medscape Medical News available
on www.medscape.com Bayley J (1998), Iris: A Memoir of Iris Murdoch, Duckworth Press, London UK.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Bird M and Parslow R (2001) Future Directions: Consultancy report to the Alzheimer's Association of
Australia, Australian National University, Canberra, July 2001. Birks J, Melzer D, Beppu H (2003) "Donepezil for mild and moderate Alzheimer's disease" 2003 Cochrane
Library see www.cochrane.org/cochrane/revabstr/ab001190.htm Birks J, Grimley Evans J, Iakovidou V, Tsolaki M (2003) "Rivastigmine for Alzheimer's disease" 2003
Cochrane Library see www.cochrane.org/cochrane/revabstr/ab001191.htm Black K, LoGiudice D, Ames D, Barber B, Smith R (2001) Diagnosing Dementia: a reference paper,
Alzheimer's Australia, September 2001. Blackmun S (1998) "Is It Depression or Is It Dementia?" Psychiatric Times, Vol. XV Issue 2, February 1998. Boden C (1998) Who will I be when I die? Harper Collins Publishers, Sydney Australia. Brodaty H, Draper B and Low L-F (2003) "Behavioural and psychological symptoms of dementia: a seven-
tiered model of service delivery" MJA, 178, 231-235 Broe, A (2002) Population Ageing, Human Lifespan and Neurodegenerative disorders: a fifth epidemiological
transition, Swets and Zeitlinger Publishers, US, July 2002. Burns A (2001) "Dementia" Factsheet for Personal Social Services Research Unit, North West Dementia
Centre, University of Manchester, NHS Executive North West, UK. Carers Australia (2001) "A Fair Go for Australia's Carers" Federal election platform paper, November 2001,
available on www.carers.asn.au. Chapman P (2000) "Alzheimer's disease: model behaviour", Nature, 408(6815), 915-916. Christen Y (2000) "Oxidative stress and Alzheimer disease" Am J Clin Nutr 71(2), 621S-629S. Continence Foundation of Australia (2000), "Towards an equitable subsidy scheme for continence products"
Position Paper, Sub Committee for Continence Products, November 2000. Creasey H and Brodaty H (1998) "New Hope for Early Diagnosis: Research Briefs" Intouch, Alzheimer's
Association of NSW, Issue 27, Summer 1998. Cummings J (2001) "Treatment of Alzheimer's disease" Clin. Cornerstone 3(4), 27-39. Cuthbertson S, Lindsay-Smith E and Rosewarne R (1998) "Review of the Resident Classification Scale"
Aged and Community Care Service Development and Evaluation Report No.36, Commonwealth Department
of Health and Family Services, Canberra, July 1998. Department of Health and Ageing (2002a) Aged Care in Australia, August 2002, available on
www.health.gov.au Department of Health and Ageing (2002b) Report of the Working Group on Dementia Specific Aged Care,
Draft, September 2002 available on http://www.health.gov.au/acc/rescare/acprtask/sub4_acwg.pdf Fillit HM (2002) "The role of Hormone Replacement Therapy in the prevention of Alzheimer's disease",
Archives of Internal Medicine, 162, 1934-1942. Fratiglioni L, Ahlbom A, Viitanen M and Winblad B (1993) "Risk factors for late onset Alzheimer's disease: a
population-based case-control study", Ann Neurol 33, 258-266. Freeth S (1994) The Young Mind: Issues in Relation to Young People with Dementia, Alzheimer's Australia. Frisch J (2001) Towards a Disability Allowance: Offsetting the Costs of Disability - An Analysis, Prepared for
the Physical Disability Council of Australia, June 2001. Galasko D, Edland S, Morris J, Clark C, Mohs R and Koss E (1995) "The Consortium to Establish a Registry
for Alzheimer's Disease (CERAD), Part XI, Clinical Milestones in patients with Alzheimer's disease followed
over three years", Neurology, 45, 1451-1455.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Gibson D, Benham C and Racic L eds. (1999) Older Australia at a glance, Australian Institute of Health and
Welfare, Cat No AGE 12. Gray L (2001) Two Year Review of Aged Care Reforms: Final report available on
www.health.gov.au/acc/2yr_rvw Grobe-Einsler, R. (1993) "Clinical aspects of nimodipine" Clin. Neuropharmacol, 16(Suppl. 1), S39-45. Gustilo M, Markowska A et al (1999) "Evidence that nerve growth factor influences recent memory through
structural changes in septohippocampal cholinergic neurons", J. Comp. Neurol. 405(4): 491-507. Gutterman E, Markowitz J, Lewis B and Fillit H (1999) "Cost of Alzheimer's Disease and Related Dementia
in Managed-Medicare", Journ Am Geriatr Soc, 47, 1065 –1071. Hampson A with Jurd E (2000) Take Me Home: families living with Alzheimer's, Rezolv in Print, NSW. Hatfield M, Sonnenschein F and Rosenberg L (2000) "Exceptional Returns: The Economic Value of
America's Investment in Medical Research", Funding First available through www.fundingfirst.org Harvey (1998) Young Onset Dementia: Epidemiology, clinical symptoms, family burden, support and
outcome, Dementia Research Group & National Health Service Executive, UK, on
www.dementia.ion.ucl.ac.uk Henderson A and Jorm A (1998) Dementia in Australia, Aged and Community Care Service Development
and Evaluation Report No 35, Canberra AGPS. Horn S (2002) "Implications of restrictive drug practices" Presentation paper, 20 February 2002. International Psychogeriatric Association (2001) "Availability and subsidy of ant-dementia drugs around the
world in mid-2001: a special report from the assistance editors" IPA Bulletin, 18:4, December 2001. Jorm A (2002) "Prospects for the prevention of dementia", Australasian Journal on Ageing, 21:1, March
2002. Jorm A (2001) "Dementia: a major health problem for Australia", Position Paper 1, September 2001,
available from Alzheimer's Australia. Jorm A, Griffiths K, Christensen H and Medway J (2001) Research priorities in mental health, Mental Health
and Special Programs Branch, Commonwealth Department of Health and Aged Care, Canberra. Kitwood T (1997) Dementia Reconsidered: The Person Comes First Open University Press: Milton Keynes,
UK. Kleinke J (2001) "The price of progress: Prescription drugs in the health care market" Health Affairs,
20(5):43-60. Kleinke J (2000) "Just what the HMO ordered: the paradox of increasing drug costs" Health Af airs, 19(2):
78-91. Knopman d, Schneider L, Davis K et al (1996) "Long term tacrine (Cognex) treatment: effects on nursing
home placement and mortality" Neurology, 47:166-77. Kukull W, Larson E, Bowen J, McCormick W, Teri L, Pfanschmidt M, Thompson J, OMeara E, Brenner D
and van Belle G (1995), "Solvent exposure as a risk factor for Alzheimer's disease: a case control study" Am
J Epidemiol, 141, 1059-1071. Kumar AM, Tims F et al (1999) "Music therapy increases serum melatonin levels in patients with Alzheimer's
disease" Altern Ther Health Med, 5(6), 49-57. Leon J, Cheng C and Neumann P (1998) "Alzheimer's disease care: costs and potential savings" Health
Affairs 1998; 17: 206-14. Life Extension Foundation (2002) Alzheimer's Disease, available on www.lef.org.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Lopez O, Becker J, Wisniewski S, Saxton J, Jaufer D and Dekosky S (2002) "Cholinesterase inhibitor
treatment alters the natural history of Alzheimer's disease" Journal of Neurology, Neurosurgery and
Psychiatry 72: 310-314. López-Arrieta B (2002) "Nimodipine for primary degenerative, mixed and vascular dementia" The Cochrane
Library, Issue 4, 2002. Lowin A, McCrone P and Knapp M (2000) "Cost of Alzheimer's Disease and Level of Research Funding",
Centre for the Economics of Mental Health, Institute of Psychiatry, Kings College, London. Lyketsos C, Steinberg M, Tschanz J et al (2000) "Mental and behavioural disturbance in dementia; findings
from the Cache County Study on Memory in Aging", American Journal of Psychiatry 157: 708-714. Maller J and Rees G (2002) "Research Priorities: Dementia" Submission to the National Research Priorities
Taskforce, August 2002. Mathers C, Vos T and Stevenson C (1999) The burden of disease and injury in Australia, AIHW Cat No
PHE-17, Australian Institute of Health and Welfare, Canberra. Mathers C and Penm, R (1999) Health system costs of injury, poisoning and musculo-skeletal disorders in
Australia 1993-94, AIHW Cat No HWE-12, Australian Institute of Health and Welfare, Canberra. Mathers C, Stevenson C, Carter R and Penm R (1998) Disease Costing methodology used in the Disease
Costs and Impact Study 1993-94, AIHW Cat No HWE-7, Australian Institute of Health and Welfare,
Canberra. Meek P, McKeithan E et al (1998) "Economic considerations in Alzheimer's Disease" Pharmacotherapy,
18(2 Pt 2): 68s-73s. Morris J (1996) "Classification of dementia and Alzheimer's disease", Acta Neurol Scand, Suppl 165, 41-50. Muller W, Eckert G et al (1999) "Piracetam: novelty in a unique mode of action", Pharmacopsychiatry 1, 2-9. Murray C and Lopez A eds (1996) The Global Burden of Disease. Geneva, Cambridge, Mass., Washington.
Harvard School of Public Health, for WHO and The World Bank, distributed by Harvard University Press. Nishizaki T, Matsuoka T et al (2000) "Presynaptic nicotinic acetylcholine receptors as a functional target of
nefiracetam in inducing a long-lasting facilitation of hippocampal neurotransmission", Alzheimer Dis Assoc
Disord 14(Suppl. 1), S82-94. Olin J and Schneider L (2003) "Galantamine for Alzheimer's disease", 2003 Cochrane Library, see
www.cochrane.org/cochrane/revabstr/ab001747.htm O'Shea E (2000) "The costs of caring for people with dementia and related cognitive impairments" National
Council on Ageing and Older People, Centre for Ageing Studies, University of Ireland, Galway. Perrin T and May H (2000) Wellbeing in Dementia: An Occupational Approach for Therapists and Carers
Churchill Livingstone, London. Pipher, M (1999) Another Country: Navigating the Emotional Terrain of Our Elders, Random House. Pollitt P (1997) "The Problem of Dementia in Australian Aboriginal and Torres Strait Islander Communities:
An Overview" International Journal of Geriatric Psychiatry, 12:155-163. Ramamurthy B, Hook P et al (1999) "An overview of carbohydrate-protein interactions with specific reference
to myosin and ageing", Acta Physiol Scand 167(4), 327-9. Rees G (2002) "Time to plan for dementia care – the disease of the twenty-first century" National Healthcare
Journal, May 2002. Rice D, Fox P, Max W, Webber P, Lindemann D, Hauck W, Segura E (1993) "The economic burden of
Alzheimer's disease" Health Affairs 12: 165-176.
The Dementia Epidemic: Economic Impact and Positive Solutions for Australia
Rosewarne R, Opie J, Ward S (2000) "Dementia-specific care in Australia: an overview and future
directions" RPAD Vol 4: Special Care Units. Rosewarne R, Opie J, Bruce A, Ward S, Doyle C and Sach J (1997) "Care Needs of People with Dementia
and Challenging Behaviour Living in Residential Facilities" Aged and Community Care Service Development
and Evaluation Reports Nos 24, 26-31, Commonwealth Department of Health and Family Services, AGPS,
Canberra. Rotstein G (2000) "Burden of illness often heaviest for caregivers" Post-Gazette, Tuesday, December 12,
2000. Saine K, Cullum C, Martin-Cook K, Hynan L, Svetlik D and Weiner M (2002) "Comparison of functional and
cognitive donepezil effects in Alzheimer's disease" Int Psychogeriatr June 2002; 14(2): 181-5. Sherman B (1999) Dementia with Dignity: a Guide for Carers (2nd edition) McGraw Hill, Australia. Sobel E, Dunn M, Davanipour Z, Qian Z and Chui H (1996) "Elevated risk of Alzheimer's disease among
workers with likely electromagnetic field exposure" Neurology, 47, 1477-1481. Sobel E, Davanipour Z, Sulkava R, Erkinjuntti T, Wikstrom J, Henderson V, Buckwalter G, Bowman J and
Lee P-J (1995) "Occupations with exposure to electromagnetic fields: a possible risk factor for Alzheimer's
disease", Am J Epidemiol, 12 515-524. Souetre e, Thwaites R et al (1999) Economic impact of Alzheimer's disease in the United Kingdom: cost of
care and disease severity for non-institutionalised patients with Alzheimer's disease" Brit J Psychiatry, 174:
51-55. Stern Y, Gurland B, Tatemichi T, Tang M, Wilder D and Mayeux R, (1994) "Influence of education and
occupation in the incidence of Alzheimer's disease", JAMA, 271, 1004-1010. Tariska P and Paksy A (2000) "Cognitive enhancement effect of piracetam in patients with mild cognitive
impairment and dementia", Orv. Hetil. 141(22), 1189-93. Trabucchi M and Bianchetti A (2002) "Do drug treatments really change the costs of dementia?" 7th
International Geneva/Springfield Symposium on Advances in Alzheimer Therapy, 6 April 2002. University of Bradford (2001) "Dementia Care Course is UK First" Press Release 13 June on
www.bradford.ac.uk Williams P, Rands G, Orrel M, Spector A (2003) "Aspirin for vascular dementia", 2003 Cochrane Library, see
www.cochrane.org/cochrane/revabstr/ab001296.htm Wimo A, Jonsson B, Karlsson G and Winblad B (1998) Health Economics of Dementia, Wiley, UK, 1998. Zandi P, Anthony J, Hayden K, Mehta K, Mayer L and Breitner J for the Cache County Study Investigators
(2002) "Early long-term NSAID use may reduce Alzheimer's risk", Neurology, 59, 880-886.
Source: http://www.dcnet.gr.jp/retrieve/kaigai/pdf/au09_01EpidemicFullReport.pdf
t i o n a l H C o s p i t a l o U f B a h r a i Sn W.L.L Vol. 2 Issue No. 18 The Second Physician Attribute: Medical and Clinical Knowledge Medicine changes rapidly. Clinical practice and standards advance fast. We in the Hospital place great importance to the management of change. We al think that proper management of change is the
Topic: Antipsychotic and Physical Health in Dementia Paper Type: Assignment Word Count: 3450 words Pages: 14 pages Referencing Style: Harvard Referencing Educational Level: Graduate Antipsychotic and Physical Health in Dementia [Student's Name] [Name of Institution]

