Calming effects of deep touch pressure in patients with autistic disorder, college students, and animals
Calming Effects of Deep Touch Pressure in Patients with
Autistic Disorder, College Students, and Animals
TEMPLE GRANDIN, Ph.D.
Many people with autistic disorder have problems with oversensitivity to both touch andsound. The author (an autistic person) developed a device that delivers deep touch pressure to
help her learn to tolerate touching and to reduce anxiety and nervousness. The "squeeze
machine" applies lateral, inwardly directed pressure to both lateral aspects of a person's
entire body, by compressing the user between two foam-padded panels. Clinical observations
and several studies suggest that deep touch pressure is therapeutically beneficial for both
children with autistic disorder and probably children with attention-deficit hyperactivity
disorder. Only minor and occasional adverse effects have been noted. Data are reported that
show a similar calming effect in nonreferred college students. A review of the animal literature
reveals that animals have similar calming reactions, and also suggests possible additionalphysiological effects of deep touch pressure. At present, there are increasing anecdotal reports
of the clinical value of the squeeze machine, including suggestions that it can be used to reduce
required doses of psychostimulant medications. More clinical studies are needed to evaluate
the potential role of this seemingly beneficial form of "physiological" stimulation.
Certain sensory processing problems may be explained by cerebellar abnormalities. In addition to the
familiar roles of the cerebellum in motor coordination and balance, there are suggestions that the
cerebellum may also have functions in sensory processing. Early studies found that stimulation of thecerebellar vermis caused a cat to become hypersensitive to touch and to sound (Chambers 1947). More recentwork in rats also suggests that the cerebellum acts as a modulator of sensory input for various sensory
modalities, effectively functioning as a type of volume control; lobules V, VI, and VII of the vermis appear to
be the most crucial sites (Crispino and Bullock 1984).
People with autism have many sensory processing deficits, including problems in modulating sensory input
(Ornitz 1985). Most research on sensory processing problems in autistic individuals has studied the auditoryand visual modalities. It may be hypothesized that some of the sensory processing problems in autisticdisorder might be related to abnormalities of the cerebellum.
Department of Animal Science, Colorado State University, Fort Collins, CO 80523
Courchesne et al. (1988) found that a majority (14/18) of high-functioning adults with autistic disorder had
cerebellar abnormalities. Brain autopsy research has also revealed cerebellar abnormalities in autism,especially in lobules V, VI, and VII of the vermis (Bauman and Kemper 1985, Ritvo et al. 1986).
When I was age 3,1 had standard autistic symptoms such as intolerance to being touched, inability to speak,
tantrums, and Stereotypie behavior. I would stiffen and pull away when people touched me, and I wasoversensitive to both touch and sound (Grandin 1989a, Grandin and Scarino 1986) Magnetic resonance image(MRI) scans have revealed that my cerebellum is undersized, and I have a slight balance problem.
I will describe here a deep touch pressure device ("squeeze machine") that I developed to help me overcome
problems of oversensitivity to touch, and that allays my nervousness. Reactions of other people to the squeezemachine, including children with autistic disorder and attention-deficit hyperactivity disorder (ADHD) arealso reported.
Finally, the animal literature on deep touch pressure will be surveyed, revealing that similar calming
reactions may be generally observed in response to deep touch pressure in higher animals. However, in view
of the possibility that cerebellar abnormalities may cause hypersensitivity to touch, the therapeutic response ofchildren with autism to correctly applied deep touch pressure might be partially explained by a cerebellarmechanism.
CLINICAL EFFECTS OF DEEP TOUCH PRESSURE
Deep touch pressure is the type of surface pressure that is exerted in most types of firm touching, holding,
stroking, petting of animals, or swaddling. In contrast, light touch pressure is a more superficial stimulationof the skin, such as tickling, very light touch, or moving hairs on the skin. In animals, the tickle of a fly landingon the skin may cause a cow to kick, but the firm touch of the farmer's hands quiets her. Occupationaltherapists have observed that a very light touch alerts the nervous system, but deep pressure is relaxing andcalming.
Deep pressure touch has been found to have beneficial effects in a variety of clinical settings (Barnard and
Brazelton 1990, Gunzenhauser 1990). In anecdotal reports, deep touch pressure has been described toproduce a calming effect in children with psychiatric disorders. Deep pressure stimulation, such as rolling upin a gym mat, has been used to calm children with autistic disorder and ADHD (Ayres 1979, King 1989).
Lorna King (personal communication, 1990) reports that children with sleeping problems appear to sleep
better inside of a mummy sleeping bag, which adapts to fit the body snuggly. It also has been used to reducetactile defensiveness in children who cannot tolerate being touched. McClure and Holtz-Yotz (1991) foundthat deep pressure applied by foam-padded splints on the arms reduced self-injurious behavior and
self-stimulation in an autistic child.
Research on autistic children indicates that they prefer proximal sensory stimulation such as touching,
tasting, and smelling to distal sensory stimulation of hearing and seeing (Kootz et al. 1981). Autistic children
will often seek out deep pressure sensations. At various lecture meetings of parents of autistic individuals,parents have reported to me various types of pressure-seeking behavior of their offspring, such as wrappingarms and legs in elastic bandages, sleeping under many blankets even during warm weather, and getting undermattresses. In my case, I used to crawl under sofa cushions and have my sister sit on them. A high functioningautistic woman stated, "I need heavy blankets on me to sleep well, or else my muscles won't calm down."
Deep touch stimulation is beneficial to normal babies (Barnard and Brazelton 1990, Gunzenhauser 1990).
Institutionalized babies who received supplemental tactile stimulation, mainly deep touch pressure, devel-oped more normally (Provence and Lipton 1962). Premature babies who receive stroking and tightly boundswaddling also are reported to show definite benefits (Anderson 1986, Field et al. 1986, Lieb et al. 1980).
The strong need for deep touch stimulation is suggested in Harlow and Zimmerman's classic experiment
(1959): baby monkeys would cling to and press against a soft cloth mother surrogate which provided contact
comfort, over a wire surrogate that provided milk.
Takagi and Kobayasi (1955) found that deep pressure applied bilaterally to a person'a body results in a
decrease in pulse rate, metabolic rate, and muscle tone. This finding, however, has not been replicated.
Krauss (1987) designed an air mattress apparatus which applied pressure to large areas of the body. The
apparatus consisted of two air mattresses surrounded by a canvas wrap connected to a pulley. A person laying
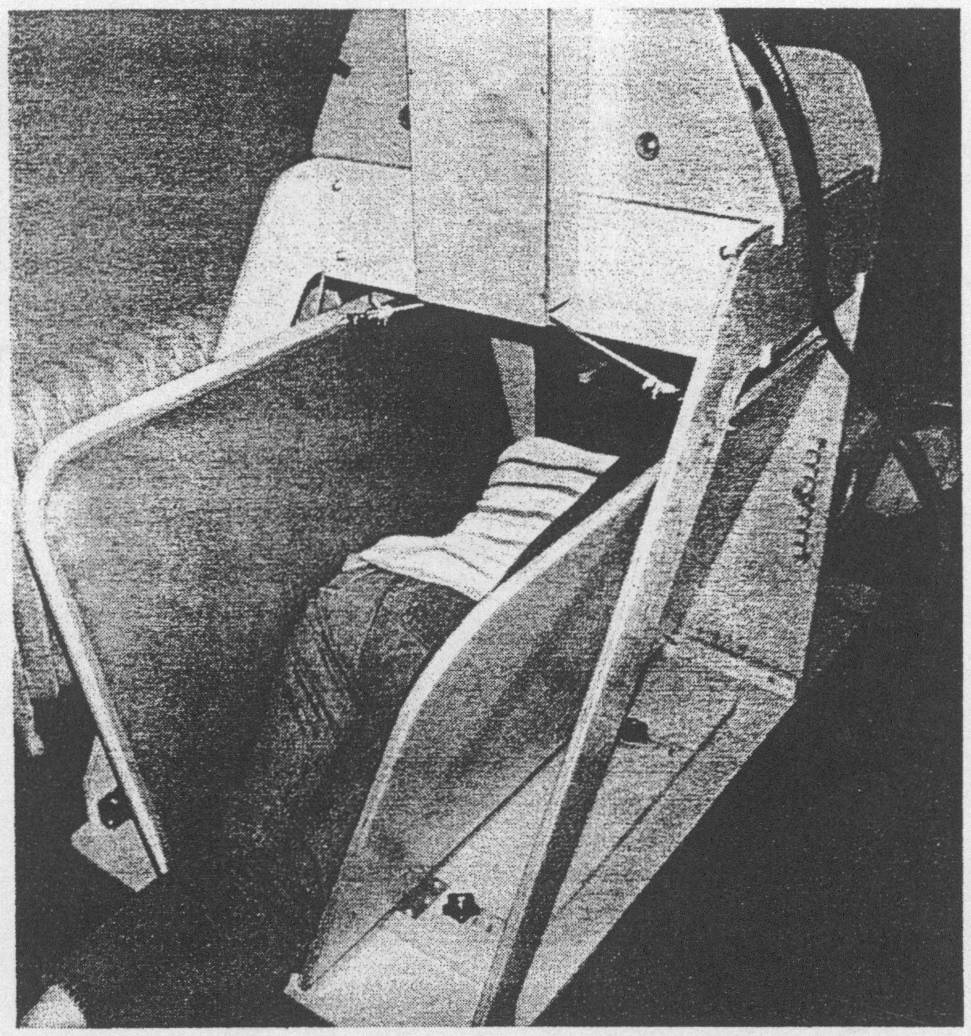
Rear view of the squeeze machine showing the position of the user between the padded side boards.
between the two mattresses could control pressure applied by pulling on a rope, which tightened the canvaswrap. In this study, college students reported mild subjective reductions in anxiety and were found to havemildly increased heart rate, but neither finding reached statistical significance. However, this rope-operatedapparatus applied considerably less pressure than the "squeeze machine" (Grandin 1984, Grandin andScariano 1986).
THE SQUEEZE MACHINE
The squeeze machine device developed by the author consists of two padded side boards which are hinged
at the bottom to form a V shape. The user steps into the machine and lies down on the inside in the V-shaped
crevicelike space. The inside surfaces of the device are completely lined with thick foam rubber. Deep touchpressure stimulation is applied along both sides of the person's body, with lateral pressure pushing inwardonto the body (Fig. 1). The V-shaped space supports the body fully from head to toe, so that the users cancompletely relax. The contoured padding provides an even pressure across the entire lateral aspects of the
body without generating specific pressure points. The foam-padded head rest and padded neck opening are
covered with soft fake fur. When the neck opening closes around the neck, it enhances the feeling of beingsurrounded and contained by the embrace of the deep touch pressure squeeze.
The user has complete control over the amount of pressure applied (Fig. 2). A lever-operated pneumatic
valve, which is connected to an air cylinder that pulls the side boards together, allows the user to self-regulatethe amount of pressure applied. For adults, the air pressure on the 5 cm diameter air cylinder is set at 60 psi,
which allows up to 43 kg (95 lbs.) of pressure to be exerted on each rope attached to the sides. For children
under age 8-9 years, the pressure is set at 30 to 40 psi.
The user can enter and leave the machine at will, which confers a more complete sense of self-control in the
context of the machine. The squeeze machine and procedures for its use are more fully described elsewhere(Grandin 1984, Grandin and Scariano 1986).
The advantage of the squeeze machine over other forms of deep pressure stimulation, such as rolling in
mats, is that the machine can apply greater amounts of pressure over larger areas of the body. The air cylinderpower applies constant pressure, even when the user shifts position.
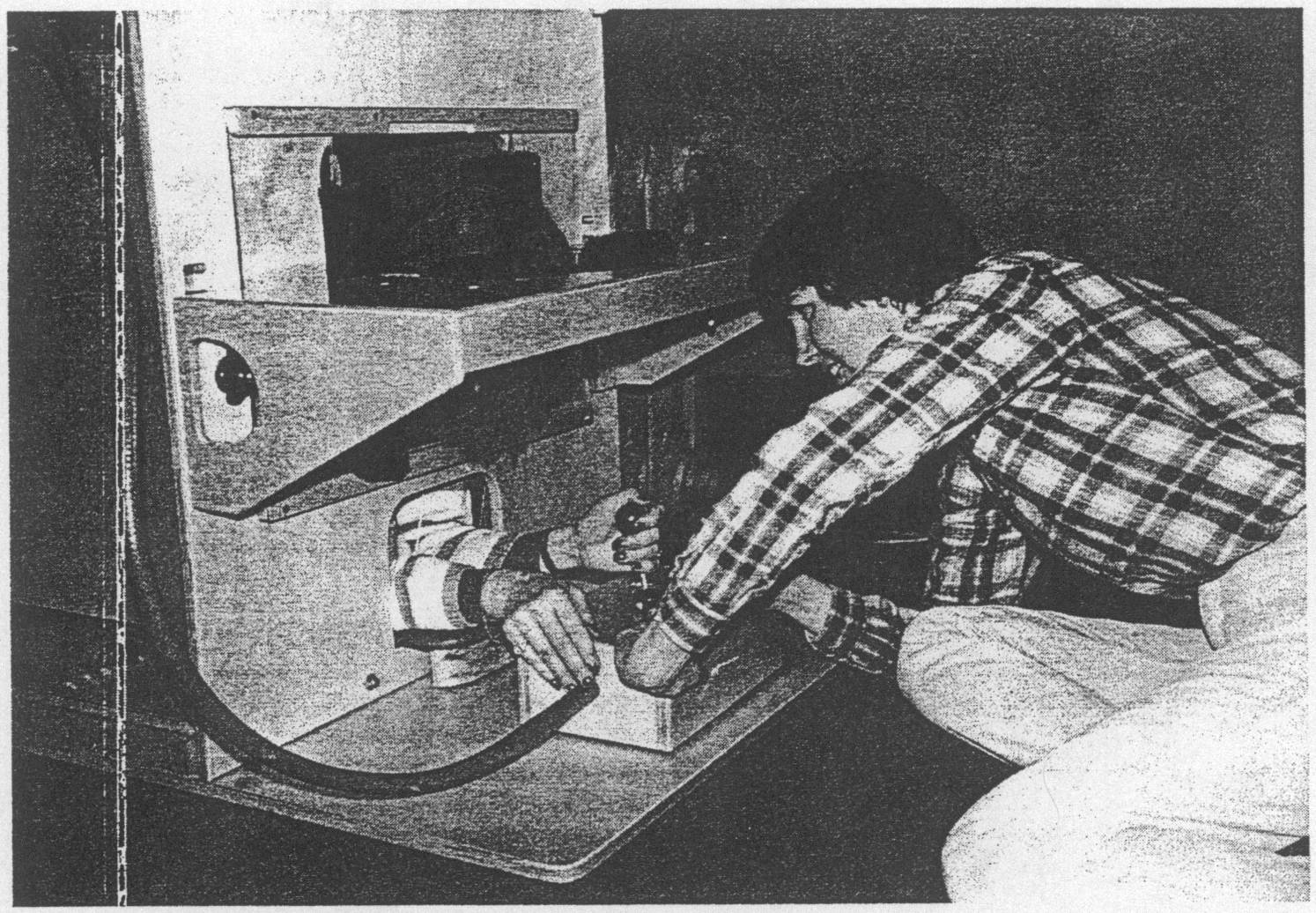
Front view of squeeze machine showing the user operating the control lever which activates the squeeze
THE AUTHOR'S EXPERIENCE WITH SQUEEZE MACHINE
As a child, I craved to feel the comfort of being held, but I would pull away when people hugged me. When
hugged, an overwhelming tidal wave of sensation flowed through me. At times, I preferred such intense
stimulation to the point of pain, rather than accept ordinary hugs. On the Ayres Checklist for TactileDefensiveness (1979), I had 9 out of 15 symptoms by age 10 years. Whenever anyone touched me, I stiffened,flinched, and pulled away. This approach-avoidance characteristic endured for years during my childhood.
At puberty, anxiety and nervousness made me feel as though I was constantly in a state of "stage fright."
While the nature of this anxiety was not diagnosed at the time, they have been retrospectively diagnosed aspanic attacks, and would fulfill the DSM-IH-R criteria.
At age 18,1 constructed the squeeze machine to help calm down the anxiety and panic attacks. Using the
machine for 15 minutes would reduce my anxiety for up to 45-60 minutes (Grandin and Scariano 1986). Therelaxing effect was maximized if the machine was used twice a day.
Gradually, my tolerance of being held by the squeeze machine grew. Knowing that I could initiate the
pressure, and stop it if the stimulation became too intense, helped me to reduce the oversensitivity of my"nervous system." A once overwhelming stimulus was now a pleasurable experience.
Using the machine enabled me to learn to tolerate being touched by another person. By age 25,1 was able
to relax in the machine without pulling away from it. It also made me feel less aggressive and less tense. SoonI noted a change in our cat's reaction to me. The cat, who used to run away from me now would stay with me,
because I had learned to caress him with a gentler touch. I had to be comforted myself before I could givecomfort to the cat.
As my "nervous system" calmed down, I required less squeeze pressure to produce a comforting feeling.
Gradually, I couid reduce the pressure regulator setting from 80 to 60 psi.
From my experiences, I learned that if pressure from the squeeze machine is applied at a steady pressure,
habituation wouid occur and discomfort would begin within 10 to 15 minutes. Instead, if the pressure isincreased and decreased slowly, the soothing effect could be maintained for up to one and a half hours. Veryslow movement of the squeeze sides was most soothing. Sudden jerky movements caused me to jump andbecome aroused. On most occasions, a 5—15 minute period in the machine was sufficient to get a goodresponse.
EFFECTS OF THE SQUEEZE MACHINE ON NORMAL ADULTS
Deep pressure applied to a wide area of the body, administered by the squeeze machine, has a relaxing
effect on normal adults. In the present study, college students were found to feel relaxed after use of the
squeeze machine. College students (18-25 years old) were not informed of the purpose of the squeezemachine, and simply were told that it was part of a sensory perception experiment. The operation of themachine was described to each student, and the author got into the machine to demonstrate its use. Eachstudent was tested individually to prevent students from influencing each other's response. After 5-10minutes, 45% (18/40) of the subjects employed words such as "relaxing" or "sleep" to describe their reactions.
Four students (10%) used the words "floating," "weightless," or "flight" to describe the sensation. Relaxationwas physically evident in some subjects. After being in the machine for a few minutes, the squeeze sides could
be pulled closer together without increasing the pressure setting.
Two people (5%) had a claustrophobic reaction to the machine and could not complete the experiment. For
40% of subjects, the machine appeared to have no relaxing effect.
Of the entire group, 25 students were asked, "If you could buy this machine in a store, what could you use
it for?" "Relaxer" or "tension reliever" was the response of 17 students. One student, who did not feelrelaxation after using the machine, suggested that it could be used as an isometric exerciser.
In a subgroup of 18 students, the squeeze machine was operated in three arbitrarily selected ways: (1)
stationary pressure, (2) fast rhythmic pulsation of 50 cycles per minute, and (3) slow rhythmic pulsation of 15cycles per minute. At the stationary setting, the tension on the ropes to the squeeze sides was 40 kg, a setting
that most adults find tight but comfortable. During the two pulsation modes, the pressure was reduced until thetop of the squeeze sides moved 1 cm on each side. After 5 minutes in the machine, each student was instructedto rate their state of relaxation on a scale from 1 ("almost asleep") to 10 ("very excited").
The data in Table 1 indicate that the stationary mode and the slow pulsation mode were more relaxing than
the fast mode.
I also have conducted some preliminary experiments that suggest that the squeeze machine may have an
effect on auditory threshold (Grandin 1970). This possibility was investigated in view of the findings that
cerebellar mechanisms might modify sensory inputs involving sound as well as touch.
USE OF THE SQUEEZE MACHINE IN TREATMENT OF CHILDREN
For the last 10 years, several occupational therapists and psychologists have used this squeeze machine with
autistic and hyperactive children. Six machines currently are being used for sensory integrative therapy, andbeneficial effects are being described anecdotally. Lorna King, Director of the Center for Neurodevelopmen-
tal Studies in Phoenix (Arizona) reports that the squeeze machine is useful for children with autistic disorder,
Relaxation Rating Scores Reported by College Students in the Squeeze Machine
Stationary pressure
Number of subjects
Number of subjects with rating below 6
Percentage of subjects with rating below 6
The squeeze machine was employed by 18 subjects using three arbitrarily selected modes: stationary pressure, slow
rhythmic pulsation of 15 cycles per minute, and fast rhythmic pulsation of 50 cycles per minute. Each subject experiencedall three settings, for 3 minutes in each mode, in random order during a 15 minute session. After experiencing each mode,subjects rated their state of relaxation on a scale of 1 (almost asleep) to 10 (very excited). An analysis of variance on the
entire sampling resulted in an F value
19.33 (p < 0.0001).
*To assess differences among the three modes, a Duncan's multiple range test was applied, using a
statistically significant difference was noted for relaxation ratings for Fast Pulsation, compared with ratings for either Slow
Pulsation or Stationary Pressure; these latter two modes were not different from one another.
attention-deficit hyperactivity disorder, or learning disabilities. Margaret Creedon at the Michael ReeseHospital in Chicago reports that children with pervasive developmental disorder (PDD) and children withTourette's disorder like to use the machine and that it calms them; it is claimed to help to inhibit tantrums andreduce stereotypies. However, there is a severe lack of formal research data pertaining to the clinical treatmentof children.
One study (Imamura et al. 1990) examined behavioral effects of the squeeze machine on 9 children, aged
3-7 years, with autistic disorder or PDD. Hyperactivity was found reduced in 4 subjects, and the machine hadno effect on 5 children. One child first began to hug the therapist after using the machine. The parents of a7-year-old, high-functioning autistic boy reported that they could tell the days on which he had used themachine by observing his calmness. When the squeeze machine was not available to him, this boy learned to
roll up in a quilt and then roll on the floor for 15 to 45 minutes every day to obtain adequate pressurestimulation.
Sessions with the machine were relatively unstructured, and usage usually was less than two minutes daily.
There appeared to be a relationship between longer duration of squeeze machine usage and beneficial effects.
Some children in their studies appear to have failed to use the squeeze machine long enough to have an effect.
Imamura et al. (1990) concluded that a more structured approach, designed to encourage greater use of themachine, probably would result in increased beneficial effects.
ANIMAL OBSERVATIONS
The author initially conceived of the idea for the squeeze machine from her observations in animal science.
Cattle being held in a squeeze chute, while waiting in line for veterinary attention, often appeared somewhatagitated during the waiting; some of the animals, however, seemed to relax once pressure was applied to largeareas of their bodies.
Deep pressure stimulation of diverse forms have been reported to have calming effects in a variety of
animals. For example, stroking and scratching the flank of a pig has long been known to induce inactivity
(Marcuse and Moore 1944), and pigs spontaneously seek body contact against a solid surface (Hartsock
1979). Pressure applied to both sides of a pig in a padded V-shaped trough will induce sleep and relaxation
(Grandin et al. 1989). In rabbits, gentle but firm pinching of the skin with padded clips will lead initially toarousal, followed by relaxed muscle tone, drowsiness, and deactivation of electroencephalogram (EEG)patterns (Kumazawa 1963). Likewise, a "squeeze machine" for chicks, constructed from hollowed-out foamrubber blocks, reduces separation distress (Jack Panksepp, Bowling Green University, personal communica-tion). In cats, rubbing and gentle pinching of a paw will decrease tonic activity in the dorsal column nuclei andsomatosensory cortex (Melzack et al. 1969).
In infant animals (and brain-damaged humans), pressure exerted on the face by an elastic bandage wrapped
around the head will override the vestibular system and cause the head to fall back (Teitlebaum 1977).
Wrapping a bandage around the torso of a cat causes the hind quarters to topple (Teitlebaum 1982).
The reactions of cattle to being restrained in a squeeze-restraining device are very similar to people in the
squeeze machine. Strong pressure initially causes cattle to relax, but will lead to struggling and discomfortwhen the animal habituates. Habituation occurs more quickly in cattle being held against unpadded metalsurfaces. Pressure must be decreased if the animal is held in a chute for more than two minutes.
Recently I operated a cattle-restraining chute that was fitted with hydraulic controls; these provide more
precise control over the amount of pressure and the speed of movement of the apparatus. Any sudden jerkymovement caused animals to jump and become agitated. If pressure was applied slowly, many animals wouldremain passive and not resist. Squeezing in a smooth steady motion, required less pressure to keep the animalstill. This chute was equipped also with a head restraint yoke, which would rise up under the animal's chin
after the body was restrained. Some cattle would fight the chin yoke by keeping their heads in a crooked
position, which made it impossible to restrain them fully. Sudden bumping often caused the animal to resist.
By gently pressing the yoke against them, I found that wild cattle would straighten their necks and place theirchin in the curved part of the yoke. When the animal moved into position, the pressure could be increased, and
the head was brought up into the restrained position with very little pressure. None of these animals pulledtheir head out of the yoke or even tried. At all times, pressure was applied firmly.
A wild horse may flinch and pull away from being touched by a human, similar to the reactions of some
autistic children to touch. In the process of taming a wild animal, animal trainers have learned that a firm touchcalms and a very light touch tends to excite, again similar to the clinical observations of occupational
The two main methods used to tame wild horses are forced holding and gradual taming. Forced holding is
quicker and more stressful than the somewhat slower gradual taming process.
Forced holding is similar to holding therapy for autistic children (Welch 1983). Gentler methods of holding
therapy are also effective for increasing eye contact and interest in humans (Powers and Thorworth 1985).
The forced holding procedure is done quietly and gently, and care is taken to avoid excitement. The horse
is securely tied or held in a livestock restraint device. The horse is held tightly and is unable to kick or thrash.
During the restraint period, the trainer strokes and pets all parts of the animal's body and talks to it gently.
Deep touching of every part of the animal's body is the key component of the taming procedure. The animal
is released once it is nonresisting. Sessions seldom last more than one hour. Good horse trainers use forcedholding only on very young animals. A significant disadvantage of this procedure is that forced restraint is
The taming approach is conducted more gradually. Horse trainers have found that nervous horses become
easier to handle if they are rubbed and brushed over all parts of their bodies (Tellington-Jones and Burns
1985). The horse may finch at first, but gradually will start to relax when stroked. Similar to the autistic child
who is initially aversive to touching and then finds that touching becomes pleasurable, a horse will show a
behavioral change such that a stimulus that was once actively avoided is now actively sought.
In animals, taming can proceed to the point of allowing the use of a deep touch pressure machine. Sheep can
be trained to enter a device similar to the squeeze machine repeatedly and voluntarily for pharmacological
studies (Grandin 1989). As with humans, the sheep were introduced gradually to the device. At first, the sheep
just stood in it, and subsequently pressure could be applied for increasing amounts of time.
SUGGESTIONS FOR THERAPISTS
In working with children, we have found that 5 minutes of sustained use of the squeeze machine is the
minimum typically required to obtain a readily detectable calming effect.
We would suggest that use of the machine should never be forced, though strong encouragement is needed
to overcome the approach-avoidance features associated with tactual defensiveness. Therapists who work
with factually defensive children find that they are better able to tolerate touching that they have initiated (Key
1989). At times, it is useful to encourage such a child to use the machine for at least the minimal 5 minutes in
order to ensure a noticeable effect. We have observed two basic ways that children and adults approach the
machine. The pressure, seeking type immediately will start using the machine, and use it readily with littleencouragement. CV>! W<fcn with attention-deficit hyperactivity disorder typically fit in this category. Incontrast, some autistic children have a high degree of tactual defensiveness, so that it is difficult for them toovercome their iniliil ¿Version to touch; they will require more encouragement. Use of the machine shouldnever be forced, but the. therapist must be "gently insistent" to coax a tactually defensive client to use it.
Clients should be (Jiscouraged from sudden jerking of the pressure on and off in rapid sequence. Some
people may want to increase and decrease the pressure slowly, which may help them to remain in the machinefor longer periods of time. The use of slowly varying deep touch pressure should be allowed.
Margaret Creedon (personal communication 1989) has suggested that users show two patterns: sustained
squeezers, and intermittent squeezers who continually squeeze it up and release it. It is possible that the
intermittent squeezers may have greater tactual defensiveness than sustained squeezers, and may needencouragement to leam to tolerate the pressure.
In teaching new users to operate the machine, it is important that the therapist who demonstrates the
machine really like to get in the machine. If he or she is uncomfortable or claustrophobic, the fear will be
communicated to the child. I often have induced a tactually defensive child to use the machine, even after
attempts by others had failed, because they could see that I enjoy it. For factually defensive children, the
therapist may need to demonstrate use of the machine repeatedly, so that they can see that it will not causethem harm. After the child becomes accustomed to the machine, he or she usually can use it voluntarilywithout further demonstration by the therapist.
It is essential that the machine is adjusted to properly fit the child. The side boards must be adjusted so that
the V-shape supports the body, but there still must be enough space for the child's knees. Proper adjustmentwill enhance the effect of the machine because the pressure will be applied more evenly.
Although the squeeze machine can be used for younger children, there are many easy methods for applying
deep pressure stimulation to children under the age of 5: rolling up in gym mats, "mat sandwiches," andresting under a pile of beanbag chairs. It is simply impossible to hold older children securely using thesealternative methods. Two holding therapy successes have been reported by parents, and both involved youngchildren (Randall and Randall 1989, Stribling 1989).
The squeeze machine may be most useful for older children or adults. In older children and adults, the
squeeze machine can apply considerable amounts of pressure. The device is also available for use at any time.
Older children and adults often feel embarrassed playing "children's games" with the therapist and prefer touse the squeeze machine in privacy.
Children with ADHD are often strongly attracted to the machine. There are suggestions that the use of the
machine may allow reduction in the dose of psychostimulant required to treat these children.
It appears that the squeeze machine may be beneficial to some children with autistic disorder or attention-
deficit hyperactivity disorder, and is of little value to others. Serious side effects appear to be minimal.
In treatment of children with autism, a very heterogeneous disorder, it is well-known that a treatment that
works for one individual may be useless for another. It is possible that the squeeze machine will be most
beneficial to those autistic people who have problems with oversensitivity to sensory stimulation. Theseproblems are perhaps due to an abnormality in the modulation of sensory inputs in several sensory modalities,
and may be related to structural abnormalities in lobules V, VI, and VII of the vermis of the cerebellumobserved in patients with autism. Some individuals with autism, who have greater cognitive problems andrelatively few sensory problems, may be less likely to benefit.
The possibility that use of the squeeze machine might allow dose reductions of psychostimulants, or
conceivably, other medications, is intriguing, but awaits formal demonstration.
At present, the squeeze machine should be considered a novel treatment that has not been subjected to
careful evaluation of clinical efficacy or safety. Preliminary observations in humans are encouraging, but the
data are inadequate to recommend routine use in clinical care. However, a calming response to deep touchstimulation appears to be characteristic of a diversity of animals, and may represent a relatively "physiolog-
ical" approach to sedation that has been overlooked by psychiatry researchers.
The squeeze machine can be obtained commercially for approximately $2000 from Therafin Corporation,
3800 South Union Avenue, Steger, Illinois 60475. Telephone: (708) 755-1535. Plans can also be obtainedfrom the author.
Ayres JA: Sensory Integration and the Child. Los Angeles, Western Psychological Services, 1979Anderson J: Sensory intervention with the preterm infant in the neonatal intensive care unit. Am J Occupational Therapy40:19-26, 1986
Barnard KE, Brazelton TB: Touch: The Foundation ofExperience. Madison (CT), International Universities Press, 1990Bauman M, KemperTL: Histoanatomic observations of the brain in early infantile autism. Neurology 35:866-874, 1985Chambers WW: Electrical stimulation of the interior of the cerebellum of the cat. Am J Anatomy 80:55-93, 1947
Courchesne E, Yeung-Courchesne R, Press GA, Hesselink JR, Jemigan TL: Hypoplasia of cerebellar vernal lobules VIand VII in autism. N Engl J Med 318:1349-1354, 1988Crispino L, TM Bullock: Cerebellum mediates modality specific modulation of sensory responses of midbrain andforebrain of rats. Proc Nati Acad Sei (USA) 81:2917-2929, 1984
Field TM, Schanberg SM, Scafidi F, Bauer CR, Vesa-Lahr N, Garcia R, Nystrom J, Kuhn CM: Tactile-kinestheticstimulation effects on preterm neonates. Pediatrics 77:654-658, 1986
Grandin T: Sensory interaction processes and the effect of pressure applied to the lateral body surfaces on auditorythresholds. Undergraduate thesis, Franklin Pierce College, Rindge, NH, 1970Grandin T: My experiences as an autistic child. J Ortho Molecular Psychiatry 13:144-174, 1984Grandin T: An autistic person's view of holding therapy. Communication 23:75-76, 1989a (Published by NationalAutistic Society of England)Grandin T: A voluntary acceptance of restraint by sheep. Appl Animal Behav Sei 23:257-261, 1989Grandin T, Scariano MM: Emergence Labeled Autistic. Novato, CA, Arena Press, 1986Grandin T, Dodman TN, ShusterL: Effect of naltrexone on relaxation induced by lateral flank pressure in pigs. Pharmacol
Biochem Behav 33:839-842, 1989
Gunzenhauzer N (ed): Advances in Touch: New Implications in Human Development. Skillman (NJ), Johnson & JohnsonConsumer Products, Inc., 1990
Harlow HH, Zimmerman RR: Affectional responses in the infant monkey. Science 130:421-432, 1959
Hartsock TG: Maladaptive behaviors of piglets weaned at 12 hours postpartum (abstract). J Animal Sei 49 (Suppl):47,
Imamura KN, Wiess T, Parham D: The effects of hug machine usage on behavioral organization of children with autismand autistic-like characteristics. Sensory Integra Quarterly 27:1-5, 1990King L: Facilitating neurodevelopment. Autism Society of America, Conference Proceedings, Seattle (Washington), July
KootzJP, MarinelliB, Cohen DJ: Sensory receptor sensitivity in autistic children. Arch Gen Psychiatry 38:271-273, 1981Krauss KE: The effects of deep pressure on anxiety. Am J OccupTher 41:366-373, 1987Kumazawa T: "Deactivation" of the rabbit's brain by pressure application to the skin. Electroencephalog ClinNeurophysiol 15:660-671, 1963Lieb SA, Benfield G, Guidubaldi J: Effects of early intervention and stimulation on the preterm infant. Pediatrics66:83-89, 1980
Ornitz E: Neurophysiology of infantile autism. J Amer Acad Child Psychiatry 24:251-262, 1985Marcuse FL, Moore AU: Tantrum behavior in the pig. Journal of Comparative Psychology 37:235-241, 1944McClure MK, Holtz Yotz M: The effects of sensory stimulatory treatment on an autistic child. Amer J OccupationalTherapy 45:1138-1142, 1991Nyhan WL: Behavior in the Lesch-Nyhan Syndrome. J Autism Child Schizophr 6:381-389, 1976
Powers MD, Thorworth CA: The effect of negative reinforcement on tolerance of physical contact in a preschool autisticchild. J Clin Psychol 14:299-303, 1985Provence S, Lipton RC: Infants in Institutions. New York, International Universities Press, 1962Randall G, Randall P: Communication 23:57, 1989
Ritvo E, Freeman BJ, Scheibel AB, Duong T, Robinson H, Guthrie D, Ritvo A: Lower purkinje cell count in the cerebellaof four autistic subjects: Initial findings of the UCLA-NSAC autopsy research report. Am J Psychiatry 143:862-866, 1986Stribling P: Communication 23(2):56-57, 1989Takagi K, Kobayasi S: Skin pressure vegetative reflex. Acta Medical et Biológica 4:31-57, 1955Teitlebaum P: Levels of integration of the opérant. In: Handbook of Opérant Behavior. Edited by Honig WK, StaddonJER. New York, Academic Press, 1977
Teitlebaum, P: Disconnection and antagonistic interaction of movement subsystems and motivated behavior. In:
Changing Concepts of the Nervous System, Academic Press, New York, 1982
Tellington-Jones L, Bums U: The Tellington Jones Equine Awareness Method. Millwood, NY, BreakthroughPublications, 1985
Welch MG: Retrieval from autism through mother child holding therapy. In: Autistic Children: New Hope for a Cure.
Edited by Tinbergen N, Tinbergen EA. London, Allan & Unwin, 1983
Address reprint requests to:
Temple Grandin, Ph.D.
Department of Animal Science
Colorado State University
Fort Collins, CO 80526
This article has been cited by:
1. S. Barry, E. A. O'Sullivan, K. J. Toumba. 2014. Barriers to dental care for children with autism spectrum disorder. European
Archives of Paediatric Dentistry 15:2, 127-134. []
2. Kym Maclaren. 2014. Touching matters: Embodiments of intimacy. Emotion, Space and Society . []3. LOUISA GRANDIN SYLVIA, LEAH W. SHESLER, ANDREW D. PECKHAM, TEMPLE GRANDIN, DAVID A.
KAHN. 2014. Adjunctive Deep Touch Pressure for Comorbid Anxiety in Bipolar Disorder. Journal of Psychiatric Practice
4. Nicole Cottam, Nicholas H. Dodman, James C. Ha. 2013. The effectiveness of the Anxiety Wrap in the treatment of
canine thunderstorm phobia: An open-label trial. Journal of Veterinary Behavior: Clinical Applications and Research 8:3,
5. Laura C. Erickson, Ashley A. Scott-Van Zeeland, Gavin Hamilton, Alan Lincoln, Beatrice A. Golomb. 2013. Erratum to:
Brief Report: Approaches to 31P-MRS in Awake, Non-Sedated Children With and Without Autism Spectrum Disorder.
Journal of Autism and Developmental Disorders
6. Tonya N. Davis, Sharon Dacus, Erica Strickland, Daelynn Copeland, Jeffrey Michael Chan, Kara Blenden, Rachel Scalzo,
Staci Osborn, Kellsye Wells, Krisann Christian. 2013. The effects of a weighted vest on aggressive and self-injurious behavior
in a child with autism. Developmental Neurorehabilitation 1-6. []
7. Balazs Toth, Monica Aleman, Robert J. Brosnan, Peter J. Dickinson, Alan J. Conley, Scott D. Stanley, Nora Nogradi,
Colette D. Williams, John E. Madigan. 2012. Evaluation of squeeze-induced somnolence in neonatal foals. American Journal
of Veterinary Research 73:12, 1881-1889. []
8. Cynthia A. PekowBasic Experimental Methods in the Rabbi9. Patricia Cody, Lori Holleran Steiker, Mary Lynn Szymandera. 2011. Equine Therapy: Substance Abusers' "Healing
Through Horses". Journal of Social Work Practice in the Addictions 11:2, 198-204. []
10. R COOPER, B DICIANNO, B BREWER, E LOPRESTI, D DING, R SIMPSON, G GRINDLE, H WANG. 2008.
A perspective on intelligent devices and environments in medical rehabilitation☆. Medical Engineering & Physics 30:10,
11. Brian Mullen, Tina Champagne, Sundar Krishnamurty, Debra Dickson, Robert X. Gao. 2008. Exploring the Safety and
Therapeutic Effects of Deep Pressure Stimulation Using a Weighted Blanket. Occupational Therapy in Mental Health 24:1,
12. Mary L. Schneider, Colleen F. Moore, Lisa L. Gajewski, Julie A. Larson, Andrew D. Roberts, Alexander K. Converse,
Onofre T. DeJesus. 2008. Sensory Processing Disorder in a Primate Model: Evidence From a Longitudinal Study of Prenatal
Alcohol and Prenatal Stress Effects. Child Development 79:1, 100-113. []
13. Sharon Blairs, Susan Slater, Dougal Julian Hare. 2007. The clinical application of deep touch pressure with a man with
autism presenting with severe anxiety and challenging behaviour. British Journal of Learning Disabilities 35:4, 214-220.
14. Michelle O'Riordan, Filippo Passetti. 2006. Discrimination in Autism Within Different Sensory Modalities. Journal of
Autism and Developmental Disorders 36:5, 665-675. []
15. Eric SchoplerCross-Cultural Program Priorities and Reclassification of Outcome Research Methods 1174-1189. []16. Temple GrandinA Personal Perspective of Autism 1276-1286. []17. Grace T. Baranek, L. Diane Parham, James W. BodfishSensory and Motor Features in Autism: Assessment and Intervention
18. Edmund Frank Lopresti, Alex Mihailidis, Ned Kirsch. 2004. Assistive technology for cognitive rehabilitation: State of the
art. Neuropsychological Rehabilitation 14
19. Sandra J. Weiss, Peggy Wilson, Delmont Morrison. 2004. Maternal Tactile Stimulation and the Neurodevelopment of Low
Birth Weight Infants. Infancy 5
20. Temple GrandinAutism 409-417. []21. L. EUGENE ARNOLD. 2001. Alternative Treatments for Adults with Attention-Deficit Hyperactivity Disorder (ADHD).
Annals of the New York Academy of Sciences 931
22. P. Howlin. 1997. Prognosis in autism: do specialist treatments affect long-term outcome?. European Child & Adolescent
23. Temple Grandin. 1996. Brief report: Response to national institutes of health report. Journal of Autism and Developmental
24. Temple Grandin, Matthew B. Rooney, Megan Phillips, Richard C. Cambre, Nancy A. Irlbeck, Wendy Graffam. 1995.
Conditioning of nyala (Tragelaphus angasi) to blood sampling in a crate with positive reinforcement. Zoo Biology 14:3,
Source: http://sensorycalm.com.au/wp-content/uploads/2014/07/Temple-Grandin-Study.pdf
Revista Brasileira de Farmacognosia Brazilian Journal of Pharmacognosy Anti-hyperlipidemic activity of oryzanol, isolated from crude rice bran oil, on Triton WR-1339-induced acute hyperlipidemia in Somsuvra B. Ghatak, Shital J. Panchal* Department of Pharmacology, Institute of Pharmacy, Nirma University, India.
My Health, My Choice, My Child, My Life! Women demand the roll out of a comprehensive national action plan to end vertical transmission of HIV in India Globally, momentum has been built to reinvigorate efforts to reduce maternal and infant mortality and improve maternal health including for women living with HIV. Nationally, women and children have been the stated priority of the government HIV programme since the beginning. The Indian Constitution guarantees the right to equality for all women and the right to life and health of all. In order to succeed in meeting these goals, civil society, especially women and mothers living with HIV, must be engaged and listened to, as we know the ground realities in the communities we live and work in.

