E-jnc.org
CASE REPORT
online ML Comm
J Neurocrit Care 2012;5:30-32
Olanzapine-Induced Hypoglycemic Encephalopathy:
Hyo Jeong Kim, MD, Dong Wook Kim, MD, Dong Joo Yun, MD, Gun-Sei Oh, MD and Sang Hyun Jang, MD Department of Neurology, Eulji University College of Medicine, Daejeon, Korea
Antipsychotic medications are associated with increased risks of metabolic abnormalities. We present a 44-year-old woman with under-lying bipolar disorder who had been treated with atypical antipsychotics, olanzapine. After taking 50 mg olanzapine to commit suicide, she developed altered mentality. The serum glucose level was 15 mg/dL and she was treated with glucose infusion immediately. Brain MRI findings were compatible with hypoglycemic encephalopathy. Olanzapine may induce serious hypoglycemia, even in the absence of any risk factors of hypoglycemia.
J Neurocrit Care 2012;5:30-32
KEY WORDS: Hypoglycemic encephalopathy · Olanzapine · Diffusion-weighted image.
to emergency room after 8 hours. On admission, her vital signs were stable. Her body weight checked 67 kg and the
Atypical antipsychotic drugs offer important benefits to body mass index was 26.8. On neurologic examination, her
many patients with disorders such as schizophrenia, including mental state was semi-coma. Vestibulo-ocular reflex and cor-a lower risk for the extrapyramidal side effects compared to neal reflex were not shown. No other definitive upper motor conventional antipsychotics. However, certain treatments with neuron signs were observed. Her serum blood glucose levels antipsychotic medication are associated with increased risks were 15 mg/dL on admission. Intra-venous infusion of 500 for weight gain, dyslipidemia, insulin resistance, hyperglyce-
mL 50% dextrose was administered immediately, but her
mia, and hypoglycemia.1-3
mental state was not improved. Laboratory findings showed
The mechanism of these metabolic abnormalities, especial-
Hb A1c 5.3%, insulin level 2.66 μU/mL and fasting total
ly glucose metabolism is stil unclear. Mechanisms such as an-
cholesterol level was normal. Valproic acid level was 11.6
tagonism of histamine and serotonin, and increased leptin se-
μg/mL, which were lower than the therapeutic level. Blood
cretion may play a role in the lowering of serum glucose le-
gas analysis revealed no hypoxia. Some possible causes of
hypoglycemia in non-diabetic patient including hepatic, renal
We report a case of severe hypoglycemia with encephalop-
disease, infection, insulinoma, non-β-cell tumor were evalu-
athy induced by olanzapine overuse.
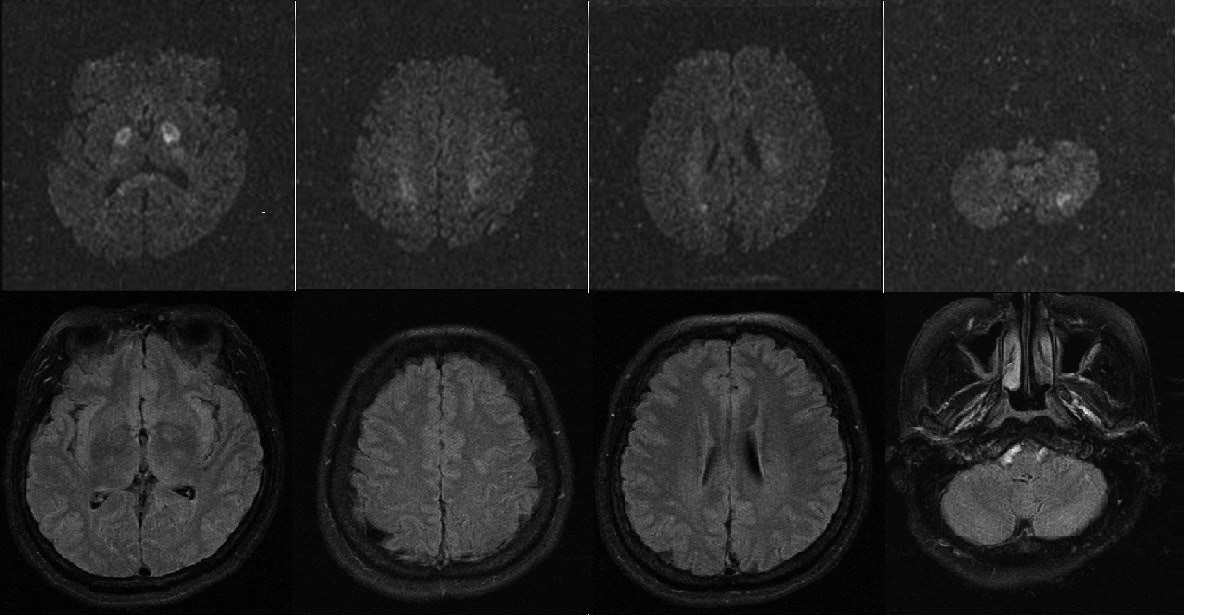
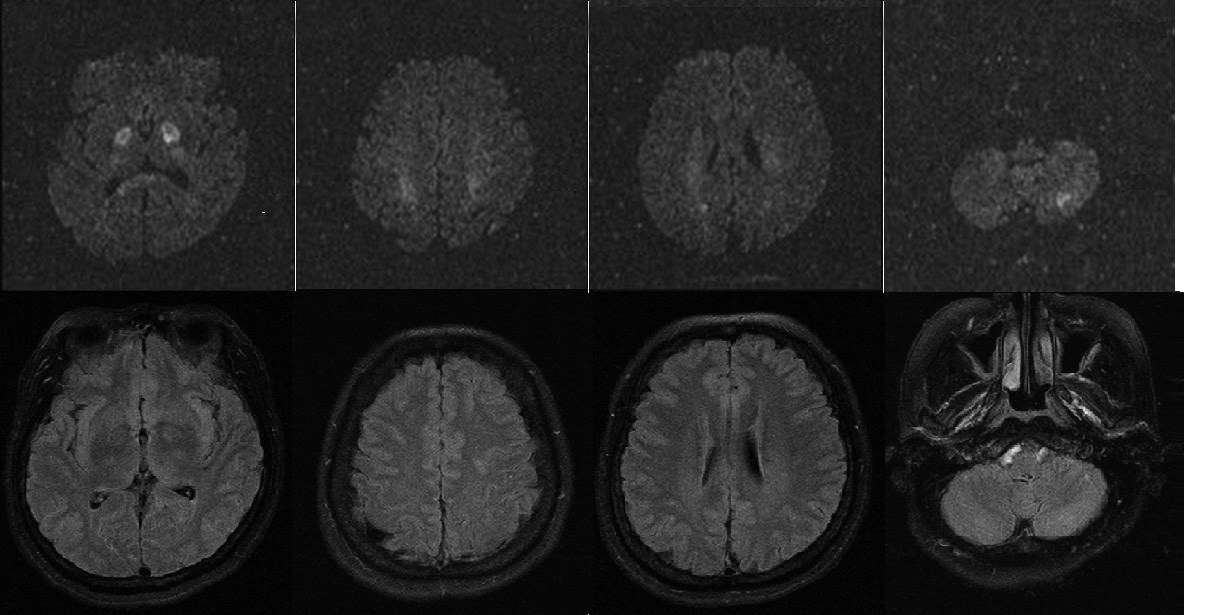
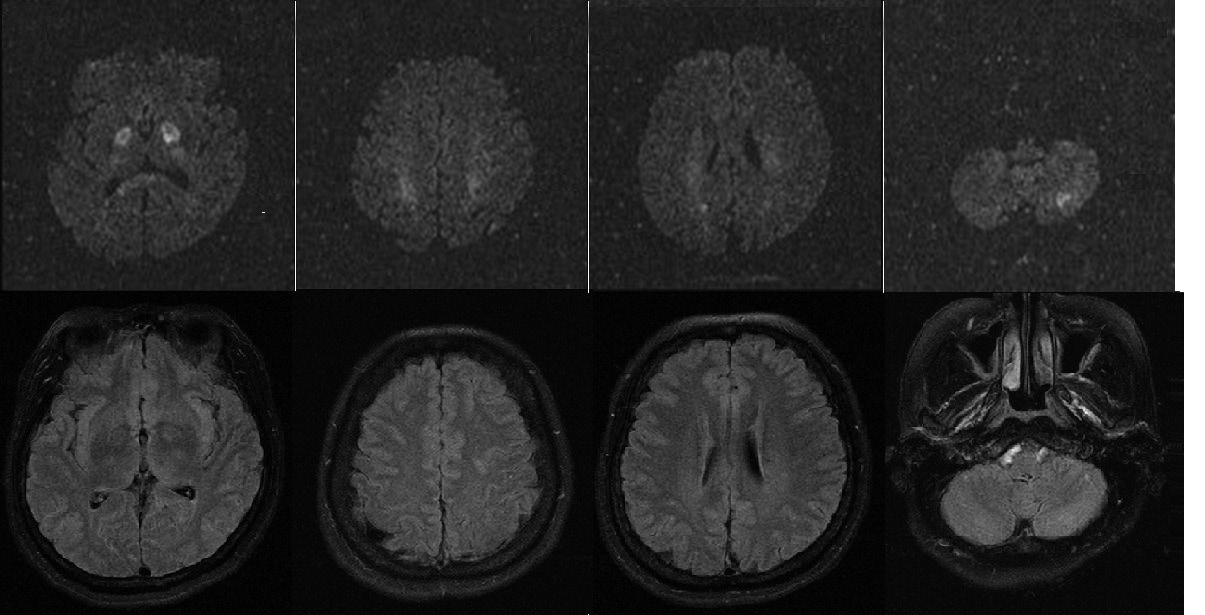
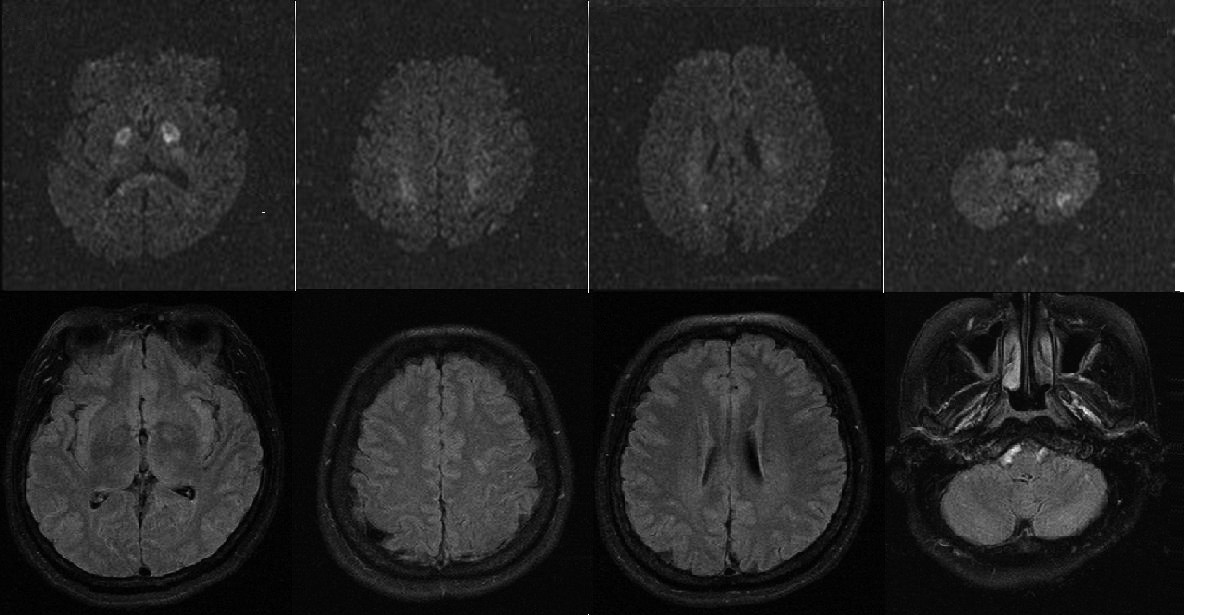
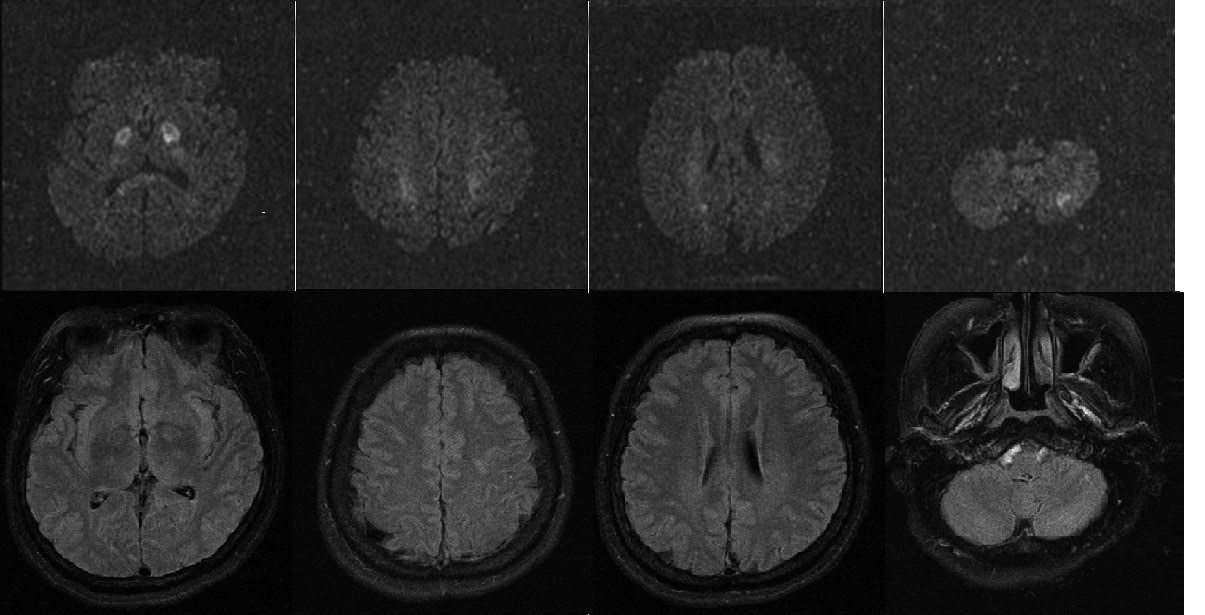
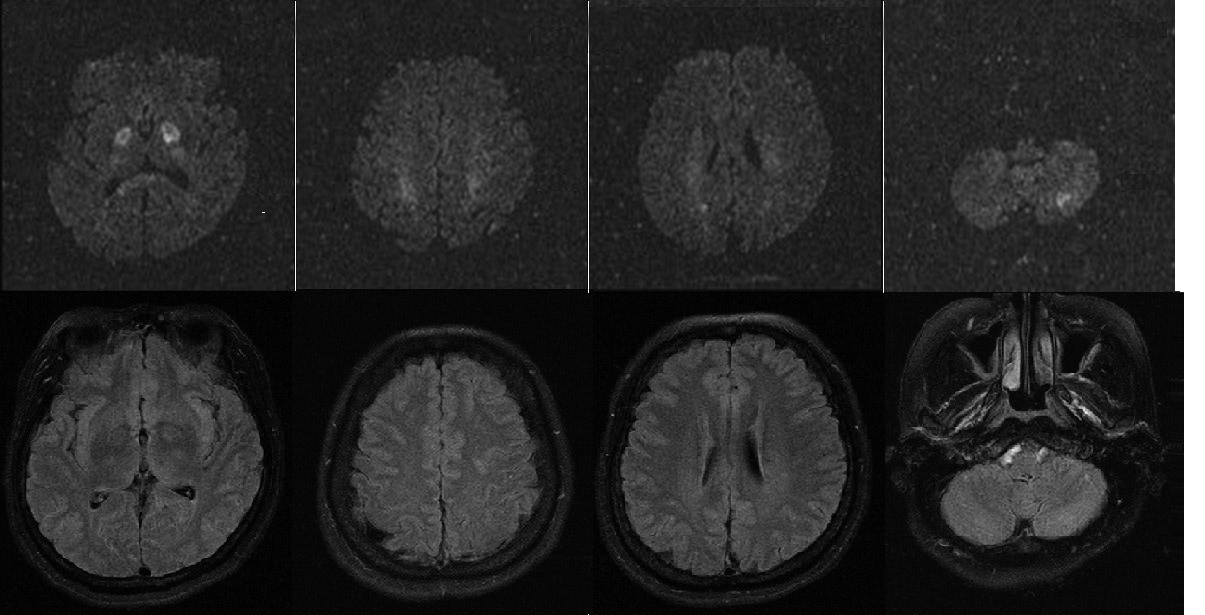
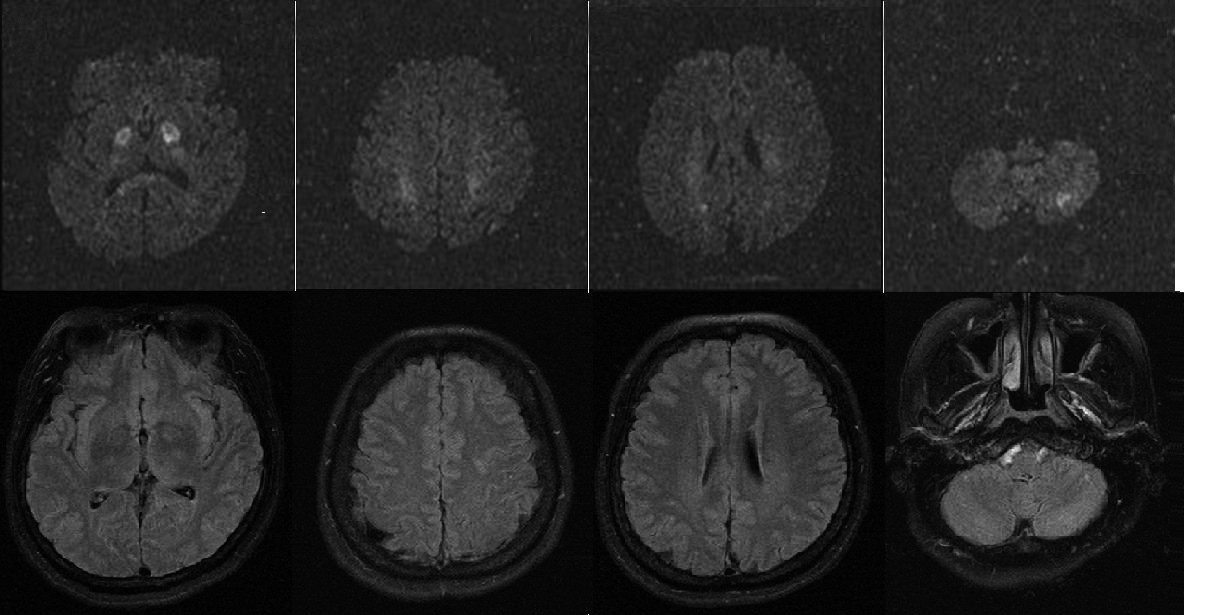
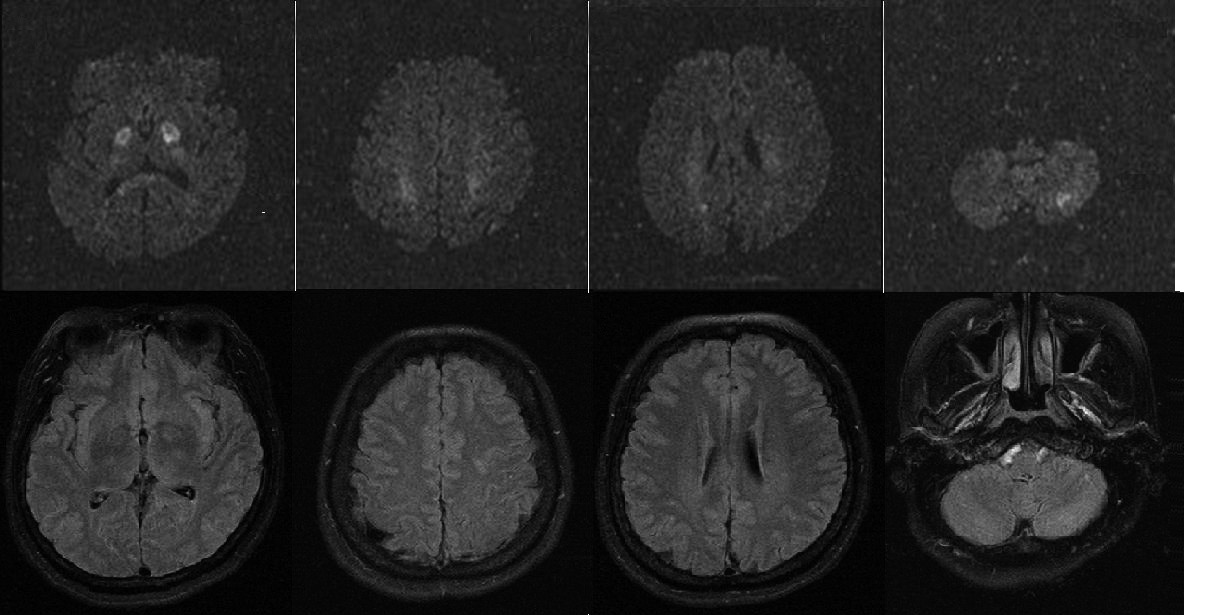
ated and the results were negative. Diffusion-weighted brain MRI (DWI) showed increased signal intensity at the bilateral
globus pallidi, fronto-parietal subcoritical white matter, cor-pus callosal splenium symmetrically, and left inferior cere-
A 44-year-old woman was admitted to our hospital due to a bellar hemisphere, but negative on fluid attenuated inversion
comatose mentality. She had previous history of bipolar dis-
recovery (FLAIR) images (Fig. 1).
order and treated with olanzapine, valproic acid for 10 years.
Electroencephalography showed nearly persistent inter-
After taking 50 mg olanzapine at once to commit suicide, mixed synchronous or independent moderate amplitude semi-she developed an impaired consciousness. She was admit ed rhythmic delta slow waves, compatible to decreased cortical
function without seizure activities.
Address for correspondence: Sang Hyun Jang, MD
On neurologic examination after the 2 days of symptoms
Department of Neurology, Eulji University Col ege of Medicine, 1306
onset, her mental status improved to drowsy. She showed brady-
Dunsan-dong, Seo-gu, Daejeon 302-799, KoreaTel: +82-42-611-3858, Fax: +82-42-611-3858
phrenia, bradykinesia and symmetric fair grade motor weak-
E-mail:
[email protected]
ness in whole extremities without other sensory abnormality,
30 Copyright 2012 The Korean Neurocritical Care Society
Olanzapine-Induced Hypoglycemic Encephalopathy ▌ HJ Kim, et al.
FIGURE 1. Initial dif usion-weighted brain MRI on admission showing hyperintense lesions in the bilateral globus pal idi, corpus cal osal
splenium (A), bilateral fronto-parietal subcoritical white mat er (B, C), and left inferior cerebel ar hemisphere (D). On fluid at enuated inver-
sion recovery images, these lesions are not shown (E-H).
etal subcoritical white matter, corpus callosum and left inferi-or cerebellar hemisphere lesions were not shown (Fig. 2).
She was discharged with no further improvement on 1
month after hospitalization.
Olanzapine is known as a common cause of hyperglycemia
and hypertriglyceridemia. Recently published randomized controlled study demonstrated that olanzapine has a relation-ship to weight gain and insulin resistance.3 It was suggested that metabolic abnormalities caused by olanzapine are relat-ed to the insulin resistance.6,7
In this patient, however, olanzapine induced hypoglycemia
and it might be related to an induced metabolic abnormality that olanzapine promote insulin resistance and excessive insu-lin secretion. In our patient, serum insulin levels were not ele-
vated during the episodes of hypoglycemia. Two possible ex-
FIGURE 2. Fol ow-up fluid at enuated inversion recovery MRI after
planations for normal serum insulin level deserve comment.
the 20 days of symptoms onset revealing hyperintense lesions in
bilateral globus pal idi, which had seen dif usion-weighted brain
First, it is possible that hypoglycemia is related to noninsulin
MRI on admission (A). The fronto-parietal subcoritical white mat er
mechanism such as antagonism of histamine and serotonin,
and left inferior cerebel ar hemisphere lesion are not shown any
and increased leptin secretion. Second, as the patient was treated with immediate infusion of glucose before sampling of
cerebellar dysfunction and abnormal movement. Her con-
serum insulin, rapid rising serum glucose level might halt in-
sciousness improved gradually and after 3 weeks on admis-
sulin secretion and lower the increased serum insulin level.
sion, her mental status became alert but bradyphrenia and bra-
Usually, even if olanzapine stimulates insulin secretion, ho-
dykinesia persisted. Follow-up brain MRI showed bilateral meostatic mechanisms act to regulate blood sugar levels and symmetric patchy high signal intensity on FLAIR images at to prevent the onset of hypoglycemia. From the perspective the globus pallidi, had seen on DWI initially. The fronto-pari-
of this patient, it might lack reserve capacity with regard to
J Neurocrit Care ▌ 2012;5:30-32
glucose homeostasis, why she developed hypoglycemia.
lin intolerance.
In the cases of hypoglycemic encephalopathy, lesions main-
ly involve the cerebral cortex, basal ganglia, hippocampus, REFERENCESsplenium, and bilateral internal capsule. The mechanisms of
1. Sander JW, Shorvon SD. Epidemiology of the epilepsies. J Neurol
cytotoxic edema are shrinkage of the extracellular space as a
Neurosurg Psychiatry 1996;61:433-43.
result of hypoglycemia, and failure of ionic pumps of neuronal
2. Sernyak MJ, Leslie DL, Alarcon RD, Losonczy MF, Rosenheck R.
Association of diabetes mellitus with use of atypical neuroleptics in
membrane, which cause hyperintense lesion on DWI.8 Some
the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
studies reported that hyperintense lesions which were detected
3. Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA,
in white matter such as corpus callosum, internal capsule, or
Perkins DO, et al. Effectiveness of antipsychotic drugs in patients
with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
corona radiata, regressed on follow-up imaging. These fea-
4. Budman CL, Gayer AI. Low blood glucose and olanzapine. Am J Psy-
tures exhibit relatively good prognosis. If lesions were detect-
ed in the cerebral cortex, basal ganglia, or hippocampus and
5. Koro CE, Fedder DO, L'Italien GJ, Weiss SS, Magder LS, Kreyenbuhl
J, et al. Assessment of independent effect of olanzapine and risperi-
did not regress on second imaging, the outcome wil be poor.8,9
done on risk of diabetes among patients with schizophrenia: population
In our patient, follow-up brain MRI showed disappeared sub-
based nested case-control study. BMJ 2002;325:243.
coritical white mat er, corpus cal osum, cerebel ar hemisphere
6. Osser DN, Najarian DM, Dufresne RL. Olanzapine increases weight
lesions, but persistent high signal intensity in the bilateral bas-
and serum triglyceride levels. J Clin Psychiatry 1999;60:767-70.
7. Nagamine T. Hypoglycemia associated with insulin hypersecretion
al ganglia. Her clinical outcome was not so good because the
following the addition of olanzapine to conventional antipsychotics.
patient was left with bradyphrenia and bradykinesia, which is
Neuropsychiatr Dis Treat 2006;2:583-5.
correlated to previous reports. Regarding above unequal vul-
8. Kang EG, Jeon SJ, Choi SS, Song CJ, Yu IK. Diffusion MR imaging
of hypoglycemic encephalopathy. AJNR Am J Neuroradiol 2010;31:
nerability, basal ganglia may be more vulnerable to oxidative
stress after glucose reperfusion because of their lesser glucose
9. Ma JH, Kim YJ, Yoo WJ, Ihn YK, Kim JY, Song HH, et al. MR imag-
transporter efficiency.10
ing of hypoglycemic encephalopathy: lesion distribution and progno-
sis prediction by diffusion-weighted imaging. Neuroradiology 2009;
Hypoglycemia is a serious medical condition which causes
neurologic damages. We should consider the metabolic effects 10. Haces ML, Montiel T, Massieu L. Selective vulnerability of brain re-when we use atypical antipsychotic drugs and monitor any hy-
gions to oxidative stress in a non-coma model of insulin-induced hy-
poglycemic symptoms, body weight, fasting glucose and insu-
Source: http://e-jnc.org/upload/pdf/jnc-5-1-30.pdf
1021-1030 20/3/06 19:21 Page 1021 INTERNATIONAL JOURNAL OF ONCOLOGY 28: 1021-1030, 2006 Cimetidine, an unexpected anti-tumor agent, and its potential for the treatment of glioblastoma (Review) FLORENCE LEFRANC1, PAUL YEATON3, JACQUES BROTCHI1 and ROBERT KISS2 1Department of Neurosurgery, Erasmus University Hospital, 2Laboratory of Toxicology,
Sept. - Oct. 2007 GSIA BI-MONTHLY NEWS BULLETIN GOA STATE INDUSTRIES ASSOCIATION (An Apex Association for Micro, Small, Medium Enterprises in Goa) ISO 9001:2000 Certified 4 FLOOR, GOA-IDC HOUSE, PATTO PLAZA, PANAJI, GOA 403 001. Office Timings: 9.30 a.m. 6.00 p.m. (Mon.-Fri.) & 9.30 a.m. 1.30 p.m. (Sat.) Ph.: 2438395 Fax: 2438210 E-mail : [email protected] Website: www.gsia.in

