Pseudotumor cerebri im kindes und jugendalter
Intracranial hypertension
Daniel Tibussek, MD
• Case• Clinical presentation of pediatric PTC• Nomenclature, Definition
– What is intracranial hypertension?– Diagnostic difficulties
• Epidemiology of headache in PTC
– Clinical course of headache– IIH without papilledema
• Cases continued• Summary
• 13 yrs, female, obese• History of intermittend headache, tension-
type, for > 1 year
• Blurred vision since 6 wks,
problems reading black board at school
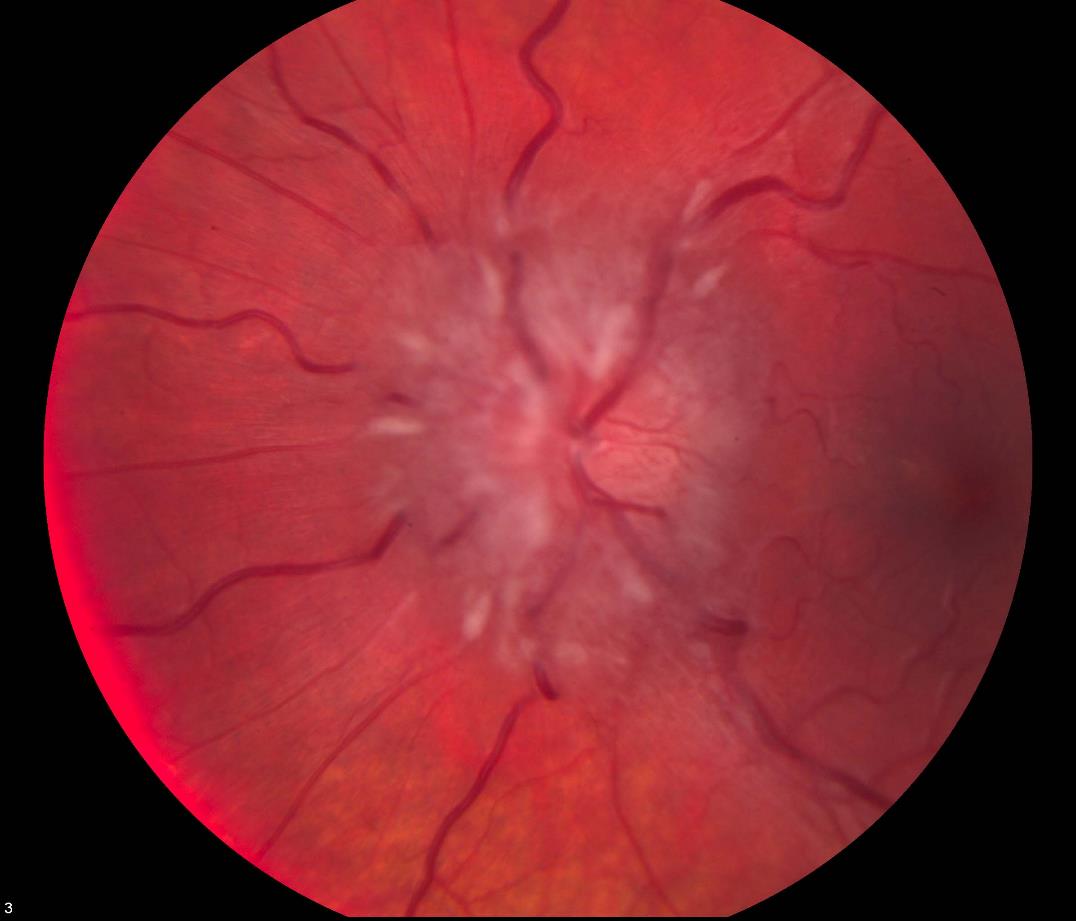
• Ophthalmology:
bilateral papilledema, reduced visualacuity, visual fields normal
• LP: CSF OP 21 cm H2O
• prompt improvement of headache
• normalisation of visual disturbances within
days post LP, improved papilledema
• No treatment b/o normal CSF OP.
• 2 months later: again blurred vision, vertigo,
headache, worse than previously
• CSF OP 24 cm H2O, post LP again rapid
improvement of vision
• Put on acetazolamide (20 mg/kg/d)• Normalisation of papilledema• Persisting headache, chronic daily• Furosemide added, increasingly tired, no
appetite, persisting headache, misses weeks ofschool
What is Pseudotumor
Pseudotumor cerebri
Mishra A et al. Eur J Paediatr Neurol 2007 ; 11 : 39 – 42
Colin Kennedy (Editorial) Dev Med Child Neur 2006;48:83-83
Are children any different?
Clinical presentation: adults,
• „Headache is the most common symptom
of IIH present in 80%-90% of patients"Julayanont et al. 2016
• Headache are the predominat feature of
the disease, reported by around 75-94%Markey et al. 2016
• „Headache is clearly the major symptom"
Johnston et al. 2007
• Highly heterogenous, migraine-like, often daily
PTCS as incidental finding
out of 61 children
• Düsseldorf:
16 out of 53 children
Literature: • Lim et al.
• Bassan et al.
Tibussek et al. Klin Padiatr. 2013;225:81-5Tibussek et al. Child Nerv Syst 2010; 26:313-21Lim et al. Arch Dis Child 2005; 90:206–210Bassan et al. Acta Neurol Scand. 2008 Oct;118(4):251-5
Headache patterns in PTCS: Duesseldorf
Lewis DW. Am Fam Physician 2002; 65:625–632Tibussek et al. Childs Nerv Syst 2010;26:313-21
„seroese Meningitis"
"otitic hydrocephalus"
Benign Intracranial Hypertension
Pseudotumor Cerebri
Idiopathic Intracranial Hypertension
Pseudotumor cerebri Syndrome/complex
Definition of Pseudotumor
• A. Papilledema• B. Normal neurologic examination except for
cranial nerve abnormalities
• C. Neuroimaging: Normal brain parenchyma• D. Normal CSF composition• E. Elevated lumbar puncture opening pressure
Adapted from: Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology; 2013;81:1159–1165.
Definition of Pseudotumor
• A. Papilledema >> IIHWOP!!!• B. Normal neurologic examination except for
cranial nerve abnormalities
• C. Neuroimaging: Normal brain parenchyma• D. Normal CSF composition• E. Elevated lumbar puncture opening pressure
Adapted from: Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebrisyndrome in adults and children. Neurology; 2013;81:1159–1165.
Definition of Pseudotumor
• A. Papilledema• B. Normal neurologic examination except for
cranial nerve abnormalities
• C. Neuroimaging: Normal brain parenchyma• D. Normal CSF composition• E. Elevated lumbar puncture opening pressure
Add Reference Imaging!Adapted from: Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebrisyndrome in adults and children. Neurology; 2013;81:1159–1165.
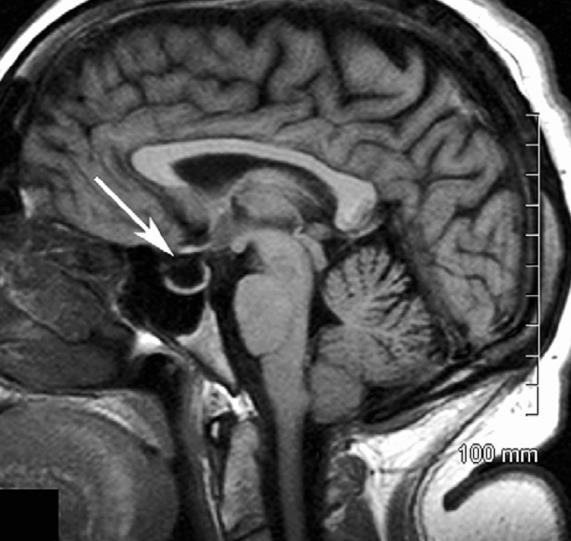
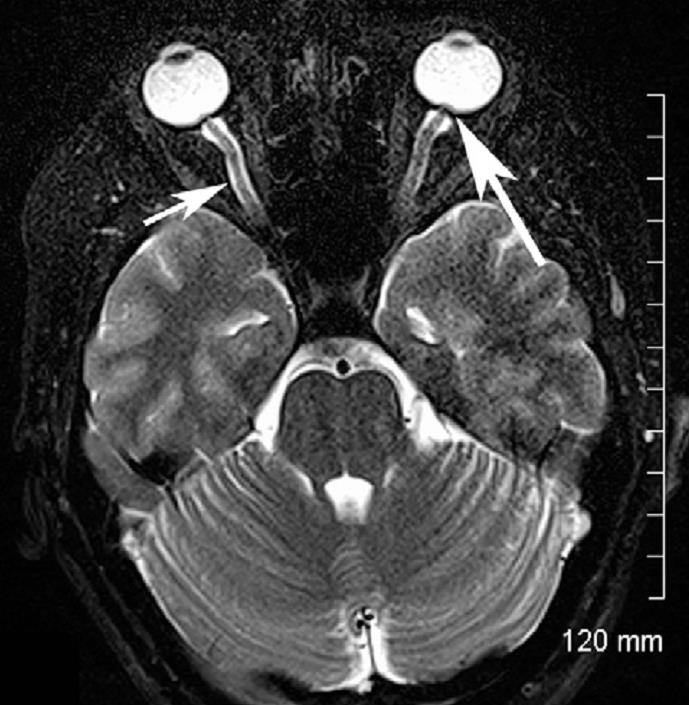

Maralani et al. Clinical Radiology 2012; 67:656-663
Definition of Pseudotumor
• A. Papilledema• B. Normal neurologic examination except for
cranial nerve abnormalities
• C. Neuroimaging: Normal brain parenchyma• D. Normal CSF composition• E. Elevated lumbar puncture opening pressure• BUT: what is elevated opening pressure?
Adapted from: Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology; 2013;81:1159–1165.
Opening Pressure Distribution (N = 197)
(Opening Pressure cm H O)
Avery et al. N Engl J Med 363;891-3
Still, this is not the
final answer.
Diagnostic Criteria for
Pseudotumor Cerebri Syndrome
• Elevated lumbar puncture opening
pressure (>250 mm CSF in adults and >280 mm CSF in children)
• [250 mm CSF if the child is not sedated
and not obese])
• Our case: < 25 mm H2O
Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology; 2013;81:1159–1165.
CSF opening pressure
< 28 cm H O
• Germany: 13/61 PTCS pediatrics patients
• Duesseldorf: 14/75 PTCS pediatric patients
• This represents 18% of the total
pediatric PTCS study population
• PTCS diagnosis possible with OP < 28 cm• There is NO cutoff value for normal CSF
Tibussek et al. Eur J Paediatr Neurol. Under revision. Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology; 2013;81:1159–1165.
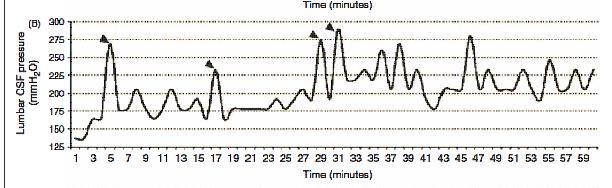
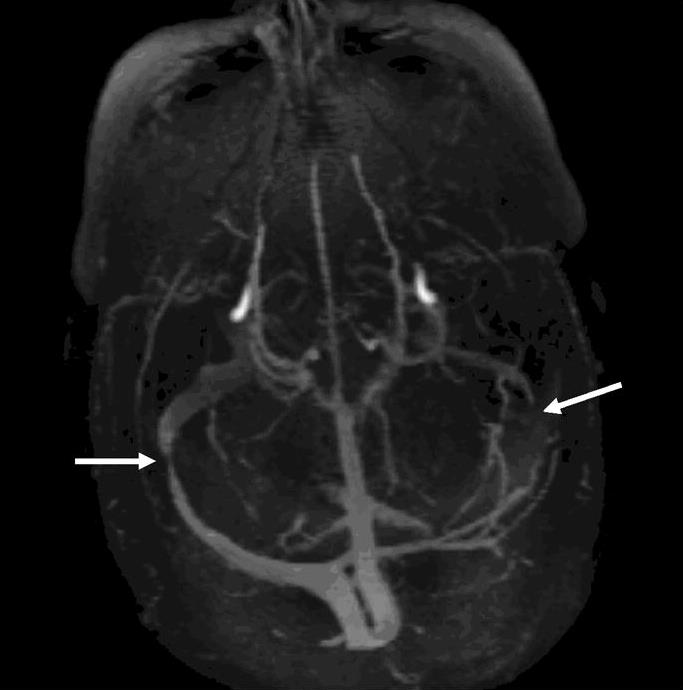
!Pressure variability in 1 h!
- Bilateral transverse sinus stenosis- Initial LP Opening pressure < 20cm
Cephalalgia 2010 30:1419-25
IIHWOP: Does it exist?
„idiopathic intracranial hypertension
(IIH) without Papilloedema"
Kelly et al. Clin Neurol Neurosurg. 2013 Aug; 115(8): 1215–1219.
Chronic migraine and PTCS
• Has been linked to PTCS in adults• Has been linked to transverse sinus
• Has been linked to IIH without papilledema
Transverse sinus stenosis
(TSS) in PTCS patients
• Is almost always bilateral!• Degree of stenosis does NOT correlate
with the clinical course
• Clinical features, not the degree of TSS,
should be used to determine managementin IIH /PTCS
Riggeal et al. Neurology. 2013;80:289-295
An indication for stenting?
To stent or not to stent?
Julayanont et al. Journal of Pain Research 2016:9 87-99
publication bias!
• Venous peforation• Subdural hemorrhage• Stent migration• In-stent thrombosis• Recurrent stenosis• Long-term antithrombotic treatment• …
Headache in treated PTCS
• N=82• 68% developed subsequent headacheEpisodic tension type
Migraine w/o aura
Chronic tension type
Analgesic overuse headache
Friedman D, Rausch E. Neurology. 2002 May 28;58(10):1551-3.
„Patients with PTCS
…despite the apparent normalization of their intracranialpressure"
Friedman D, Rausch E. Neurology. 2002 May 28;58(10):1551-3.
An indication for stenting?
„We do not usually recommend surgicaltreatment or venous stenting for patientswith isolated chronic headaches and mild tomoderate papilloedema without visual loss"„because of high prevalence of associatedprimary headache disorders and the frequent development of chronic headacheunrelated to raised ICP make the success … too unpredictable"
Anne Ducros and Valerie Biousse in Lancet Neur 2015;14:655-68
What are our treatment goals?
1) Maintain/regain normal visual
2) Relief headaches
3) prevent unneccesary invasive
• Still normal vision, no papilledema• Headache still reported• Follow-up LP, OP 28 cm H²O• Interpreted as treatment resistence• Scheduled for VP-shunt
Interpretation and
• „probable PTCS" (OP <25 cm H2O)• Response to LP very suggestive of PTCS• Good response to treatment (Vision)• f/u LP with increased OP falsely
interpreted as treatment resistence
• Clinical deterioration due to medication
• Headache not PTCS related
Sir William Osler, 1st Baronet (born July 12, 1849 – December 29, 1919) was a
Canadian physician and one of the four founding professors of Johns Hopkins
Hospital (Wikipedia).
• After cessation of furosemid prompt
clinical improvement
• Back to school• Referral to headache progam (multimodal
• Gradually improving headache• Still remission, normal eye exam• No neurosurgery
Therapy-Escalation:
„treatment decisions should not rest
on … the severity of papilledema, or
CSF opening or closing pressure."
„Instead, the modern management of
pseudotumor cerebri is based largely
upon the level of visual loss."
Aus: Liu et al.: Neuro-Ophthalmology. Diagnosis and Management. Second edition. 2010
• N=24, female adults with PTCS• Quality of life is significantly reduced in
• Headache was the only clinical outcome
that correlates with enhanced QOL
• Effective headache management is
required to improve QOL in PTCS!
Mulla et al. J Headache Pain. 2015;16:521.
Headache as criteria for success?
• A „classical" patient shows rapid headache
Bruce BB, Biousse V, Newman NJ. Am J Ophthalmol 2011;152:163-169Friedman DI, Rausch A. Neurology 2002; 58:1551-1553
Headache as criteria for success?
• A „classical" patient shows rapid headache
Bruce BB, Biousse V, Newman NJ. Am J Ophthalmol 2011;152:163-169Friedman DI, Rausch A. Neurology 2002; 58:1551-1553
Headache as criteria for success?
• A „classical" patient shows rapid headache
Bruce BB, Biousse V, Newman NJ. Am J Ophthalmol 2011;152:163-169Friedman DI, Rausch A. Neurology 2002; 58:1551-1553
Headache as criteria for success?
• A „classical" patient shows rapid headache
„Many IIH patients have
persistent headaches,
even after normalization
of the intracranial pressure"
„Patients with IIH frequently have
headaches not necessarily related to
increased intracranial pressure"
Bruce BB, Biousse V, Newman NJ. Am J Ophthalmol 2011;152:163-169Friedman DI, Rausch A. Neurology 2002; 58:1551-1553
Therapy, little evidence
Update 2015:Although the two included RCTs showed modest benefits for acetazolamide for some outcomes, there is insufficient evidence to recommend or reject the efficacy of this intervention, or any other treatments currently available, for treating people with IIH.
the use of acetazolamide with a low-sodium
weight reduction diet, compared with diet
alone, resulted in modest improvement in
visual field function.
No significant treatment effects were noted
with respect to headache disability
Step-wise approach
Step 3: No visual loss:
- Symptomatic headache (migraine) therapy
Step 4: Mild visual loss:
- Acetazolamide- Furosemide- (Topiramate) - Weight reduction, if necessary
Liu et al. 2011 in: Neuro-Ophthalmology, Diagnosis and Management, Saunders, Elsevier
Step-wise approach
Step 3: No visual loss:
- Symptomatic headache (migraine) therapy- weight loss
Although plausible, no evidence
Step 4: Mild visual loss:
that topiramate is superior when
- Acetazolamide- Furosem
- Weight reduction, if necessary
Liu et al. 2011 in: Neuro-Ophthalmology, Diagnosis and Management, Saunders, Elsevier
• Step 5: Severe, or progression of visual
Always critically question your
- Optic nerve sheath decompression
diagnosis before even considering!
(ONSD) - High-dose IV steroids and acetazolamide - Lumboperitoneal shunt for failed ONSD or intractable headache- Bariatric surgery
Do not forget: Differential
Elevated CSF opening pressure in Pediatric Demyelinating Disease Cohort:
„Almost 1/3 of children with inflammatorydemyelinating disease have an elevatedCSF opening pressure"
Pediatric Neurology 2015;52:446-449
• Optimal management of IIH requires good
communications between specialties to protect the patient from unnecessary lumbar punctures and CSF diversion surgery on the one hand and avoidable visual loss on the other.
Standridge SM. Idiopathic intracranial hypertension in children: A review and algorithm. Pediatr Neurol 2010;43:377-390.
Take home message
• The doubtless diagnosis of PTCS is difficult!• Exclusion of papilledema should always be
part of headache work-up
• Beware of pseudopapilledema!• If MRI appears indicated do high quality MRV• Relevance of transverse sinus stenosis in
children unclear.
• However, bilateral TSS suggestive of PTCS• Frequency of IIHWOP in children is unknown
Take Home Messages
• Headache may or may not improve after LP
even in proven PTCS cases
• Headache may or may not respond to pressure
lowering medication on follow-up
• Headache is not a good monitoring instrument
• Persisting headache after treated PTCS is
common in children and adults
• Persisting headache does not neccesarily
indicate treatment resistence of PTCS
• Beware of medication induced headache
Take home messages
• Critically question diagnosis BEFORE
invasive treatment.
• PTCS needs to be treated in a
• PTCS should usually not be considered a
Intracranial pressure monitoring.
• Lumbar Puncture Opening Pressure Is Not
a Reliable Measure of Intracranial Pressure in Children. Journal of Child Neurology 2015, Vol. 30(2) 170-173.
• „Lumbar puncture therefore significantly
overestimates the intracranial pressure in children."
Step-wise approach
• Step 1: correct potentially causal factors
(medication, anaemia, hypothyroidism, .)
• Step 2: LP with CSF drainage to lower
pressure >> measure post punctional pressure („closing pressure")
Pressure release as the only
„Interestingly, it is not uncommon to observe a
lasting clinical remission after a single lumbar puncture in some IIH patients"
Germany study
• 14/61 Patients got LP pressure as the only
treatment. In 1 case succesfully as serial LP.
Bruce BB, Biousse V, Newman NJ. Update on Idiopathic Intracranial Hypertension. Am J Opthalmol 2011;152:163-169
Source: http://www.pseudotumor-cerebri.de/Intracranial%20Hypertension-Tibussek-Amsterdam%202016%20short.pdf
The Power of Not Asking: How Do Generic Drug Substitution Laws Affect Patient's Demand for Generic Drugs? 1 Yan Song2 Douglas Barthold 3 Current Version: Nov/9/2015 Substituting generic for brand drugs whenever possible has been proposed as an effective way to control pre-scription drug expenditure growth in the United States. This work investigates whether mandatory switchingand presumed consent laws are effective in increasing generic drug use. The analysis uses plausibly exoge-nous changes in states' drug substitution policies for identification. The Difference-in-Difference regressionresults indicate that mandatory switching laws have little effect. However, presumed consent laws, wherebythe pharmacists could assume patients' consent to switch to generic drugs, reduce consumers' probability ofpurchasing brand drugs by 4.1 percentage points. We construct and estimate a bounded rationality modelto explain why presumed consent laws work. In the model, consumers in states with presumed consent lawsincur a cost when asking pharmacists for brand drugs. We find that presumed consent laws' effect in de-creasing brand drug use is equivalent to increasing the brand drug price by 3 dollars. The average marginaleffect of the policy is to reduce the probability of purchasing brand drugs by 6 and 11 percent. A welfarecalculation indicates that consumers' surplus loss exceeds the insurances' gain by 7.5 dollars per person perpurchase when states switch from explicit to presumed consent laws.
IJREAS VOLUME 5, ISSUE 8 (August, 2015) (ISSN 2249-3905) International Journal of Research in Engineering and Applied Sciences (IMPACT FACTOR – 5.981) King of Desert (Prosopis) : A source of potential medicinal values in Arid Zone of India: Review Dr.Surbhi Rajvanshi1, Dr.Veena Garg2

